Background
Forequarter amputation (interscapulothoracic amputation) entails en bloc removal of the upper extremity together with the scapula and the lateral aspect of the clavicle. This mutilating amputation of the upper extremity was traditionally done for high-grade sarcomas around the proximal humerus and scapula.
Tumor response to chemotherapy and radiation therapy and the option of endoprosthetic reconstruction have made these procedures rare, and limb-sparing resections are safe alternatives in 90% to 95% of these cases.
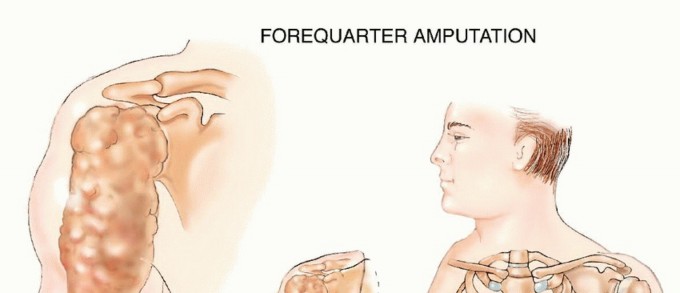
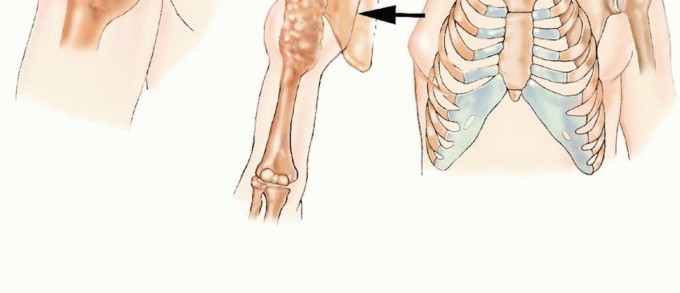
FIG 1: Forequarter amputation entails en bloc removal of the upper extremity together with the scapula and the lateral aspect of the clavicle.
Anatomy
The upper extremity and scapula are attached to the upper torso and chest wall by soft tissue elements (rhomboid, levator scapulae, trapezius, pectoralis major and minor, latissimus dorsi, teres major, and serratus anterior muscles) and a single bone (clavicle). They all must be transected to allow the performance of a forequarter amputation.
The axillary vessels and infraclavicular portion of the brachial plexus pass just inferiorly to the coracoid process, which is easily palpable, and lie below the deltopectoral fascia. These structures should be evaluated prior to surgery in order to determine the segment that can be safely transected and ligated, especially because large tumors may come close to the thoracic outlet.
Large tumors of the periscapular area may easily extend into the posterior triangle of the neck, the adjacent paraspinal muscles, and the underlying chest wall. Tumor extension into these anatomic sites must be carefully evaluated prior to surgery because en bloc resection of a chest wall segment or a concomitant neck dissection may be required.
Indications
Primary indications for forequarter amputation include:
- Large soft tissue tumor around the proximal arm/axilla with neurovascular encasement, compromise, and extension across the joint.
- Large bone tumor (primary bone sarcoma or metastatic lesion) of the proximal humerus and scapula with an extensive soft tissue component and invasion into the shoulder joint and surrounding muscles.
- Extensive locoregional tumor recurrence around the shoulder girdle.
- Palliation of intractable pain or tumor fungation, associated with a rapidly enlarging lesion that has not responded to chemotherapy and/or radiation therapy.
**Contraindications:** Forequarter amputation is usually contraindicated when the tumor extends to the chest wall or to the posterior triangle of the neck and paraspinal muscles.
**Special Considerations:** This surgery can be considered in selected cases with no metastases, in which concomitant chest wall resection or neck dissection can achieve negative margins and patients can withstand the physiologic impact of these combined major surgeries.
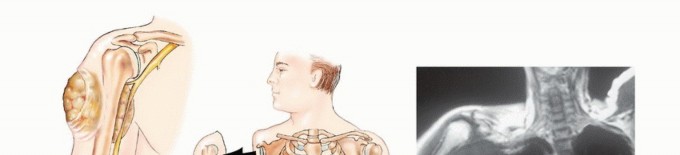
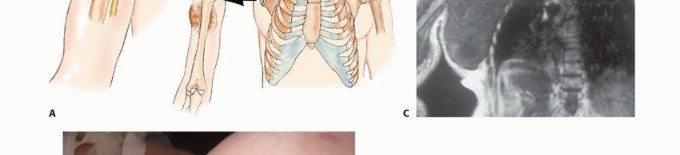
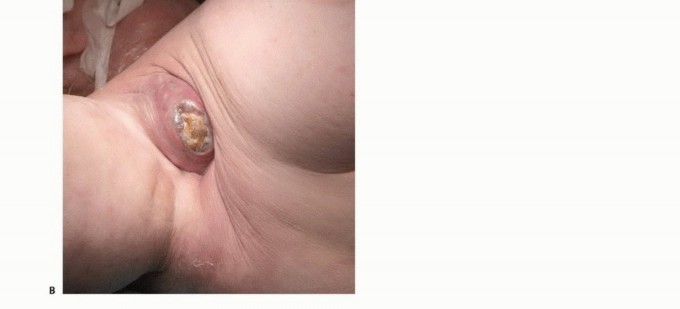
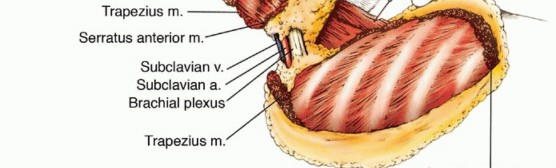
FIG 2: (A) Illustration of high-grade sarcoma encasing the neurovascular bundle. (B, C) Intraoperative photo and MRI of a fungating axillary sarcoma compromising radial and median nerve functions.
Imaging and Other Staging Studies
The combined use of computerized tomography (CT) and magnetic resonance imaging (MRI) allows determination of the extent of bone and soft tissue tumor involvement and thus estimation of the potential size of the soft tissue margins (i.e., at the neck, paraspinal muscles, and chest wall).
Angiography is extremely helpful in locating the anatomic position of the axillary and/or brachial vessels and in evaluating whether these structures are involved by tumor. Physical anomalies (e.g., a duplicate axillary artery) can occasionally be identified as well. Angiography also makes it possible to accurately determine the best level of ligation of the axillary vessels.
No imaging studies can precisely distinguish whether the brachial plexus is infiltrated by tumor or whether the vessels and plexus are simply displaced; they provide only indirect evidence of tumor extension to the nerves. On the other hand, we have found venography of the axillary veins to be a simple and accurate method of determining brachial plexus involvement. A brachial venogram will show complete obstruction of the main axillary veins when a tumor is infiltrating the brachial plexus, whereas it will show venous patency and displacement when a tumor is adjacent to, but not infiltrating, the plexus.
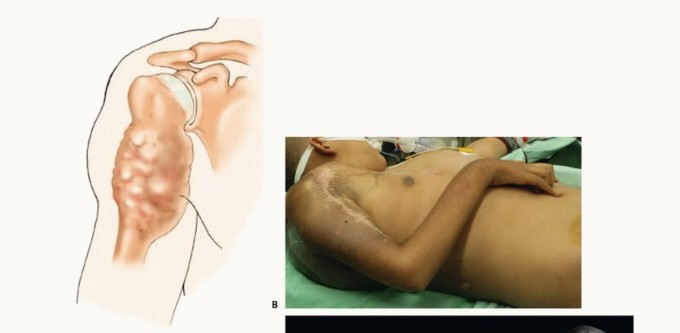
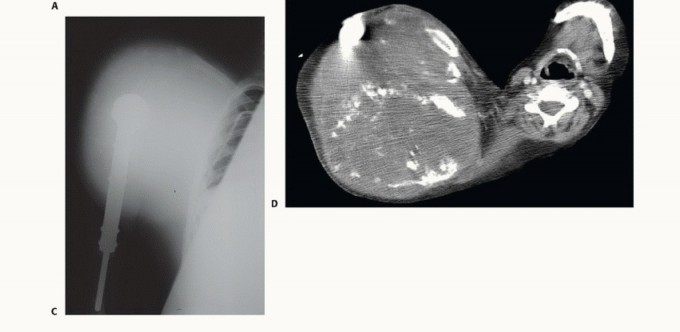
FIG 3: (A) High-grade sarcoma of proximal humerus extending across the joint. (B) Intraoperative view of Ewing sarcoma showing extensive soft tissue destruction despite prior therapy.
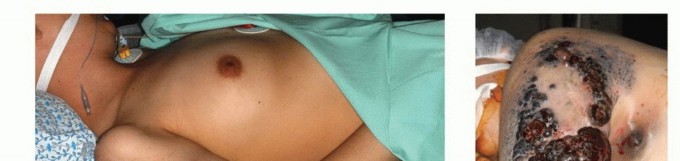
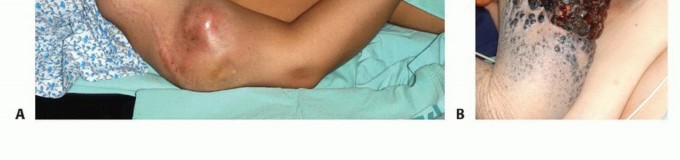
FIG 4: (A) Locally recurrent osteosarcoma at the proximal arm and axilla. (B) Locally recurrent malignant melanoma rapidly growing despite immunotherapy and radiation.
Surgical Management
Positioning
The patient is placed in a full lateral position and is secured to the operating table at the hips with tape. Alternatively, a VAC pack can be used to secure the torso. An axillary roll is placed under the axilla to allow full excursion of the chest, and a sponge-rubber pad is placed under the hip to prevent ischemic damage to the skin in this area. The skin is prepared in the usual manner, and the tumor-bearing extremity is draped free.
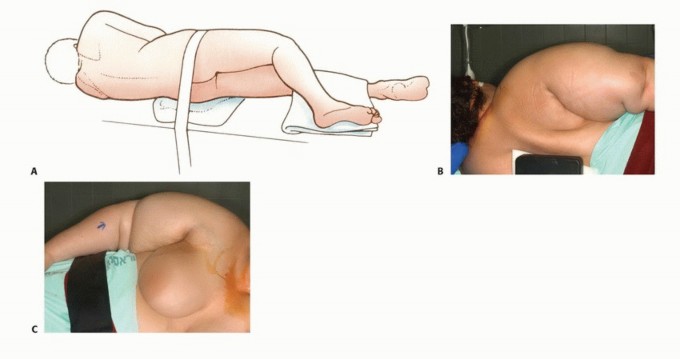
FIG 5: Positioning for forequarter amputation. The patient is secured in a full lateral position with axillary and hip padding to prevent ischemic damage.
Surgical Techniques
1. Incision
The anterior component of the incision starts over the clavicle about 2 cm lateral to the sternoclavicular joint. Caudally, the incision line is in or near the deltopectoral groove; superiorly, it crosses the tip of the acromion. These two lines meet below the axilla to include the skin bearing axillary hair and hematoma that results from the biopsy.
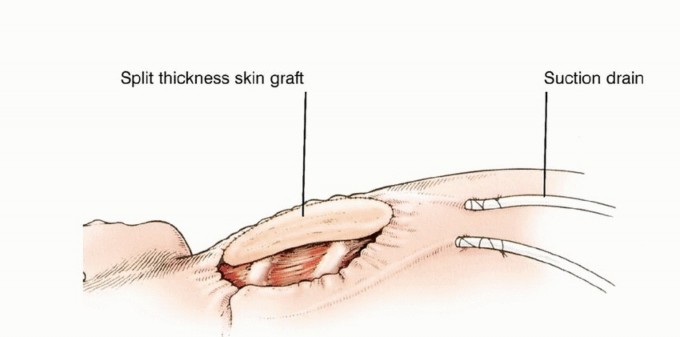
The final shape of the flaps and position of the lines of incision vary according to individual tumor extent. Because of the excellent blood supply to the skin in this region, long anterior or posterior flaps generally survive even though they are closed under considerable tension. Occasionally, large tumors extend to the overlying skin and require en bloc resection with a substantial area of skin. This results in a wound defect that cannot be closed primarily and will require a skin graft or be left for delayed wound closure.
The anterior skin flap, which can be extended to the midsternum, is usually constructed first, with the surgeon standing in front of the patient. The surgeon then switches position to stand behind the patient and constructs the posterior flap to the medial border of the scapula.
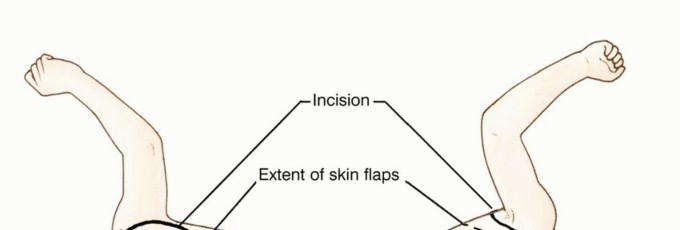

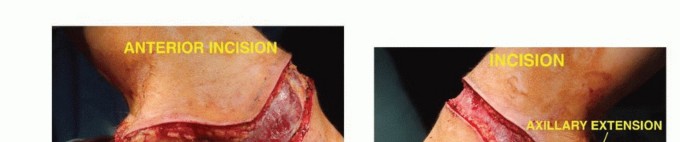
TECH FIG 1: Anterior and posterior components of the incision, starting over the clavicle and crossing the tip of the acromion.
2. Removal of the Affected Limb and Scapula
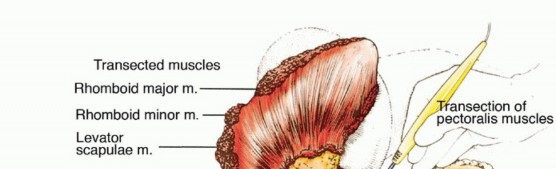
Anterior vascular exploration is performed by detaching the pectoralis major muscle from the clavicle. A clavicular osteotomy is performed at the proximal one-third junction, and the underlying brachial plexus and subclavian vessels are identified. A Satinsky clamp can be placed high along the vessels and surgery can then proceed as planned.
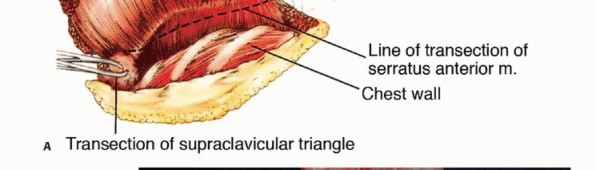
The posterior approach is used to detach the scapula from the rhomboid, trapezius, levator scapulae, and latissimus dorsi muscles. The scapula is lifted from the chest wall by detaching the serratus anterior muscle from its inner plate and the latissimus dorsi at its lowest point.
This exposes the posterior chest wall and allows the surgeon to place his or her hand into the axillary space to check for chest wall or intercostal muscle involvement, whereupon the planned amputation can proceed. If there is chest wall involvement, a combined chest wall/forequarter amputation can be performed. An axillary incision is made to connect the anterior and posterior incisions. The entire forequarter is removed after ligation and transection of the brachial plexus and subclavian vessels.
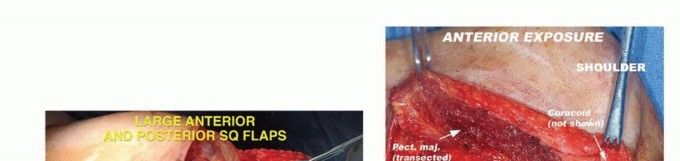



TECH FIG 2: Elevation of the anterior flap, detachment of pectoralis major, clavicular osteotomy, and exposure of subclavian vessels.
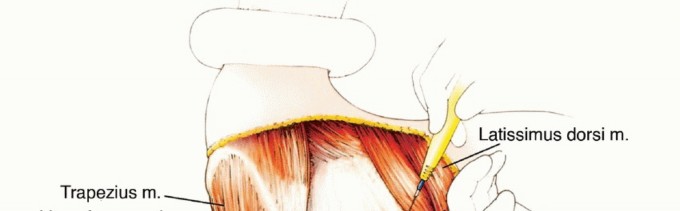
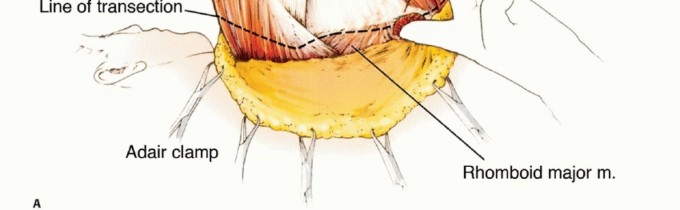
TECH FIG 3: Detachment of the scapular attachments of the rhomboids, trapezius, levator scapulae, and latissimus dorsi muscles.
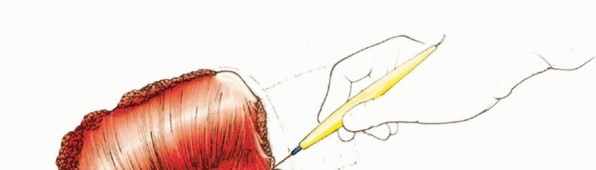

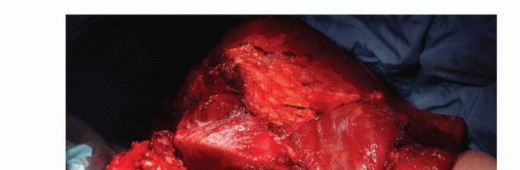
TECH FIG 4: Lifting of the scapula from the chest wall by detaching the serratus anterior and latissimus dorsi.
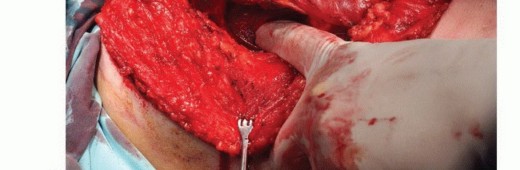
TECH FIG 5: Exposure and palpation of the posterior chest wall for tumor detection to rule out chest wall extension.

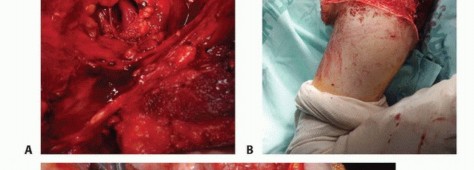
TECH FIG 6: Ligation of subclavian vessels, brachial plexus transection, and the use of epineural catheters for postoperative analgesics.
3. Soft Tissue Reconstruction and Wound Closure
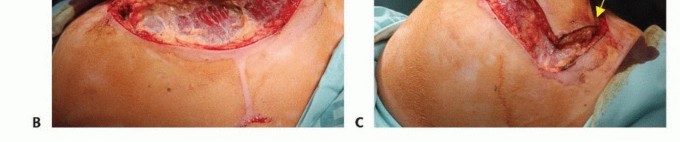
The area is copiously irrigated. The large posterior flap is closed over the remaining chest wall defect. Marked redundancy of the skin may present an unacceptable cosmetic appearance, so every effort should be made to ensure that the skin flaps are carefully approximated.
The midportion of the long posterior skin flap is approximated to the midportion of the anterior flap. Carrying out the closure in this way pleats the longer posterior skin flap and prevents unsightly folds of skin. A two-layered closure, first of superficial fascia and then of skin, is used. Generous suction drainage under the anterior and posterior skin flaps is secured. Suction drains are removed when serous drainage is minimal.
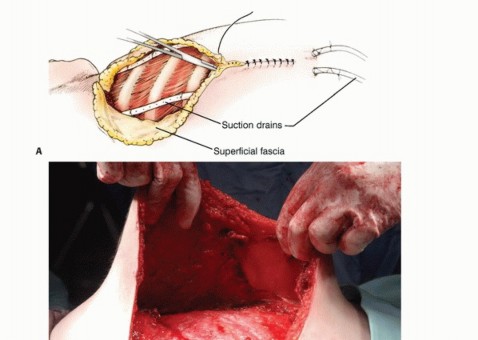


TECH FIG 7: Mobilization of the large posterior fasciocutaneous flap anteriorly over the chest wall.
TECH FIG 8: Wound closure over large suction drains.
Pearls and Pitfalls
- Indications: Mandatory preoperative detailed radiologic assessment of the soft tissue extents of the tumor, its vascular anatomy, and determination of neck and chest wall invasion. If the latter exists and amputation is feasible, make the necessary preparations for concomitant chest wall resection or neck dissection.
- Positioning and Resection: Patient is placed in a full lateral position. Clavicular osteotomy and clamping of the subclavian vessels are done first. Intraoperative palpation of the chest wall to assess tumor extension is crucial.
- Wound Closure: Proper trimming and alignment of the posterior flap are required to avoid redundancy and the formation of unsightly skin folds.
- Analgesia: Marcaine infusion (0.25%) through an epineural catheter placed in the nerve sheath significantly decreases postoperative pain and causalgia.
- Postoperative Care: Assisted postoperative ambulation is necessary to avoid loss of balance due to weight inequality. Early occupational therapy care must be initiated.
Postoperative Care and Rehabilitation
Continuous suction is usually required for 5 to 7 days, and perioperative intravenous antibiotics are continued until the drainage tubes are removed. Phantom pain (causalgia) is a major problem following high-level amputations. We use an epineural catheter placed into the axillary sheath at the time of surgery and infuse 0.25% Marcaine for 3 to 5 days postoperatively. This decreases postoperative pain and may lessen late causalgia syndromes.
Patients initially have difficulties in keeping their balance because of the acute weight inequality of their upper torso and tend to fall toward the contralateral side. This problem typically resolves itself after a few days of assisted walking.
It is crucial to have an occupational therapist involved early in the postoperative period to teach the patient how to perform the activities of daily living with a single upper extremity. This is even more critical when the amputated extremity is the dominant one. A cosmetic prosthesis can be fitted upon wound healing and resolution of wound edema, usually 4 to 6 weeks after surgery.
Outcomes
Forequarter amputation is a mutilating procedure that has a profound aesthetic, psychological, and functional impact on the patients. It is done for large and aggressive tumors, which bear a high risk of metastatic dissemination. Most patients who undergo forequarter amputation gain local control over their tumor but still face the likelihood of distant metastases.
Pain relief and improved quality of life are pronounced in patients who had undergone palliative amputation to control intractable pain associated with a rapidly enlarging tumor that had not responded to chemotherapy and radiation therapy. Most patients who undergo forequarter amputation regain reasonable function and are able to perform most daily activities. For some yet undefined reason, phantom limb pain is less common and disturbing than that associated with high amputation of the lower extremities.
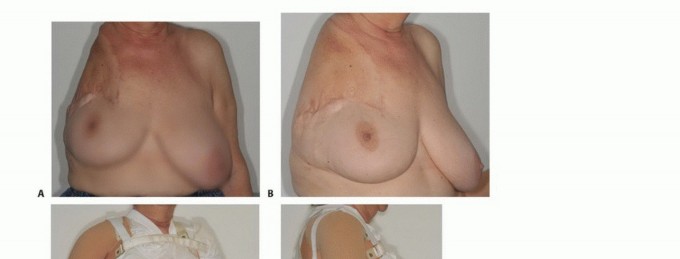


FIG 6: Functional and cosmetic outcomes. Note the typical deformity of the shoulder girdle, the use of a custom-made cosmetic prosthesis, and a healed clinical photograph 5 years post-surgery.
Complications
- Flap Ischemia: Usually superficial and marginal because of the good blood supply of the shoulder girdle. It typically resolves spontaneously. Occasionally, there is full-thickness necrosis of the posterior flap. A clear demarcation line appears after 4 to 7 days, after which débridement of the necrotic segment and primary closure are carried out.
- Phantom Limb Pain
- Local Tumor Recurrence

FIG 7: Superficial flap ischemia occurring 3 days after surgery, which resolved spontaneously after 5 days.
Scientific References
- Bhagia SM, Elek EM, Grimer RJ, et al. Forequarter amputation for high-grade malignant tumours of the shoulder girdle. J Bone Joint Surg Br 1997;79:924-926.
- Bickels J, Wittig JC, Kollender Y, et al. Limb-sparing resections of the shoulder girdle. J Am Coll Surg 2002;194:422-435.
- Ferrario T, Palmer P, Karakousis CP. Technique of forequarter (interscapulothoracic) amputation. Clin Orthop Relat Res 2004;423:191-195.
- Fianchini A, Bertani A, Greco F, et al. Transthoracic forequarter amputation and left pneumonectomy. Ann Thorac Surg 1996;62: 1841-1843.
- Kuhn JA, Wagman LD, Lorant JA, et al. Radical forequarter amputation with hemithoracectomy and free extended forearm flap: technical and physiologic considerations. Ann Surg Oncol 1994;1: 353-359.
- Levine EA, Warso MA, McCoy DM, et al. Forequarter amputation for soft tissue tumors. Am Surg 1994;60:367-370.
- Merimsky O, Kollender Y, Inbar M, et al. Is forequarter amputation justified for palliation of intractable cancer symptoms? Oncology 2001;60:55-59.
- Roth JA, Sugarbaker PH, Baker AR. Radical forequarter amputation with chest wall resection. Ann Thorac Surg 1984;37:423-427.
- Wittig JC, Bickels J, Kollender Y, et al. Palliative forequarter amputation for metastatic carcinoma to the shoulder girdle region: indications, preoperative evaluation, surgical technique, and results. J Surg Oncol 2001;77:105-113. [View Source / PubMed]
