DEFINITION
Multiple hereditary exostoses (MHE), first described by Boyer3 in 1814, is a familial disorder with an autosomal dominant mode of inheritance exhibiting very high penetrance and variable expressivity.12 Also known asmultiple osteochondromatosis,multiple osteochondromata,multiple cartilage exostoses,diaphyseal aclasis, ormetaphyseal aclasis5,23
ANATOMY
Knowledge of the normal anatomy and biomechanics of the forearm in the immature individual is instrumental in understanding the pathogenesis of the deformity and ultimately in planning appropriate treatment.During forearm pronation-supination, the relationship between the radius and ulna changes. This rotational movement requires near-anatomic alignment of both as well as integrity of the proximal and distal radioulnar joints and the interosseous membrane. Minimal axial or rotational bone deformity, asymmetric bone shortening, or ligament instability can hinder this function.The ulna acts like a swivel hinge around which the radius rotates. The axis of forearm rotation is oblique.
PATHOGENESIS
The most common genetic mutations are in theEXT-1andEXT-2genes.6Approximately 10% of individuals with manifestations of multiple exostoses have no family history of MHE.22 The prevalence of MHE in the general population is estimated to be at least one in 50,000, with a median age of first diagnosis of 2 to 3 years of age (exostoses rarely develop before age 2 years).22 An average of five orsix exostoses, involving both upper and lower extremities, is found at the time of the first consultation.9The presence of exostoses is almost always evident by the age of 12 years.Osteochondromas develop at numerous sites in the immature skeleton, they may affect any bone except the skull. They most commonly affect the ends of long bones and flat bones including the scapula and pelvis.Osteochondromas consist of a base or stalk covered by a cartilaginous cap. They arise from the peripheral aspect of the growth plate of bones that undergo endochondral ossification.14They are the product of abnormal proliferation of chondroblasts and subsequent defective remodeling of the metaphysis. This leads to the two main characteristics of this condition: skeletal metaphyseal exostoses and retardation of longitudinal bone growth.They migrate away from the physis with longitudinal growth.14In MHE, the exostoses vary greatly in number, location, size, and configuration. They tend to have a more irregular and bizarre shape than solitary osteochondromas.Should always be continuous with the medullary cavity of the bone from which they ariseOnce skeletal maturity is reached, the lesions will become quiescent.22 Lesions that enlarge after skeletal maturity should be investigated to exclude malignant change.
NATURAL HISTORY
Deformity of the forearm is seen in 30% to 60% of the individuals with MHE.22 The forearm deformities can be progressive and result in a variable amount of weakness, pain,4 functional limitation, and aesthetic deformity.The deformities are almost always accompanied by discrepancy in length between the two bones. Asynchronous longitudinal growth between paired bones leads to a greater risk of anatomic distortion. Mostof the longitudinal growth of the ulna occurs at the distal physis,15 which is also the more commonly affected physis (30% to 85% of the cases).22,23The affected ulna typically remains relatively shortened and curved, and this often leads to significant bowing of the radius. When the ulna is shorter, the ulnar-sided soft tissue acts as a tether, causing bowing of the radius. In addition, the local presence of the exostosis itself causes radial bowing by disturbinghemiepiphyseal growth.15A serious risk associated with MHE is the potential for malignant transformation of an exostosis into chondrosarcoma. This can occur at any age, but it is exceedingly rare during childhood.22Patients affected by MHE have a normal life expectancy unless malignant degeneration and metastasis develop.9 The risk of malignant degeneration in adults with MHE has been reported to range from 0.57% to 5%.12,22,31MHE can have a serious influence on the quality of life of affected individuals, affecting sporting participation, occupation, and daily activities.8
HISTORY AND PHYSICAL FINDINGS
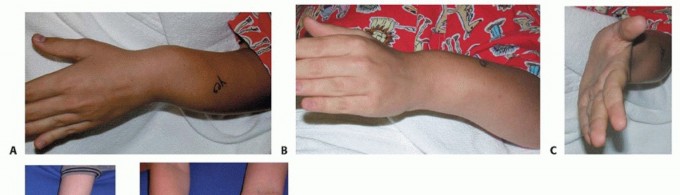
FIG 1 • A. Significant ulnar deviation of the wrist, which can also be present in these patients. B,C. The patient has limited pronation and supination. D. Obvious radial head dislocation, reported. E. Patient with severe involvement of the left forearm. Physical examination of the upper extremity should assess for location of disease burden and common associated findings.It is a common finding that the deformity is quite asymmetric. One forearm may be heavily affected, whereas the other relatively spared.Shortening of the forearm, specifically relative shortening of the ulna, increased radial bow and possible radial head dislocation.A mild flexion deformity of the elbow is often present.At the wrist level, an increased ulnar tilt of the radial epiphysis, ulnar deviation of the hand, and progressive ulnar translocation of the carpus are often present. These deformities can lead to a loss of radial deviation of the hand and loss of pronation-supination of the forearm (FIG 1).The loss of forearm pronation-supination may develop early and become progressively more severe as thechild ages.26 Pronation-supination may be limited due to altered mechanical alignment, osteochondroma blocking motion, or radial head dislocation. The greater the number of osteochondromas and shorter the ulna, the greater the loss of motion.10,32Radial head dislocation is reported to occur in 22% of the affected forearms.23 It may present as pain, a mass on the lateral side of the elbow, altered carrying angle, decreased elbow range of motion or decreased pronation-supination, or catching.It is possible to have neurologic impingement from either direct compression by an osteochondroma or through deformity including radial head dislocation.
IMAGING AND OTHER DIAGNOSTIC STUDIES


FIG 2 • Radiographs showing large osteochondroma of distal ulna affecting the epiphysis and causing significant tethering of the radius. Characteristically, the distal ulna is narrow with a pointed end.
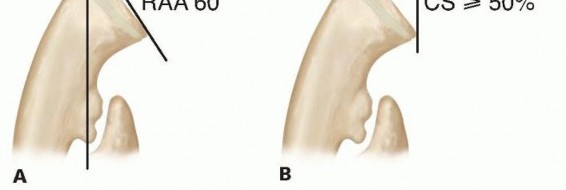

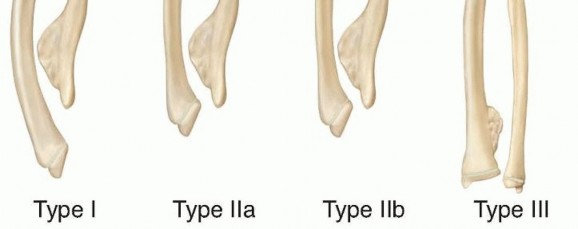
FIG 4 • Masada classification of the involvement of the forearm in MHE. (Adapted from Masada K, Tsuyuguchi Y, Kawai H, et al. Operations for forearm deformity caused by multiple osteochondromas. J Bone Joint Surg Br 1989;71:24-29.) In older children and teenagers, irregular areas of calcification of the cartilaginous cap may be present. Extensive calcification with changes in the shape, thickness of the cartilaginous cap, or a lesion enlarging more rapidly than the growth of the child should raise suspicion of possible chondrosarcoma transformation.
DIFFERENTIAL DIAGNOSIS
Langer-Giedion syndrome Madelung deformity Chondrosarcoma
NONOPERATIVE MANAGEMENT
Patients with MHE can often be managed successfully using a conservative approach.Exostoses alone can often be surprisingly well tolerated and result in minimal loss of function.26 It has been reported that forearm function in untreated adults with MHE is subjectively greater than the one objectivelymeasured.17The conspicuous number of lesions and the fact that they are mostly asymptomatic warrant a cautious surgical approach.A dislocated radial head that is not symptomatic should be left alone.Attempts at relocating a dislocated radial head have been unsuccessful.2,19
SURGICAL MANAGEMENT
Surgical treatment of forearm deformities in MHE remains controversial. A number of operative techniques have been proposed.5,10,15,20,24The main surgical indications are toImprove forearm function (pronation-supination)2Relieve pain from external trauma or irritation of the surrounding soft tissue4 Improve appearance10Exclude malignancy when there is a rapid increase in size of a lesion18When evaluating the surgical indications in an individual patient, it is important to distinguish between the functional deficit and the cosmetic appearance.The postoperative appearance of the forearm has been shown to be unrelated to the functional outcome.17Despite many maintaining good function even without treatment,2,17 a percentage of patients find theappearance of the shortening, angulation, and deformities unacceptable.17 If surgery is being undertaken for aesthetic rather than functional purposes, the hopes, concerns, and expectations of patient and parents must be thoroughly discussed and accurately outlined.A mass or deformation may be removed; however, a scar shall be added.Restoration of range of motion and improvement of radiographic parameters are unpredictable but may occur.2,11Some5,15,18 advocate an aggressive approach based on the rationale that forearm deformities may lead to functional impairment especially if radial head dislocation occurs.2,26P.1346Surgical treatment employed includes excision of the exostoses and ulnar lengthening and associated radial osteotomy when indicated.Radiographic indications cited include relative ulnar shortening (with or without bowing) of more than 1.5 cm, RAA of greater than 30 degrees, carpal slip of more than 60%, and bowing of the radius or the ulna (orboth).5Predication of radial head dislocation has remained one of the most difficult aspects of MHE forearm care.The most common association with radial head dislocation is isolated distal ulnar osteochondromas.7However, our approach reflects that the presence of forearm deformities alone is relatively unrelated to functional impairment,2,17,26 and therefore we do not recommend surgical correction of the deformities only to prevent a possible, but not predictable, future functional impairment.Symptomatic dislocation of the radial head is an indication for surgical intervention when it interferes with joint motion or causes significant pain.
PROCEDURES
Exostosis excision alone is indicated when a lesion becomes symptomatic or when it directly causes limitation of forearm pronation-supination.This procedure alone does not necessarily correct the forearm deformity. Excision of a distal ulnar osteochondroma may lead to remodeling of the radius.11Ulnar tether release is indicated when there is significant wrist deformity present secondary to ulnarshortening.When the distal epiphyseal plate of the ulna has lost its growth potential and resultant significant radial bowing exists, extensive ulnar tether release is our preferred technique to improve wrist position and potentially decrease the risk of radial head subluxation/dislocation. Lengthening may temporarily level the joint; however, the physis will not provide growth and recurrent deformity is common.May be combined with osteochondroma excision or radial osteotomyIf the patient has significant growth potential remaining, ulnar tether release alone can lead to radial correction.Ulnar lengthening with or without radial osteotomy remains a common procedure.Acute10,30 and gradual1,13,16,20,28 lengthenings have been used.Ulnar lengthening levels the joint and relieves tension on the ulnar-sided soft tissues.Anatomic structure, alignment, and potential for remodeling of the DRUJ needs to be considered prior to lengthening the ulna.Lengthening will not restore growth to the distal ulna, the remaining growth potential and possible recurrence of deformity needs to be considered.There are incumbent risks associated with lengthening procedures. The risks and benefits must be considered. The time to union or consolidation of bone regenerate is commonly 2 to 3 months.Radial osteotomy is performed in the skeletally mature or nearly skeletally mature patient.Significant remodeling of the radius is unlikely in the older patient. Radial osteotomy acutely corrects the radial deformity.Combination with osteochondroma excision and ulnar-sided procedures is common.Consider staging procedures if the level of surgery is similar on the radius and ulna to minimize the risk of synostosis or loss of correction.Distal radial hemiepiphysiodesis with stapling has been used in the past.15,25 It has not gained widespread use.Treatment for symptomatic radial head dislocation is usually limited to salvage procedures.Surgical excision may be performed once the patient is skeletally mature. Excision before this time may lead to instability, growth disturbance, and possible worsening of the wrist or elbow deformity.Formation of a single-bone forearm has been successfully used in the skeletally immature and skeletally mature patient.19,21,29In rare instances, exostosis excision with osteotomy or ulnar lengthening may be effective in relocating the radial head.16
TECHNIQUE
Exostosis Excision and Ulnar Tethering Release


TECH FIG 1 • A. Exposure of large osteochondroma of the distal ulna. B. Dissection and exposure of the osteochondroma. Significant tethering is present distally. C. After excision of osteochondroma and release of ulnar tethering.
DISTAL RADIAL OSTEOTOMY


TECH FIG 2 • A. Prior to distal radial dome osteotomy. B. Early postoperative radiograph. C. Postoperative outcome at skeletal maturity.A dome osteotomy is selected when there is no significant ulnar shortening.Wire fixation is usually adequate for the osteotomy (either two stout K-wires or multiple smaller caliber wires).Wires may be preplaced in the radial styloid before completion and displacement of the osteotomy. They are inserted percutaneously into the radial styloid.Once the osteotomy is displaced, the wires are driven across until they obtain bicortical fixation.Adequacy of correction and final alignment is checked using fluoroscopy (TECH FIG 2B,C). Pronator quadratus is repaired using interrupted absorbable sutures.3. Radial Head ExcisionP.1348An incision is made over the prominent radial head with the forearm in pronation to protect the posterior interosseous nerve.Dissection is then carried down in the interval between the anconeus muscle and ECU. TECH FIG 3 • A. Patient with painful radial head dislocation. B. Exposure of the radial head. Forearm is in a pronated position to protect the posterior interosseous nerve. C. Radial head exposed before excision. D. Excised radial head. Significant degenerative changes are present.




FIG 5 • A. Radiograph of a 5-year-old child prior to ulnar tether release with increased radial slope and severely affected distal ulnar physis. B. Seven years after ulnar tether release.
POSTOPERATIVE CARE
Exercises to maintain the range of motion of the fingers are encouraged immediately after surgery regardless of the technique used.In cases of ulnar tethering release, casting is performed for 4 weeks, followed by range-of-motion exercises and splinting.If an osteotomy was performed, casting is continued until radiographic evidence of healing is seen.
OUTCOMES
Many MHE patients do not need surgery. In patients who require surgery, ulnar tether release, with or without exostoses excision, with or without radial osteotomy, provides reliable results with the few complications (FIG 5). In selected patients, this can greatly improve function in addition to the improved cosmesis of the extremity.Ulnar lengthening is reserved for select patients.For symptomatic radial head dislocations, radial head excision usually leads to a consistent, reproducible result; however, formation of single-bone forearm can certainly be beneficial, especially in the skeletally immature patient.
REFERENCES
- Abe M, Shirai H, Okamoto M, et al. Lengthening of the forearm by callus distraction. J Hand Surg Br 1996;21:151-163.
- Akita S, Murase T, Yonenobu K, et al. Long-term results of surgery for forearm deformities in patients with multiple cartilaginous exostoses. J Bone Joint Surg Am 2007;89:1993-1999.
- Boyer A. Traite des Maladies Chirurgicales et des Operations qui Leur Conviennent. Paris: Chez l'Auteur, 1814.
- Darilek S, Wicklund C, Novy D, et al. Hereditary multiple exostoses and pain. J Pediatr Orthop 2005;25:369-376.
- Fogel GR, McElfresh EC, Peterson HA, et al. Management of deformities of the forearm in multiple hereditary osteochondromas. J Bone Joint Surg Am 1984;66:670-680.
- Francannet C, Cohen-Tanugi A, LeMerrer M, et al. Genotypephenotype correlation in hereditary multiple exostoses. J Med Genet 2001;38:430-434.
- Gottschalk HP, Kanauchi Y, Bednar MS, et al. Effect of osteochondroma location on forearm deformity in patients with multiple hereditary osteochondromatosis. J Hand Surg Am 2012;37:2286-2293.
- Goud AL, de Lange J, Scholtes VA, et al. Pain, physical and social functioning, and quality of life in individuals with multiple hereditary exostoses in The Netherlands: a national cohort study. J Bone Joint Surg 2012;94:1013-1020.
- Herring JA. Tachdjian's Pediatric Orthopaedics. ed 4. Philadelphia: WB Saunders, 2007.
- Ip D, Li YH, Chow W, et al. Reconstruction of the forearm deformities in multiple cartilaginous exostoses. J Pediatr Orthop B 2003;12:17-21.
- Ishikawa J, Kato H, Fujioka F, et al. Tumor location affects the results of simple excision for multipleosteochondromas in the forearm. J Bone Joint Surg Am 2007;89:1238-1247.
- Legeai-Mallet L, Munnich A, Maroteaux P, et al. Incomplete penetrance and expressivity skewing in hereditary multiple exostoses. Clin Genet 1997;52:12-16.
- Mader K, Gausepohl T, Pennig D. Shortening and deformity of radius and ulna in children: correction of axis and length by callus distraction. J Pediatr Orthop B 2003;12:183-191.
- Mansoor A, Beals RK. Multiple exostosis: a short study of abnormalities near the growth plate. J Pediatr Orthop B 2007;16:363-365.
- Masada K, Tsuyuguchi Y, Kawai H, et al. Operations for forearm deformity caused by multiple osteochondromas. J Bone Joint Surg Br 1989;71:24-29.
- Matsubara H, Tsuchiya H, Sakurakichi K, et al. Correction and lengthening for deformities of the forearm in multiple cartilaginous exostoses. J Orthop Sci 2006;11:459-466.
- Noonan KJ, Levenda A, Snead J, et al. Evaluation of the forearm in untreated adult subjects with multiple hereditary osteochondromatosis. J Bone Joint Surg Am 2002;84:397-403.
- Peterson HA. Deformities and problems of the forearm in children with multiple hereditary osteochondromata. J Pediatr Orthop 1994;14:92-100.
- Peterson HA. The ulnius: a one-bone forearm in children. J Pediatr Orthop B 2008;17:95-101.
- Pritchett JW. Lengthening the ulna in patients with hereditary multiple exostoses. J Bone Joint Surg Br 1986;68:561-565.
- Rodgers WB, Hall JE. One-bone forearm as a salvage procedure for recalcitrant forearm deformity in hereditary multiple exostoses. J Pediatr Orthop 1993;13:587-591.
- Schmale GA, Conrad EU III, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
- Shapiro F, Simon G, Glimcher MJ. Hereditary multiple exostoses. Anthropometric, roentgenographic, and clinical aspect. J Bone Joint Surg Am 1979;61:815-824.
- Shin EK, Jones NF, Lawrence JF. Treatment of multiple hereditary osteochondromas of the forearm in children: a study of surgical procedures. J Bone Joint Surg Br 2006;88:255-260.
- Siffert RS, Levy RN. Correction of the wrist deformity in diaphyseal aclasis by stapling. Report of a case. J Bone Joint Surg Am 1965;47:1378-1380.
- Stanton RP, Hansen MO. Function of the upper extremities in hereditary multiple exostoses. J Bone Joint Surg Am 1996;78:568-573.
- Vanhoenacker FM, Van Hul W, Wuyts W, et al. Hereditary multiple exostoses: from genetics to clinical syndrome and complications. Eur J Radiol 2001;40:208-217.
- Vogt B, Tretow HL, Daniilidis K, et al. Reconstruction of forearm deformity by distraction osteogenesis in children with relative shortening of the ulna due to multiple cartilaginous exostosis. J Pediatr Orthop 2011;31:393-401.
- Waters PM. Forearm rebalancing in osteochondromatosis by radioulnar fusion. Tech Hand Up Extrem Surg 2007;11:236-240.
- Waters PM, Van Heest AE, Emans J. Acute forearm lengthenings. J Pediatr Orthop 1997;17:444-449.
- Watts AC, Ballantyne JA, Fraser M, et al. The association between the ulnar length and the forearm movement in patients with multiple osteochondromas. J Hand Surg Am 2007;32(5):667-673.
- Wicklund CL, Pauli RM, Johnston D, et al. Natural history study of hereditary multiple exostoses. Am J Med Genet 1995;55:43-46.
