Introduction & Epidemiology
The forearm represents a critical anatomical and biomechanical segment of the upper extremity, mediating the intricate interplay between elbow and wrist function. Its complex arrangement of osseous structures, muscular compartments, neurovascular networks, and connective tissues facilitates a wide range of motion, force generation, and fine motor control essential for daily activities. Injuries and pathological conditions affecting the forearm can severely compromise global upper limb function, necessitating a profound understanding of its detailed anatomy for accurate diagnosis and effective surgical intervention.
Forearm fractures, nerve compression syndromes (e.g., posterior interosseous nerve syndrome), compartment syndromes, and soft tissue pathologies collectively account for a significant burden in orthopedic practice. Radial and ulnar shaft fractures are common, with an estimated incidence of 10-15 per 100,000 person-years, varying with age and activity levels. Distal radius fractures are among the most prevalent fractures in adults, while pediatric forearm fractures are also highly frequent. Understanding the precise anatomical relationships, particularly the course and vulnerability of key neurovascular structures like the Posterior Interosseous Nerve (PIN), is paramount in mitigating iatrogenic injury and optimizing patient outcomes during surgical approaches. This review aims to delineate the comprehensive surgical anatomy of the forearm, with a particular focus on the PIN, its clinical relevance, and its implications for surgical management.
Surgical Anatomy & Biomechanics
The forearm extends from the elbow joint proximally to the wrist joint distally, comprising two long bones—the radius and the ulna—connected by a robust interosseous membrane. This structural arrangement, coupled with its muscular and neurovascular components, dictates the complex biomechanics of pronation and supination, as well as wrist and hand movements.
Osteology
The radius and ulna articulate proximally at the elbow (radiocapitellar and proximal radioulnar joints) and distally at the wrist (distal radioulnar and radiocarpal joints).
Ulna
-
Proximally
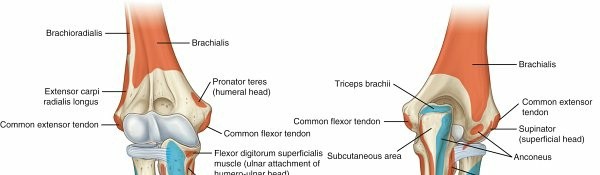
: The ulna features two curved processes, the olecranon and the coronoid processes, which form the trochlear notch. This notch articulates with the trochlea of the humerus, forming the primary hinge component of the elbow joint.
- The olecranon process serves as the insertion site for the triceps brachii, the primary elbow extensor.
- The coronoid process provides an attachment for the brachialis muscle and contributes to the stability of the elbow joint.
- Adjacent to the coronoid process, the radial notch on the lateral aspect articulates with the radial head.
- Shaft : The ulnar shaft is triangular proximally and cylindrical distally. It tapers distally.
- Distally : The ulna ends in a lateral head (which articulates with the ulnar notch of the radius to form the distal radioulnar joint) and a medial styloid process . The ulnar styloid serves as an attachment point for the ulnar collateral ligament of the wrist.
Radius
- Proximally : The radius consists of a head with a central fovea that articulates with the capitellum of the humerus. Inferior to the head is the neck , followed by the proximal medial radial tuberosity , which serves as the insertion site for the biceps brachii tendon.
-
Shaft
: The radial shaft has a characteristic gradual bend (convex laterally), known as the
radial bow
. This curvature is crucial for maintaining the physiological arc of pronation and supination.
- Restoration of the radial bow (and length) is critical in the fixation of radial shaft fractures to maintain the arc of pronation and supination. Loss of this bow can lead to significant functional impairment, including restricted forearm rotation and impingement.
-
Distally
: The distal radius is composed of the
carpal articular surface
(scaphoid and lunate fossae), an
ulnar notch
(for articulation with the ulnar head), a
dorsal tubercle (Lister's tubercle)
, and a
lateral styloid process
.
- Lister's tubercle is an important anatomical landmark, typically located at the level of the scapholunate joint, often used for surgical orientation and as a pulley for the extensor pollicis longus (EPL) tendon. The radial styloid is more distal than the ulnar styloid, a relationship crucial for normal wrist kinematics.

Figure 1: Lateral view of the radius and ulna, highlighting proximal and distal landmarks.
Arthrology
The forearm's articulation includes:
*
Proximally
: The elbow joint, which comprises the humeroulnar (trochlea-trochlear notch), humeroradial (capitellum-radial head fovea), and proximal radioulnar articulations. The latter is essential for forearm rotation.
*
Distally
: The wrist joint, which encompasses the distal radioulnar joint (DRUJ) and the radiocarpal joint. The DRUJ is a pivot joint, allowing pronation and supination, and is stabilized by the triangular fibrocartilage complex (TFCC). The radiocarpal joint is a condyloid joint, allowing flexion, extension, radial, and ulnar deviation.
Interosseous Membrane
The radius and ulna are connected by a robust, oblique
interosseous membrane/ligament
. This fibrous sheet extends from the interosseous crest of the radius to that of the ulna. It serves several critical functions:
*
Stabilization
: Binds the radius and ulna together, preventing longitudinal displacement.
*
Load Transmission
: Transfers axial loads from the radius (e.g., from hand/wrist) to the ulna and subsequently to the humerus, especially during gripping and weight-bearing. Approximately 80% of axial load across the wrist is transmitted through the radius to the ulna via the interosseous membrane.
*
Muscle Attachment
: Provides broad surfaces for the attachment of deep forearm muscles.
*
Pathology
: Its disruption, particularly proximally, can be a hallmark of complex injuries such as the
Essex-Lopresti injury
, involving a radial head fracture, rupture of the interosseous membrane, and disruption of the DRUJ.
Myology and Compartments
The forearm is divided into anterior (flexor) and posterior (extensor) compartments, separated by the radius, ulna, interosseous membrane, and intermuscular septa.
Anterior (Flexor) Compartment
Innervated primarily by the median nerve (except for the flexor carpi ulnaris and medial half of flexor digitorum profundus, which are ulnar nerve-innervated).
*
Superficial Layer
: Originates from the common flexor origin on the medial epicondyle.
*
Pronator Teres
: Inserts on the lateral radius; pronates and weakly flexes the elbow.
*
Flexor Carpi Radialis (FCR)
: Inserts at the base of the 2nd and 3rd metacarpals; flexes and radially deviates the wrist.
*
Palmaris Longus
: Inserts into the palmar aponeurosis; weakly flexes the wrist (absent in ~15% of individuals).
*
Flexor Carpi Ulnaris (FCU)
: Inserts into the pisiform, hook of hamate, and base of 5th metacarpal; flexes and ulnar deviates the wrist.
*
Flexor Digitorum Superficialis (FDS)
: Lies deep to the above, origins from humerus, ulna, and radius; flexes proximal interphalangeal (PIP) joints and contributes to wrist and MCP flexion.
*
Deep Layer
:
*
Flexor Digitorum Profundus (FDP)
: Origins from ulna and interosseous membrane; flexes distal interphalangeal (DIP) joints and contributes to PIP, MCP, and wrist flexion.
*
Flexor Pollicis Longus (FPL)
: Origins from radius and interosseous membrane; flexes the interphalangeal (IP) joint of the thumb.
*
Pronator Quadratus
: Lies transversely across the distal radius and ulna; primary pronator of the forearm.

Figure 2: Anterior compartment muscles of the forearm.
Posterior (Extensor) Compartment
Innervated entirely by the radial nerve and its deep branch, the Posterior Interosseous Nerve (PIN).
*
Superficial Layer (Mobile Wad)
:
*
Brachioradialis
: Originates from the lateral supracondylar ridge; flexes the elbow, particularly in a neutral forearm position. Not a true extensor.
*
Extensor Carpi Radialis Longus (ECRL)
: Originates from the lateral supracondylar ridge; extends and radially deviates the wrist.
*
Extensor Carpi Radialis Brevis (ECRB)
: Originates from the lateral epicondyle (common extensor origin); extends and radially deviates the wrist. Often considered the workhorse radial wrist extensor.
*
Deep Layer (True Extensors)
: Originates from the ulna, interosseous membrane, and deep fascia.
*
Supinator
: Wraps around the radial neck; supinates the forearm. The Posterior Interosseous Nerve (PIN) passes through its two heads.
*
Abductor Pollicis Longus (APL)
: Origins from radius, ulna, and interosseous membrane; abducts and extends the thumb.
*
Extensor Pollicis Brevis (EPB)
: Origins from radius and interosseous membrane; extends the MCP and IP joints of the thumb.
*
Extensor Pollicis Longus (EPL)
: Origins from ulna and interosseous membrane; extends the IP, MCP, and CMC joints of the thumb, wrapping around Lister's tubercle.
*
Extensor Indicis (EI)
: Origins from ulna and interosseous membrane; extends the index finger independently.
*
Extensor Digitorum (ED)
: Origins from common extensor origin; extends the medial four digits.
*
Extensor Digiti Minimi (EDM)
: Origins from common extensor origin; extends the little finger independently.

Figure 3: Posterior compartment muscles of the forearm, showing superficial layer and deep layer origins.

Figure 4: Detailed view of the deep extensor compartment muscles and their relationships.
Neurovascular Anatomy
Radial Nerve and Posterior Interosseous Nerve (PIN)
The
radial nerve
enters the forearm anterior to the lateral epicondyle, deep to the brachioradialis. Here, it divides into its two main terminal branches:
*
Superficial Radial Nerve (SRN)
: A purely sensory nerve, it runs deep to the brachioradialis, emerging distally to supply sensation to the dorsum of the hand and radial three and a half digits. It is vulnerable during distal radius fixation and surgical approaches to the radial shaft.
*
Deep Branch of the Radial Nerve (Posterior Interosseous Nerve - PIN)
: This is the primary motor nerve to the extensor compartment of the forearm.
*
Course
: The PIN pierces the supinator muscle, passing between its superficial and deep heads, an area known as the
Arcade of Frohse
. This arcade, a fibrous arch at the proximal border of the superficial head of the supinator, is a common site of PIN compression.
*
Branches
: After exiting the supinator, the PIN branches extensively to innervate all the muscles of the deep extensor compartment: Supinator (often receives branches before complete exit), ECRB (variable, often before supinator entry), APL, EPB, EPL, EI, ED, and EDM.
*
Functional Impact
: PIN palsy results in a characteristic "drop wrist" deformity, with inability to extend the fingers at the MCP joints and inability to extend or abduct the thumb. Wrist extension may be preserved or weakened due to innervation of ECRL and ECRB (the latter often receiving branches from the radial nerve
before
the PIN enters the supinator, or from the PIN proper
after
exiting). Crucially, PIN has no sensory component, distinguishing it from radial nerve palsy.
*
Surgical Relevance
: The PIN is highly vulnerable during surgical approaches to the proximal radius and ulnar shaft, particularly the posterior approach (Thompson) and the anterolateral approach (Kaplan). Its exposure requires careful dissection of the supinator, and it must be protected during plate application and screw insertion.

Figure 5: Course of the radial nerve and its deep branch (PIN) through the supinator muscle.
Median Nerve
- Enters the forearm anterior to the elbow, between the heads of the pronator teres.
- Courses deep to the FDS, between FDS and FDP.
- Provides motor innervation to most of the flexor-pronator mass (Pronator Teres, FCR, Palmaris Longus, FDS, FPL, Pronator Quadratus, and lateral half of FDP).
- The Anterior Interosseous Nerve (AIN) , a purely motor branch of the median nerve, arises just distal to the pronator teres and innervates FPL, Pronator Quadratus, and the lateral half of FDP. AIN syndrome presents with inability to flex the DIP of the thumb and index finger (pinch sign).
- Sensory innervation to the radial side of the palm and digits 1-3.5.

Figure 6: Median nerve course and its branches in the forearm.
Ulnar Nerve
- Enters the forearm posterior to the medial epicondyle (cubital tunnel).
- Courses deep to the FCU.
- Provides motor innervation to FCU and the medial half of FDP.
- Sensory innervation to the ulnar side of the hand and digits 4.5-5.

Figure 7: Ulnar nerve course and its relationship to the FCU.
Vascular Supply
- The brachial artery bifurcates in the cubital fossa into the radial artery and ulnar artery .
- Radial Artery : Courses distally deep to the brachioradialis, supplying radial forearm structures, and forming the primary arterial supply to the hand.
-
Ulnar Artery
: Gives off the
common interosseous artery
, which then divides into the
anterior interosseous artery (AIA)
and
posterior interosseous artery (PIA)
.
- AIA : Travels on the anterior surface of the interosseous membrane with the AIN.
- PIA : Travels on the posterior surface of the interosseous membrane with the PIN, supplying the extensor compartment.
- These arteries form extensive anastomoses around the elbow and wrist, providing collateral circulation.
Biomechanics of Forearm Rotation
Forearm pronation and supination are complex motions requiring the coordinated movement of the radius around the fixed ulna, driven by specialized muscles and stabilized by the interosseous membrane and articular capsules.
*
Supination
: Primary supinators are the biceps brachii (most powerful, especially with elbow flexion) and supinator muscle (most effective in full elbow extension).
*
Pronation
: Primary pronators are the pronator teres and pronator quadratus.
* The integrity of the radial head, DRUJ, and interosseous membrane, as well as the maintenance of the radial bow, are all critical for preserving the full arc of forearm rotation.
Indications & Contraindications
Surgical intervention in the forearm is indicated for a range of conditions, often involving fracture fixation, nerve decompression, tumor excision, or correction of deformity. The decision for operative versus non-operative management is based on a thorough assessment of fracture characteristics, neurovascular status, patient factors, and functional goals.
Indications for Operative vs. Non-Operative Management
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Forearm Fractures |
Adults:
- Displaced diaphyseal fractures of both radius and ulna (both-bone forearm fractures) - Displaced isolated radial or ulnar shaft fractures (often indicative of interosseous membrane injury or DRUJ/PRUJ disruption) - Open fractures - Pathological fractures - Segmental fractures - Floating elbow - Monteggia fractures (ulnar fracture with radial head dislocation) - Galeazzi fractures (radial fracture with DRUJ disruption) - Essex-Lopresti injuries (radial head fracture, interosseous membrane disruption, DRUJ dislocation) - Compartment syndrome |
Adults:
- Minimally displaced, stable isolated ulna shaft fractures (nightstick fracture) - Stress fractures - Select non-displaced radial head fractures (e.g., Mason Type I) - Distal radius fractures without significant instability or articular incongruity (e.g., Pilon, Colles, Barton type, etc.) |
|
Pediatrics:
- Highly displaced/unstable fractures (e.g., >10-15 degrees angulation, >50% cortical apposition, bayonet apposition in older children) - Open fractures - Fractures with neurovascular compromise - Irreducible fractures - Compartment syndrome |
Pediatrics:
- Minimally displaced or angulated fractures (often acceptable up to 10-15 degrees angulation, 50% cortical apposition, depending on age and location) - Greenstick fractures - Torus/buckle fractures - Growth plate injuries (Salter-Harris I/II) amenable to closed reduction and casting. |
|
| Nerve Compression |
Posterior Interosseous Nerve (PIN) Syndrome:
- Persistent, progressive motor weakness despite conservative management. - Surgical exploration for suspected mass or lesion compressing the nerve. - Confirmed compression at the Arcade of Frohse with electrodiagnostic studies and clinical correlation. Median Nerve (Pronator Syndrome/AIN Syndrome): - Persistent symptoms despite conservative management. - Surgical decompression for confirmed sites of compression. |
PIN Syndrome/Radial Tunnel Syndrome:
- Early presentation without significant motor deficit. - Conservative measures: rest, NSAIDs, steroid injections, physical therapy. Median Nerve: - Similar conservative approach for Pronator Syndrome. - AIN syndrome may have a higher rate of spontaneous recovery, but close monitoring is required. |
| Other Conditions |
- Forearm compartment syndrome (emergent fasciotomy)
- Bone tumors (excision, reconstruction) - Nonunion/malunion (corrective osteotomy, revision fixation) - Infection (debridement, irrigation, potentially hardware removal) |
- Mild tendinopathies (e.g., extensor carpi radialis tendinopathy)
- Minor soft tissue injuries - Stable chronic nonunion without significant pain or deformity (rare for forearm) |
Contraindications
Relative contraindications to surgery may include:
* Significant active infection (unless urgent debridement is required).
* Severe comorbidities precluding safe anesthesia (e.g., uncontrolled cardiac disease, respiratory compromise).
* Patient refusal or inability to comply with post-operative rehabilitation protocols.
* Poor soft tissue envelope precluding primary wound closure (may require staged approach or plastic surgery consultation).
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to ensure a predictable and safe surgical outcome, particularly given the intricate neurovascular anatomy of the forearm.
Pre-Operative Assessment
- Clinical Examination : Detailed neurovascular assessment (including specific testing for PIN function, median/ulnar nerve function, and vascular status), assessment of soft tissue integrity, range of motion (if possible), and pain mapping.
-
Imaging
:
- Plain Radiographs : AP and lateral views of the entire forearm, including the elbow and wrist joints, are essential. Oblique views may provide additional detail for complex fractures.
- Computed Tomography (CT) Scan : Indicated for complex articular fractures (radial head, distal radius, DRUJ), nonunions, or pre-operative planning for significant deformities. It helps delineate fracture patterns, comminution, and articular step-off.
- Magnetic Resonance Imaging (MRI) : Useful for assessing soft tissue injuries (ligamentous damage, interosseous membrane tears), stress fractures, osteomyelitis, or identifying masses compressing nerves (e.g., ganglia, lipomas causing PIN syndrome).
- Electrodiagnostic Studies (EMG/NCS) : Crucial for confirming nerve compression syndromes, localizing the site of compression (e.g., PIN at the Arcade of Frohse), and assessing the severity of nerve injury, especially prior to surgical decompression.
- Pre-operative Templating : For fracture fixation, templating with plates and screws can aid in selecting appropriate hardware size and length, particularly for complex comminuted fractures or cases requiring bone grafting.
- Discussion with Patient : Comprehensive discussion of risks, benefits, alternatives, and expected outcomes, including the potential for nerve injury and the need for rehabilitation.
Patient Positioning
The choice of patient position depends on the planned surgical approach and the location of the pathology.
*
Supine Position
: The most common position for forearm surgery.
* The arm can be placed on a hand table for distal forearm or wrist procedures, allowing for circumduction and fluoroscopy.
* For proximal forearm or elbow procedures, the arm can be extended on a padded arm board.
* Allows for easy access to the anterior (volar) and posterior (dorsal) aspects of the forearm by rotating the arm.
*
Lateral Decubitus Position
: May be considered for complex proximal forearm or elbow procedures requiring extensive posterior access, but is less common for isolated forearm shaft procedures.
*
Tourniquet
: A pneumatic tourniquet is routinely applied to the upper arm to provide a bloodless field, typically inflated to 250-300 mmHg for the duration of the procedure, with close monitoring of tourniquet time.
*
Sterile Prep and Drape
: Standard sterile preparation and draping from the axilla to the fingertips are performed, allowing full visualization and manipulation of the extremity.
Detailed Surgical Approach / Technique
Surgical approaches to the forearm must prioritize precise anatomical dissection, identification, and protection of neurovascular structures, particularly the PIN when working in the extensor compartment or near the proximal radius.
General Principles
- Tourniquet Control : Essential for clear visualization.
- Loupe Magnification : Recommended for precise dissection and nerve identification.
- Nerve Protection : Proactive identification and retraction of nerves are paramount.
- Internervous Planes : Utilizing known internervous planes minimizes muscle damage and denervation.
Surgical Approaches to the Forearm (Relevant to PIN)
1. Posterior Approach (Thompson Approach)
- Indications : Dorsal exposure of the radial shaft, particularly the middle and distal thirds, and access to the posterior interosseous nerve for decompression or exploration.
- Internervous Plane : Between the ECRB (radial nerve/PIN) and the ED (PIN). However, the more widely accepted and safer plane is between the ECRL/ECRB (radial nerve proper) and the Extensor Digitorum (PIN) proximally, and between the ED and the APL/EPB (both PIN innervated) distally. For exposure of the PIN directly, it's a direct incision through the supinator.
-
Technique
:
- Incision : A longitudinal incision is made on the dorsal aspect of the forearm, centered over the radial shaft.
- Subcutaneous Dissection : Careful dissection is performed to identify and protect cutaneous nerves, particularly branches of the superficial radial nerve in the distal forearm.
- Identify Mobile Wad : Identify the brachioradialis, ECRL, and ECRB (mobile wad) radially.
- Muscle Split : The plane is typically developed between the ECRB and the extensor digitorum. Retract the mobile wad (ECRL/ECRB) radially and the extensor digitorum ulnarly.
- Exposure of Supinator : As you proceed proximally, the supinator muscle will be exposed. The Posterior Interosseous Nerve (PIN) passes through the two heads of the supinator.
-
PIN Identification and Protection
:
- The PIN exits the radial nerve proper proximal to the supinator.
- The nerve enters the supinator through its superficial head, passing beneath the Arcade of Frohse , which is the proximal most fibrous edge of the superficial head.
- To expose the radial shaft proximal to the supinator or to decompress the PIN, the supinator muscle must be carefully incised parallel to its fibers, avoiding direct neurotomy. The PIN typically lies within the substance of the supinator, running obliquely from lateral to medial.
- The plane between the ECRB and the supinator can be developed to expose the radial neck and proximal shaft, with the PIN protected by the supinator.
- For complete exposure of the PIN and the proximal radius, the supinator can be elevated off the radius, or split longitudinally (blunt dissection recommended) to follow the nerve. Extreme care is required.
- Radial Shaft Exposure : Once the PIN is identified and protected, the supinator (with the PIN) is retracted ulnarly to expose the radial shaft. Distally, the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) originate from the posterior aspect of the radius and interosseous membrane; these muscles are also retracted ulnarly.

Figure 8: Posterior approach to the forearm, demonstrating retraction and exposure of deep structures.
2. Anterolateral Approach (Kaplan Approach)
- Indications : Proximal radial shaft fractures, radial head fractures requiring open reduction, or exploration of the proximal radial shaft. This approach allows for radial head and neck visualization while protecting the PIN.
- Internervous Plane : Between the brachioradialis (radial nerve proper) and the ECRB (radial nerve proper / PIN - variable).
-
Technique
:
- Incision : Longitudinal incision centered over the lateral epicondyle, extending distally along the line of the radial shaft.
- Dissection : The plane between brachioradialis and ECRL/ECRB is developed. Retract brachioradialis and ECRL radially.
- Identify PIN : The deep branch of the radial nerve (PIN) dives into the supinator muscle approximately 3-4 cm distal to the radial head. This is a critical anatomical landmark.
- Protection : The PIN is deep to the superficial head of the supinator and should be protected by keeping dissection close to the bone (subperiosteal) on the anterior aspect of the radial neck and shaft, or by carefully elevating the supinator muscle anteriorly. Avoid forceful retraction or instrumentation near the supinator.
3. Anterior Approach (Henry Approach)
- Indications : Volar exposure of the radial shaft and proximal radius, allowing access to the bicipital tuberosity.
- Internervous Plane : Between the brachioradialis (radial nerve proper) and the pronator teres/FCR (median nerve).
-
Technique
:
- Incision : Longitudinal incision on the volar aspect of the forearm, extending from the antecubital fossa distally.
- Dissection : Identify the interval between the brachioradialis and the flexor carpi radialis (FCR) or pronator teres (PT).
- Retraction : Retract the brachioradialis radially and the pronator teres/FCR/flexor mass ulnarly.
- Neurovascular Protection : The radial artery and superficial radial nerve lie deep to the brachioradialis and must be protected and retracted radially. The median nerve lies ulnar to the exposure, protected by the pronator teres and FDS.
- Radial Shaft Exposure : The supinator and pronator teres insert on the anterior aspect of the radial shaft. These muscles are released or elevated from the bone as needed for exposure.

Figure 9: Anterior (Henry) approach to the forearm, illustrating the internervous plane.
Fracture Reduction and Fixation Principles
-
Direct vs. Indirect Reduction
:
- Direct Reduction : Open reduction with direct visualization of fracture fragments, often necessary for articular fractures or highly displaced diaphyseal fractures.
- Indirect Reduction : Achieved through ligamentotaxis or external manipulation, often preferred for preserving soft tissue attachments and minimizing periosteal stripping, beneficial for biological healing.
-
Restoration of Anatomy
: Key goals include:
- Length : Restore anatomical length of both radius and ulna.
- Rotation : Ensure accurate rotational alignment.
- Alignment : Correct angulation and translation.
- Radial Bow : Crucial for maintaining forearm rotation. Loss of the radial bow by >10 degrees can lead to significant pronation/supination deficits.
-
Fixation
:
-
Plating (ORIF)
: Most common method for adult forearm fractures.
- Dynamic Compression Plates (DCP) / Limited Contact DCP (LC-DCP) : Provide rigid fixation.
- Locking Plates : Offer enhanced stability, especially in osteopenic bone or comminuted fractures, by creating a fixed-angle construct.
- Typically, 6-8 cortices of fixation on each side of the fracture are aimed for.
- Intramedullary Nailing : Can be used for isolated ulnar shaft fractures or in selected radial shaft fractures, particularly in pediatric patients (flexible nails). Less commonly used for adult diaphyseal radius fractures due to challenges in maintaining rotational control and radial bow.
- External Fixation : Indicated for open fractures with significant soft tissue injury, severe comminution, or as a temporary stabilizing measure.
-
Plating (ORIF)
: Most common method for adult forearm fractures.
PIN Decompression (for Radial Tunnel / PIN Syndrome)
- Approach : Most commonly via the dorsal (Thompson) or anterolateral (Kaplan) approach to the proximal forearm.
- Identification : The radial nerve is identified as it emerges from deep to the brachioradialis. Follow the deep branch (PIN) into the supinator.
-
Release of Constriction Points
: The PIN can be compressed at several points (the "five fibrous arches"):
- Fibrous bands anterior to the radial head.
- Vascular leash of Henry (recurrent radial vessels).
- Proximal edge of ECRB.
- Arcade of Frohse (most common site).
- Distal edge of the supinator.
- Technique : Carefully incise or release any constricting fibrous bands or muscle edges, particularly the Arcade of Frohse. The supinator muscle itself can be split longitudinally or partially released if it is hypertrophied or overtly compressing the nerve. Ensure full decompression along the entire course of the PIN through the supinator.
- Verification : Visual inspection of the nerve should reveal a healthy, non-constricted appearance.

Figure 10: Surgical exposure of the posterior interosseous nerve (PIN) and release of the Arcade of Frohse.
Complications & Management
Complications following forearm surgery can significantly impact functional outcomes. A thorough understanding of their incidence, recognition, and management strategies is paramount.
Common Complications and Management
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Nerve Injury |
PIN Palsy:
1-5% (iatrogenic during surgery, more common with proximal radius exposures)
SRN Neuroma/Injury: 5-15% (distal radial approaches) AIN Palsy: Rare (volar approaches) |
PIN Palsy:
- Immediate Post-Op: Observe for 3-6 months. Splinting for wrist/finger extension. Electrophysiological studies (EMG/NCS) at 3 months. - Delayed/No Recovery: Surgical exploration and neurolysis for persistent or worsening deficits. Tendon transfers (e.g., Pronator Teres to ECRB, FCR to ED, FDS to EPL/EPB) for irreversible PIN palsy to restore wrist extension, finger extension, and thumb abduction/extension. SRN Neuroma: Neuroma excision, nerve grafting, or burying nerve into muscle/bone. AIN Palsy: Observation; rarely requires exploration. |
| Nonunion | 5-15% (higher in open fractures, infection, severe comminution, poor reduction/fixation) |
Established Nonunion:
- Revision ORIF with plate exchange (locking plates), bone grafting (autograft/allograft), electrical stimulation. - Biomechanical optimization (e.g., dual plating for both bones, restoration of length/rotation). - Address infection if present. |
| Malunion | 10-20% (often related to inadequate radial bow restoration, rotational malalignment, shortening) |
Symptomatic Malunion (e.g., loss of pronation/supination, pain, DRUJ arthritis):
- Corrective osteotomy (radial, ulnar, or both), often with plating and bone grafting. - Darrach or Sauve-Kapandji procedures for symptomatic DRUJ arthritis. |
| Infection | 1-5% (superficial or deep) |
Superficial:
Oral antibiotics, wound care.
Deep/Hardware-related: Surgical debridement, irrigation, IV antibiotics, cultures. Retained hardware if stable and no signs of systemic infection. Removal of hardware if unstable or persistent infection. Staged reconstruction if severe. |
| Compartment Syndrome | Rare post-op, but critical pre-op/early post-op. | Acute: Emergent fasciotomy (volar and dorsal compartments). Maintain open wound and delayed closure/skin graft. Monitor nerve and muscle viability. |
| Hardware Failure/Prominence | 5-10% |
Failure:
Revision fixation, often with stronger implants, bone grafting if nonunion developing.
Prominence: Removal of symptomatic hardware after fracture healing (typically 12-18 months post-op). |
| Synostosis | 1-5% (often after severe trauma, open fractures, or combined radial/ulnar fixation) |
Early Post-Op (Progressive Loss of Rotation):
Aggressive therapy, splinting.
Established Synostosis (Symptomatic): Surgical excision of the bone bridge (often with interposition material like fat, muscle, or silicone sheeting) to restore forearm rotation. Timing of surgery is crucial (often waiting for bone maturity and quiescence). |
| Reflex Sympathetic Dystrophy (CRPS) | <1% | Early recognition and aggressive multimodal management: pain control (NSAIDs, neuropathic agents), physical and occupational therapy, sympathetic blocks, psychological support. |
| DRUJ Instability/Arthritis | Variable, depending on initial injury (e.g., Galeazzi, Essex-Lopresti) |
Instability:
Ligament reconstruction (TFCC repair/reconstruction).
Arthritis: Darrach procedure, Sauve-Kapandji procedure, hemiarthroplasty/total arthroplasty, or fusion (rare). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgical intervention itself in achieving optimal functional recovery. Protocols are individualized based on the injury type, surgical procedure, stability of fixation, and patient-specific factors.
General Principles
- Pain and Edema Control : Elevation, ice, pain medication.
- Early Motion (where permitted) : To prevent stiffness, promote cartilage nutrition, and optimize nerve gliding.
- Protection of Fixation : Initial immobilization or protected range of motion to allow for adequate bone and soft tissue healing.
- Progressive Strengthening : Once healing is established.
- Functional Training : Integration of the recovered extremity into activities of daily living.
Fracture Fixation (e.g., Radial/Ulnar Shaft ORIF)
-
Phase 1 (0-6 Weeks: Immobilization/Protected Motion)
:
- Goal : Protect surgical repair, manage pain/edema.
-
Intervention
:
- Initial splinting (e.g., sugar tong) or brace for comfort and protection.
- Early active range of motion (AROM) of uninvolved joints (shoulder, elbow flexion/extension, finger AROM).
- Gentle, protected passive range of motion (PROM) of the wrist and forearm (pronation/supination) may be initiated as early as 1-2 weeks post-op if fixation is rigid and surgeon allows.
- No lifting or weight-bearing.
-
Phase 2 (6-12 Weeks: Progressive Motion and Early Strengthening)
:
- Goal : Restore full range of motion, initiate gentle strengthening.
-
Intervention
:
- Discontinuation of formal immobilization, transition to removable brace if needed.
- Progressive AROM and PROM exercises for wrist, elbow, and forearm rotation (pronation/supination).
- Gentle isometric exercises.
- Light functional activities.
- Radiographic assessment of healing.
-
Phase 3 (12+ Weeks: Advanced Strengthening and Return to Activity)
:
- Goal : Maximize strength, endurance, and return to pre-injury activities.
-
Intervention
:
- Progressive resistive exercises (isotonics, isokinetics).
- Endurance training.
- Sport-specific or work-specific activities.
- Full weight-bearing as tolerated.
- Hardware removal considered typically after 12-18 months, if symptomatic or requested by patient.
Nerve Decompression (e.g., PIN Decompression)
-
Phase 1 (0-2 Weeks: Protection and Edema Control)
:
- Goal : Protect surgical site, allow nerve to recover.
-
Intervention
:
- Light splinting (e.g., wrist in neutral or slight extension) for comfort and to minimize tension on the nerve.
- Early gentle AROM of fingers, wrist, and elbow, avoiding extreme positions that might stretch the nerve.
- Nerve gliding exercises initiated cautiously.
-
Phase 2 (2-6 Weeks: Gentle Motion and Nerve Gliding)
:
- Goal : Improve nerve gliding, prevent adhesions, and monitor motor recovery.
-
Intervention
:
- Continued nerve gliding exercises.
- Gentle AROM for all joints.
- Passive motion initiated as tolerated.
- Close observation for return of motor function.
-
Phase 3 (6+ Weeks: Strengthening and Functional Reintegration)
:
- Goal : Strengthen recovering muscles, restore full function.
-
Intervention
:
- Progressive strengthening exercises as motor recovery progresses.
- Fine motor coordination exercises.
- If no motor recovery by 3-6 months, consider EMG/NCS and potentially further intervention or tendon transfers.

Figure 11: Example of post-operative splinting for wrist/finger extension, often used after PIN injury or tendon transfers.
Summary of Key Literature / Guidelines
Evidence-based practice is foundational to optimal outcomes in forearm surgery. Key literature and guidelines address various aspects, from fracture management to nerve compression syndromes.
-
Adult Forearm Fractures
: The AO Foundation principles emphasize anatomical reduction, stable internal fixation, and early functional rehabilitation. Studies consistently demonstrate superior outcomes with open reduction and internal fixation (ORIF) for displaced adult both-bone forearm fractures, leading to higher union rates and better functional scores compared to non-operative management.
- Radial Bow : The importance of restoring the radial bow is highlighted by numerous studies demonstrating compromised forearm rotation with even subtle angulation deformities (e.g., typically >10° of angular deformity can lead to significant loss of pronation/supination).
- Essex-Lopresti Injury : Requires prompt recognition and treatment, often involving radial head replacement, interosseous membrane repair, and DRUJ stabilization to prevent chronic pain, instability, and forearm shortening. Long-term outcomes are often guarded due to the severity of the initial injury.
- Pediatric Forearm Fractures : Management trends towards non-operative treatment for the majority of cases, emphasizing the significant remodeling potential in children. However, surgical intervention (often with flexible intramedullary nailing) is indicated for highly displaced, unstable, or open fractures, with strict parameters for acceptable angulation and translation based on age and fracture location.
-
Posterior Interosseous Nerve (PIN) Syndrome / Radial Tunnel Syndrome
:
- Diagnosis : Clinical presentation is often confusing, mimicking lateral epicondylitis. Electrodiagnostic studies (EMG/NCS) are often utilized to confirm nerve compression and rule out cervical radiculopathy or other neuropathies, though their sensitivity for radial tunnel syndrome can be low.
- Management : Initial management is typically conservative (rest, activity modification, NSAIDs, steroid injections). Surgical decompression is reserved for cases of persistent, debilitating pain (radial tunnel) or progressive motor weakness (PIN syndrome) after adequate conservative trial, or for cases with an identifiable compressive mass. Outcomes for PIN decompression for motor palsy are generally good, with variable success rates for pain relief in radial tunnel syndrome.
- Surgical Approaches : The Thompson and Kaplan approaches are well-described for PIN exposure, each with its advantages and risks. The Thompson approach often provides better visualization of the PIN through the supinator, while the Kaplan approach can be less invasive for certain proximal radial pathologies but requires meticulous care to avoid PIN injury.
- Complication Management : Protocols for nonunion (revision ORIF, bone grafting), malunion (corrective osteotomy), and infection (debridement, antibiotics) are well-established, emphasizing early recognition and aggressive intervention to prevent long-term disability. The management of synostosis is challenging, with surgical excision typically delayed until the bone bridge is mature and often combined with interpositional materials to prevent recurrence.
Continuous advancements in implant design, surgical techniques, and rehabilitation protocols continue to refine the management of forearm pathologies, underscoring the importance of staying abreast of current literature and expert consensus.
Clinical & Radiographic Imaging




