Fractured Neck of Femur: Expert Guide to Diagnosis & Management
Introduction & Epidemiology
A fractured neck of femur (NOF) represents a critical orthopedic presentation, characterized by its high incidence and significant associated morbidity and mortality. Globally, hip fractures account for a substantial burden on healthcare systems, with estimated annual numbers exceeding 1.6 million, a figure projected to rise dramatically with an aging global population. In the United Kingdom alone, over 65,000 hip fractures are recorded annually, reflecting an escalating frequency directly attributable to demographic shifts toward older demographics.
The public health implications extend beyond incidence, encompassing the profound impact on patient outcomes. Femoral neck fractures carry a one-year mortality rate approaching 30%, a sobering statistic that underscores the inherent vulnerability of this patient cohort and the critical need for specialized, multidisciplinary care. This necessitate a structured approach, with many orthopedic units now integrating dedicated orthogeriatric services to optimize pre-operative assessment, peri-operative management, and post-operative rehabilitation for these complex patients.
Etiologically, NOF fractures primarily arise from two distinct injury mechanisms. The most prevalent are low-energy injuries , typically falls from standing height in osteoporotic older adults, which often occur with minimal trauma dueic fragility. Conversely, high-energy injuries , such as those sustained in road traffic collisions or falls from significant heights, are less common but tend to affect younger individuals and are frequently associated with polysystem trauma, necessitating comprehensive polytrauma protocols.
This review will provide an in-depth exploration of the surgical anatomy, biomechanics, classification systems, clinical and radiological diagnosis, and evidence-based management strategies for femoral neck fractures, including detailed surgical techniques, potential complications, and rehabilitation principles.
Surgical Anatomy & Biomechanics
Gross Anatomy of the Proximal Femur
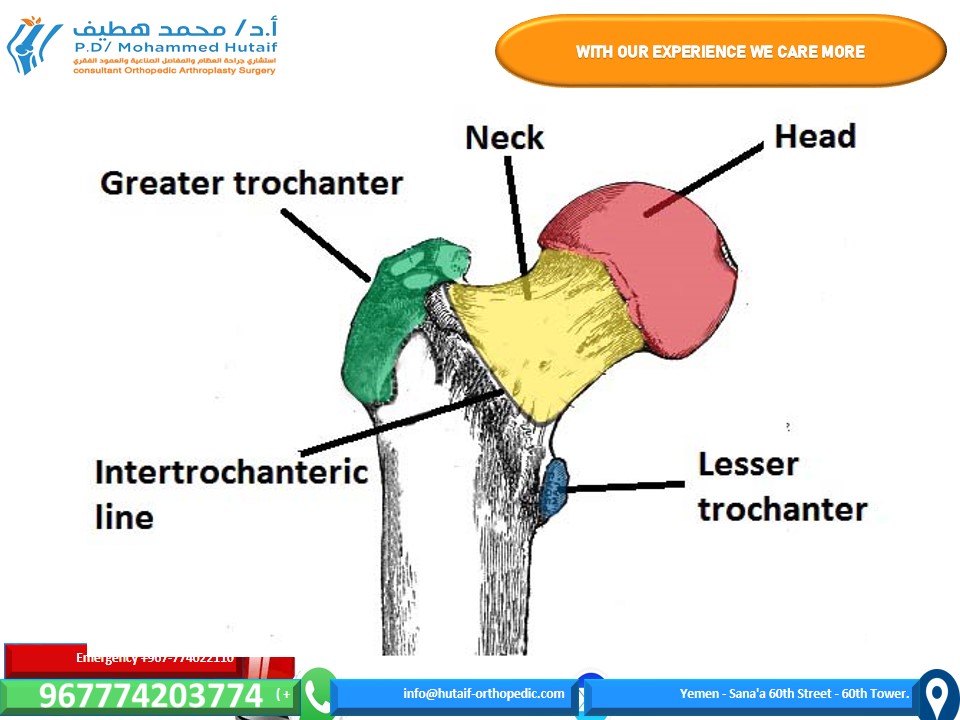
The proximal femur, critical to hip function and common site of fracture, encompasses the femoral head, neck, and trochanteric region. Neck of femur fractures are anatomically defined as occurring from the subcapital region of the femoral head distally to 5 cm below the lesser trochanter. This broad definition encompasses a spectrum of fracture patterns with distinct biomechanical and clinical implications.

Figure 1 – The bony landmarks of the anterior proximal femur
For surgical planning and prognostication, the femoral neck is broadly categorized into two distinct anatomical regions relative to the hip joint capsule:
- Intracapsular fractures: These occur from the subcapital region of the femoral head through the transcervical region to the basocervical area, immediately proximal to the trochanters. Fractures within this region are contained by the synovial fluid and are more prone to complications such as avascular necrosis (AVN) due to disruption of the primary blood supply.
- Extracapsular fractures: These occur distal to the capsular insertion, typically involving the intertrochanteric or subtrochanteric regions. While often grouped clinically as "hip fractures," their management and prognosis differ significantly from intracapsular fractures. This review primarily focuses on intracapsular and basocervical fractures of the femoral neck.
Vascular Supply of the Femoral Head
The vascularity of the femoral head is paramount in understanding the pathophysiology and prognosis of intracapsular NOF fractures. The primary blood supply to the femoral head is derived from the medial circumflex femoral artery (MCFA) and, to a lesser extent, the lateral circumflex femoral artery (LCFA) , both branches of the deep femoral artery (profunda femoris).

These arteries form an extracapsular arterial ring at the base of the femoral neck. From this ring, retinacular arteries ascend along the femoral neck within the synovium, perforating the bone primarily in the posterosuperior and posteroinferior aspects to supply the femoral head and neck. The artery of the ligamentum teres (foveal artery) , a branch of the obturator artery, provides a variable and often insufficient supply, particularly in adults, becoming more critical following primary blood supply disruption.
Intracapsular fractures, especially displaced subcapital fractures, critically disrupt the retinacular vessels, compromising the blood supply to the femoral head. This vascular insult is the primary determinant in the high incidence of femoral head avascular necrosis (AVN) and non-union following internal fixation of displaced intracapsular fractures.
Biomechanics of the Femoral Neck
The femoral neck is a cantilever beam, subjected to significant bending and shear forces during weight-bearing. Its structural integrity is maintained by a complex trabecular architecture designed to withstand these stresses:
- Primary Compressive Trabeculae: Extend from the medial cortex of the femoral shaft to the superomedial aspect of the femoral head.
- Primary Tensile Trabeculae: Arc from the lateral cortex of the femoral shaft to the inferomedial aspect of the femoral head.
- Secondary Compressive/Tensile Trabeculae: Contribute to overall strength.
- Ward's Triangle: A region of relatively sparse trabeculae in the central femoral neck, which is often the first area to show osteopenic changes, increasing susceptibility to fracture.
Fracture patterns are influenced by the direction of the applied force relative to the femoral neck axis. The
Pauwels classification
specifically addresses the angle of the fracture line relative to the horizontal plane, directly correlating with the shear forces experienced at the fracture site:
*
Pauwels Type I:
<30 degrees (primarily compressive forces, relatively stable).
*
Pauwels Type II:
30-50 degrees (increased shear, moderately stable).
*
Pauwels Type III:
>50 degrees (predominantly shear forces, inherently unstable).
Higher Pauwels angles predict a greater risk of non-union and implant failure due to increased shear stress at the fracture interface.
Indications & Contraindications
Clinical Presentation and Initial Assessment
Patients typically present after a fall, complaining of severe hip pain, inability to bear weight, and often exhibit a classic deformity: a shortened and externally rotated lower extremity. In non-displaced or impacted fractures, the deformity may be subtle or absent, and patients may still be able to ambulate, albeit with pain. Initial assessment should include:
*
Primary Survey:
Rule out life-threatening injuries, especially in high-energy trauma.
*
Secondary Survey:
Detailed history (mechanism, comorbidities, medications, pre-injury functional status, cognitive assessment), comprehensive physical examination.
*
Pain Management:
Early and effective analgesia is crucial, often involving systemic medications and regional nerve blocks (e.g., fascia iliaca block).
Radiological Diagnosis and Classification
- Standard Radiographs: Anteroposterior (AP) pelvis and AP/lateral views of the affected hip are the initial imaging modalities. These typically suffice for diagnosing displaced fractures.
- Occult Fractures: In cases of strong clinical suspicion with equivocal plain radiographs, further imaging is mandated. Magnetic Resonance Imaging (MRI) is the gold standard for detecting occult NOF fractures, including bone bruising. Computed Tomography (CT) scans may be used if MRI is contraindicated or unavailable, offering good visualization of fracture patterns and comminution.
Fracture Classification Systems
Accurate classification is critical for guiding management and prognostication.
*
Garden Classification (Displacement-based):
Most widely used for intracapsular NOF fractures, categorizing displacement and impaction.
*
Garden I:
Incomplete or impacted valgus fracture.
*
Garden II:
Complete, non-displaced fracture.
*
Garden III:
Complete, partially displaced fracture (often varus, with some remaining trabecular alignment).
*
Garden IV:
Complete, completely displaced fracture (no trabecular alignment between head and neck).
*

*
Pauwels Classification (Angle of Fracture Line):
As discussed, classifies fractures based on the angle of the fracture line to the horizontal, reflecting biomechanical stability.
*
AO/OTA Classification:
A comprehensive system based on fracture location (e.g., 31-B for femoral neck), morphology, and severity. While more detailed, its complexity sometimes limits its routine clinical application for NOF fractures compared to Garden.
Operative vs. Non-Operative Indications
The vast majority of femoral neck fractures, particularly displaced patterns, require surgical intervention. Non-operative management is reserved for highly selected cases.
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Indications |
-
Displaced Fractures (Garden III/IV):
Nearly all require surgery.
- Non-Displaced Fractures (Garden I/II): Generally recommended due to high risk of displacement (up to 30%) and AVN. - Young, Active Patients (<60-65 years): Priority for head preservation via internal fixation. - Elderly, Active Patients (>=60-65 years) with Displaced Fractures: Arthroplasty (Hemiarthroplasty or THA) is the preferred treatment. - High Functional Demand: THA considered in appropriate elderly patients. |
-
Medically Unfit for Surgery:
Patients with severe comorbidities (e.g., ASA V) where the risk of surgery outweighs potential benefits.
- Non-Ambulatory/Pre-Existing Low Functional Status: Patients who are bed-bound or severely demented with minimal pre-injury mobility. - Imminent Death/Palliative Care: End-of-life care where comfort is the primary goal. - Impacted Valgus Fractures (Garden I) in Very Selected Patients: Rare, stable, and requires strict non-weight-bearing and vigilant radiographic follow-up for potential displacement (often still fixed due to displacement risk). |
| Contraindications |
-
Absolute:
Medically unstable for any intervention, patient refusal, non-viable limb.
- Relative: Severe osteoporosis precluding stable fixation (consider arthroplasty), uncontrolled infection (delay surgery if possible). |
-
Functional Patient:
Non-operative management will lead to prolonged pain, malunion, non-union, or AVN, severely impacting mobility and quality of life.
- Displaced Fractures: High risk of poor outcomes, often leads to revision surgery. |
| Goals |
- Restore anatomy and function.
- Preserve femoral head (in younger patients). - Facilitate early mobilization. - Minimize pain and complications. |
- Comfort and palliation.
- Avoid surgical risks in very frail patients. - Pain management with minimal mobility. |
Pre-Operative Planning & Patient Positioning
Pre-Operative Assessment and Optimization
A comprehensive pre-operative evaluation is paramount, particularly for the elderly cohort. This involves:
*
Medical Optimization:
Collaboration with orthogeriatricians, internists, and anesthesiologists to address comorbidities (cardiac, pulmonary, renal, neurological function), optimize medication regimens, and manage delirium risk.
*
Nutritional Assessment:
Malnutrition is common and associated with poorer outcomes; interventions should be considered.
*
Delirium Screening:
Baseline cognitive assessment and strategies for delirium prevention (e.g., early mobilization, avoiding deliriogenic medications, sensory aids).
*
Imaging Review:
Meticulous review of radiographs to assess fracture pattern, displacement, bone quality, and identify any pre-existing hip pathology. Templating for arthroplasty is essential to determine implant size and type.
*
Informed Consent:
Detailed discussion with the patient and/or surrogate regarding treatment options, risks (including AVN, non-union, infection, dislocation), and expected outcomes.
*
Timing of Surgery:
Evidence supports early surgical intervention (within 24-48 hours) to reduce mortality, length of hospital stay, and complication rates, provided the patient is medically stable.
Anesthesia and Pain Management
- Anesthetic Choice: Spinal, epidural, or general anesthesia. Spinal anesthesia is often preferred in elderly patients due to potentially lower rates of delirium and VTE, though choice depends on patient comorbidities and surgeon preference.
- Regional Nerve Blocks: Fascia iliaca compartment block or pericapsular nerve group (PENG) block can provide excellent pre- and post-operative analgesia, reducing opioid requirements and improving early mobilization.
Patient Positioning
The choice of patient position depends on the planned surgical approach and fixation method.
*
Supine Position on a Traction Table:
Commonly used for internal fixation with cannulated screws or dynamic hip screw (DHS) systems, and for direct anterior approach (DAA) or anterior approaches to arthroplasty.
*
Advantages:
Allows for controlled reduction with traction and internal rotation, easy fluoroscopic access in multiple planes.
*
Setup:
The affected leg is placed in traction, often with the foot taped to a traction boot. The contralateral leg is often abducted and flexed to allow perineal access. Adequate padding of all pressure points (sacrum, heels, perineum) is critical to prevent skin breakdown and nerve compression.
*
Lateral Decubitus Position:
Standard for posterior (posterolateral) or anterolateral approaches for hemiarthroplasty or total hip arthroplasty.
*
Advantages:
Excellent exposure of the posterior aspect of the hip joint and proximal femur, often preferred for revision cases.
*
Setup:
Patient positioned on the unaffected side with axillary roll, hip and knee flexed on the affected side, secured with bean bag or dedicated hip positioners. Careful padding of the dependent arm, leg, and sacrum.
Prophylaxis
- Antibiotic Prophylaxis: Administered pre-incision according to local guidelines (e.g., Cefazolin).
- Venous Thromboembolism (VTE) Prophylaxis: Mechanical (compression stockings, intermittent pneumatic compression devices) and pharmacological (low molecular weight heparin or direct oral anticoagulants) prophylaxis initiated pre- or post-operatively and continued for several weeks.
Detailed Surgical Approach / Technique
The choice of surgical technique depends on patient age, functional status, fracture displacement (Garden classification), bone quality, and surgeon preference. The primary treatment options are internal fixation (IF) or arthroplasty (hemiarthroplasty or total hip arthroplasty).
Internal Fixation (IF) - For Garden I/II and Select Garden III in Younger Patients
Internal fixation aims to preserve the femoral head, making it the preferred option for younger, active patients (generally <60-65 years) and for non-displaced or impacted fractures in older individuals.
- Patient Positioning: Supine on a traction table is standard.
-
Reduction:
This is the most critical step. The goal is anatomical or near-anatomical reduction, often described as "anatomical reduction is mandatory, non-anatomical is catastrophic."
- Traction and Internal Rotation: Apply longitudinal traction to the affected leg, followed by internal rotation and slight abduction to disimpact and correct the typical external rotation and shortening deformity.
-
Fluoroscopic Guidance:
Antero-posterior (AP) and lateral fluoroscopic views are essential to confirm reduction.
- AP View: Ensure continuity of Shenton's line and restoration of the neck-shaft angle (approximately 130-135 degrees). The lesser trochanter should not be prominently visible (indicates excessive external rotation).
- Lateral View: The most reliable indicator of adequate reduction is the "cross-table" or "true lateral" view. Look for restoration of the anterior and posterior cortical continuity of the femoral neck. A common pitfall is residual posterior sag or displacement, which is poorly seen on a standard lateral.
-
Reduction Maneuvers:
- Leadbetter Maneuver: Hip flexed, internally rotated, and abducted.
- "Heel-palm" Maneuver: Direct pressure over the greater trochanter with the heel of the hand while applying traction and internal rotation.
-
Fixation (Cannulated Screws):
Typically, three 6.5 or 7.3 mm cannulated screws are used in an inverted triangular configuration.
-
Guide Wire Placement:
- The first guide wire is typically placed centrally or slightly anterior-inferior in the femoral neck, aiming for the subchondral bone of the femoral head. It should be parallel to the anterior cortex in the lateral view.
- The second wire is placed superiorly.
- The third wire is placed inferiorly.
- All wires should be parallel to each other and equidistant, forming an inverted triangle. They should reach within 5-10 mm of the subchondral bone in the femoral head for optimal purchase but avoid joint penetration.
- Screw Length and Insertion: Measure the length of each guide wire. Drill and insert appropriate length cannulated screws. Compression can be applied across the fracture site by partial threading of the screws or use of washers.
- Final Fluoroscopy: Confirm satisfactory screw placement, reduction, and absence of joint penetration in all views.
-
Guide Wire Placement:

Arthroplasty (Hemiarthroplasty or Total Hip Arthroplasty) - For Displaced Fractures in Older Patients
Arthroplasty is the treatment of choice for displaced intracapsular NOF fractures in most elderly patients (generally >60-65 years), due to the high rates of AVN and non-union with internal fixation in this demographic.
-
Hemiarthroplasty:
Replaces the femoral head with a prosthetic component, articulating with the native acetabulum.
- Indications: Elderly patients with displaced NOF fractures, low functional demand, or significant comorbidities.
-
Types:
- Unipolar: A single prosthetic femoral head articulates directly with the acetabulum.
- Bipolar: A smaller femoral head articulates within a polyethylene-lined metallic shell, which then articulates with the acetabulum. This theoretically reduces wear on the native acetabular cartilage, but long-term benefits over unipolar are debated.
-
Approach (Posterior/Posterolateral):
Most common.
- Incision: Curved incision centered over the greater trochanter, extending proximally and distally.
- Dissection: Split the gluteus maximus fibers. Identify and incise the fascia lata.
- External Rotator Tenotomy: Transect the short external rotators (piriformis, gemelli superior and inferior, obturator internus) close to their insertion on the greater trochanter, preserving their nerve supply if possible. Tag these for later repair.
- Capsulotomy: Incise the posterior hip capsule, typically in a T-shape or H-shape. Dislocate the femoral head (often already dislocated or easily removed).
- Femoral Preparation: Neck osteotomy using a cutting guide, typically at a 45-degree angle to the femoral shaft, at the level of the lesser trochanter. Ream and broach the femoral canal sequentially to fit the chosen femoral stem (cemented or uncemented).
- Implant Insertion: Insert the chosen stem. Attach the trial head and perform a trial reduction to assess stability, range of motion, and leg length.
- Final Implantation: Secure the definitive femoral head component.
- Closure: Repair the capsule and external rotators meticulously to reduce dislocation risk. Layered soft tissue closure.
- Approach (Anterolateral/Direct Anterior): Can also be used, with specific advantages regarding soft tissue preservation or dislocation risk (DAA).
-
Total Hip Arthroplasty (THA):
Replaces both the femoral head and the acetabulum with prosthetic components.
- Indications: Active elderly patients with displaced NOF fractures, particularly those with pre-existing acetabular pathology (e.g., osteoarthritis, severe acetabular cartilage damage), or those with high functional demands. THA generally provides superior functional outcomes and lower re-operation rates than hemiarthroplasty in selected patients.
- Technique: Similar to hemiarthroplasty for femoral preparation. Additionally involves acetabular reaming, placement of an acetabular cup (cemented or uncemented), and insertion of a polyethylene liner. Trial reduction and assessment of stability, leg length, and offset are critical.
Internervous Planes and Nerve Protection
Regardless of the approach, meticulous attention to internervous planes and nerve protection is crucial:
*
Posterior Approach:
Risk to the sciatic nerve (most commonly with excessive retraction or cement extrusion).
*
Anterolateral Approach:
Risk to the superior gluteal nerve (supplying gluteus medius/minimus, resulting in Trendelenburg gait if injured) and lateral femoral cutaneous nerve (LFCN, resulting in meralgia paresthetica).
*
Direct Anterior Approach:
Risk to the LFCN and femoral nerve, particularly with strong retraction.
Complications & Management
Complications associated with femoral neck fractures and their surgical management are frequent and can significantly impact patient outcomes. They can be broadly categorized into general medical complications and specific orthopedic complications.
General Medical Complications
These are common in the elderly, frail population sustaining NOF fractures:
*
Delirium:
Up to 50% incidence. Risk factors include advanced age, pre-existing cognitive impairment, polypharmacy, and surgical stress.
*
Management:
Prevention is key: early mobilization, pain control, hydration, correction of metabolic disturbances, avoid deliriogenic drugs, sensory aids, quiet environment. Pharmacological intervention (e.g., haloperidol) for agitation.
*
Venous Thromboembolism (VTE):
Deep vein thrombosis (DVT) and pulmonary embolism (PE) incidence can be high without prophylaxis.
*
Management:
Pharmacological (LMWH, DOACs) and mechanical prophylaxis (TEDs, IPCs) initiated early and continued for 4-6 weeks post-op. Early mobilization.
*
Infection (UTI, Pneumonia, Wound):
Increased susceptibility due to age, immobility, and surgical insult.
*
Management:
Prophylactic antibiotics, early mobilization, pulmonary hygiene, Foley catheter removal ASAP.
*
Pressure Injuries:
Due to prolonged immobility pre- and post-operatively.
*
Management:
Frequent repositioning, pressure-relieving mattresses, skin care.
*
Cardiac/Pulmonary Decompensation:
Common in patients with pre-existing cardiovascular or respiratory disease.
*
Management:
Pre-operative optimization, close peri-operative monitoring, judicious fluid management.
Specific Orthopedic Complications
| Complication | Incidence (Approx.) | Salvage Strategy |
Surgical Site Infection (SSI)
- Hemi-arthroplasty/THA: Typically 1-2% but can be as high as 5-10% in high-risk patients.
- Internal Fixation: <1% for clean cases.
-
Management:
- Acute (within weeks of surgery): Irrigation and debridement (I&D) with component retention (hemi/THA), exchange of modular components, prolonged IV antibiotics based on culture results. If persistent, 2-stage revision (implant removal, spacer, antibiotics, then re-implantation).
- Chronic (months-years post-op): Often requires 2-stage revision arthroplasty. For internal fixation, hardware removal and debridement, followed by conversion to arthroplasty if non-union or AVN is present.
Avascular Necrosis (AVN) of the Femoral Head (Internal Fixation)
- Incidence: 10-30% for displaced NOF (Garden III/IV) treated with IF. Lower for non-displaced.
-
Management:
- Early/Pre-collapse: Core decompression, vascularized fibular graft (controversial).
- Post-collapse: Conversion to hemiarthroplasty or total hip arthroplasty (THA).
Non-Union (Internal Fixation)
- Incidence: 10-20% for displaced NOF treated with IF. Higher with poor reduction, inadequate fixation, or delayed surgery.
- Management: Conversion to hemiarthroplasty or THA.
Malunion (Internal Fixation)
- Incidence: Varies, generally lower than non-union. Can lead to pain, limb length discrepancy, or impingement.
- Management: Corrective osteotomy (rare), conversion to THA if symptomatic and debilitating.
Screw Cutout/Perforation (Internal Fixation)
- Incidence: <5%, typically due to poor screw placement or secondary displacement.
- Management: Revision of fixation (if early), or conversion to arthroplasty.
Dislocation (Arthroplasty)
- Incidence: 2-10%, higher with posterior approach, poor soft tissue repair, patient non-compliance, or revision surgery.
-
Management:
- Closed Reduction: Urgent closed reduction under sedation/anesthesia.
- Revision Surgery: If recurrent or irreducible, consider revision of components, constrained liner, or soft tissue procedures.
Periprosthetic Fracture (Arthroplasty)
- Incidence: <1-5%, often intra-operative or post-operative due to trauma or falls.
- Management: Varies based on Vancouver classification (location, stability of implant, bone quality). Options include open reduction and internal fixation (ORIF), revision of components, or combination.
Aseptic Loosening (Arthroplasty)
- Incidence: Long-term complication. Higher with uncemented stems in poor bone quality or with poor cementing technique.
- Management: Revision arthroplasty.
Leg Length Discrepancy (Arthroplasty)
- Incidence: Up to 30%, often perceived by the patient even with small differences.
- Management: Shoe lifts for minor discrepancies. Revision arthroplasty for significant, symptomatic cases.
Nerve Injury (Arthroplasty/IF)
- Incidence: <1-2%. Sciatic, femoral, lateral femoral cutaneous, superior gluteal nerves are at risk.
- Management: Prevention (careful dissection and retraction), close monitoring, neurological consultation, physiotherapy. Often managed conservatively.
Post-Operative Rehabilitation Protocols
Early, aggressive, and individualized rehabilitation is crucial for optimizing functional recovery and reducing complications following femoral neck fracture surgery. A multidisciplinary approach involving orthopedic surgeons, orthogeriatricians, physical therapists (PT), and occupational therapists (OT) is essential.
Immediate Post-Operative Period (Days 0-7)
- Pain Management: Multimodal analgesia, including regional blocks, oral opioids, NSAIDs (if not contraindicated), and acetaminophen.
-
Mobilization:
- Day 0-1: Out of bed (OOB) to chair, passive/active-assisted range of motion (ROM) exercises for the operated hip, ankle pumps, gluteal sets.
-
Weight-Bearing (WB) Status:
- Internal Fixation: Usually partial weight-bearing (PWB) or touch-down weight-bearing (TDWB) initially, progressing as fracture healing dictates, typically over 6-12 weeks. This can vary based on fracture stability and surgeon preference.
- Hemiarthroplasty/THA: Typically full weight-bearing (FWB) as tolerated immediately, provided the fixation (cemented stem) or stability (uncemented stem, THA) is secure.
- Ambulation: With assistance (walker, crutches) as tolerated, focusing on proper gait mechanics.
- DVT Prophylaxis: Continue pharmacological and mechanical prophylaxis.
- Delirium Management: Continue prevention strategies.
- Wound Care: Daily inspection, dressing changes.
Intermediate Rehabilitation (Weeks 1-12)
-
Physical Therapy:
- Strengthening: Progressive resisted exercises for hip abductors, extensors, flexors, and core musculature. Quadriceps and hamstring strengthening.
- Range of Motion: Continue active and passive ROM exercises to prevent contractures.
- Gait Training: Progression from assistive devices to independent ambulation as strength and balance improve. Focus on normalized gait pattern.
- Balance Training: Single-leg stance, tandem stance, dynamic balance exercises.
-
Occupational Therapy:
- Activities of Daily Living (ADLs): Training for self-care (dressing, bathing, toileting) and household tasks.
- Adaptive Equipment: Prescription and training for assistive devices (long-handled reachers, sock aids, raised toilet seats).
- Home Safety Assessment: Identification and modification of fall hazards in the home environment.
- Hip Precautions (Post-Arthroplasty): Strictly enforced for posterior approach (avoid hip flexion >90 degrees, adduction past midline, internal rotation). Modified or no precautions for anterolateral or direct anterior approaches, depending on surgeon preference and capsular repair.
Long-Term Rehabilitation (Beyond 12 Weeks)
- Progression of Activity: Gradual return to pre-injury activities, emphasizing low-impact exercises.
- Fall Prevention: Continued education, home safety, balance exercises, assessment for osteoporosis and treatment if indicated.
- Bone Health Management: All patients, particularly older adults, should be evaluated for osteoporosis and initiated on appropriate medical management (e.g., bisphosphonates, calcium, Vitamin D) to prevent future fragility fractures.
- Follow-up: Regular clinical and radiological follow-up to monitor implant integrity, bone healing, and overall function.
Summary of Key Literature / Guidelines
The management of femoral neck fractures is guided by a robust body of evidence and international guidelines, emphasizing early intervention and patient-centered care.
-
Timing of Surgery: Numerous studies and meta-analyses consistently demonstrate that surgery within 24-48 hours of presentation is associated with reduced mortality, lower rates of post-operative complications (e.g., pneumonia, delirium), and shorter hospital stays, irrespective of the surgical method. This urgency applies once the patient is medically optimized.
- Reference example: Simunovic et al. (2010) in BMJ showed that delay to surgery significantly increased 30-day mortality.
-
Role of Orthogeriatric Co-management: Integrated orthogeriatric care models have proven superior to traditional care, leading to reduced mortality, shorter length of stay, lower rates of medical complications, and improved functional outcomes. This multidisciplinary approach addresses the complex medical needs of older adults with fragility fractures.
- Reference example: National Institute for Health and Care Excellence (NICE) guidelines strongly recommend orthogeriatric co-management for hip fracture patients.
-
Internal Fixation vs. Arthroplasty for Displaced Fractures in the Elderly: For displaced intracapsular NOF fractures in patients aged 65 and older, arthroplasty (hemiarthroplasty or THA) is the preferred treatment. Studies consistently show significantly lower re-operation rates, lower rates of AVN and non-union compared to internal fixation.
-
Hemiarthroplasty vs. THA:
- The HEALTH trial (2019) , a large multinational RCT, compared hemiarthroplasty to THA for displaced femoral neck fractures in active older adults. It found that THA resulted in better functional outcomes and a lower rate of re-operation for any cause at 24 months, at the expense of a higher initial complication rate.
- The PROFHER study (2015) also supported THA over hemiarthroplasty for active older patients.
- Current Consensus: THA is generally recommended for active, cognitively intact older patients with displaced NOF fractures and low pre-existing comorbidity. Hemiarthroplasty remains a viable option for less active patients or those with significant comorbidities, offering a quicker and less demanding procedure.
- Reference example: The American Academy of Orthopaedic Surgeons (AAOS) and NICE guidelines provide strong recommendations based on these trials.
-
Hemiarthroplasty vs. THA:
-
Cemented vs. Uncemented Hemiarthroplasty: For hemiarthroplasty, cemented femoral stems have demonstrated superior outcomes, including lower rates of periprosthetic fracture, less thigh pain, and better long-term survival, particularly in osteoporotic bone.
- Reference example: Parker et al. (2010) Cochrane review.
-
Management of Non-Displaced Fractures: While internal fixation (typically cannulated screws) is the standard for non-displaced or impacted femoral neck fractures (Garden I/II), there is a recognized risk of secondary displacement (up to 30%). Close radiographic monitoring is essential for non-operative cases, but surgical fixation is generally favored even in non-displaced fractures due to this risk.
- Reference example: FAITH trial (2017) explored internal fixation in young patients but highlighted challenges in displaced fractures.
-
Osteoporosis Management: Recognizing that NOF fractures are often fragility fractures, comprehensive secondary prevention of osteoporosis is critical. All patients should undergo bone mineral density assessment and receive appropriate pharmacological treatment (e.g., bisphosphonates, denosumab, teriparatide) and nutritional supplementation (calcium, Vitamin D) to reduce the risk of future fractures.
- Reference example: International Osteoporosis Foundation (IOF) and National Osteoporosis Foundation (NOF) guidelines emphasize this.
In conclusion, effective management of fractured neck of femur requires a holistic approach, integrating prompt diagnosis, timely and appropriate surgical intervention, rigorous complication management, and comprehensive orthogeriatric-led rehabilitation, all underpinned by strong evidence-based principles to optimize outcomes in this challenging patient population.
