Mastering Screw Fixation for Displaced Extraarticular Humeral Fractures
Introduction & Epidemiology
Displaced extraarticular fractures of the proximal humerus, particularly those involving the greater tuberosity (GT), represent a significant proportion of shoulder trauma. While often categorized within the broader spectrum of proximal humeral fractures, isolated or dominant GT fractures present unique biomechanical challenges due to the formidable pull of the rotator cuff muscles. These fractures are typically extraarticular, avoiding disruption of the glenohumeral joint surface, which distinguishes them from more complex articular fractures.
Epidemiologically, proximal humeral fractures are the third most common fracture in adults over 65, following hip and distal radius fractures. While multi-part proximal humeral fractures garner substantial attention, isolated GT fractures, classified as AO/OTA 11-A1.2 (for displaced fragments) or Neer 2-part GT fractures, account for approximately 15-20% of all proximal humeral fractures. They often result from direct trauma to the shoulder or avulsion forces generated by sudden muscle contraction, frequently occurring in younger, active individuals involved in high-energy trauma, or in osteoporotic elderly patients following a fall.
The critical importance of restoring anatomical alignment in displaced GT fractures stems from the intimate relationship between the GT and the rotator cuff insertion. The supraspinatus and infraspinatus tendons insert onto the superior and posterior facets of the greater tuberosity, respectively. Displacement of this fragment, commonly observed superiorly and posteriorly due to the unopposed pull of these muscles, can lead to painful subacromial impingement, rotator cuff weakness due to a shortened lever arm, and restricted glenohumeral motion. Therefore, accurate reduction and stable fixation, often achieved through screw fixation, are paramount to optimize functional outcomes and prevent long-term sequelae.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the proximal humerus is fundamental for effective management of GT fractures.
Osseous Anatomy
The proximal humerus comprises the humeral head, anatomical neck, surgical neck, greater tuberosity, and lesser tuberosity. The greater tuberosity is a prominent bony projection located laterally on the humeral head. It serves as the primary insertion site for the supraspinatus, infraspinatus, and teres minor muscles. The supraspinatus inserts on the superior facet, while the infraspinatus inserts on the middle facet, and the teres minor on the inferior facet. The lesser tuberosity, anterior to the GT, provides insertion for the subscapularis tendon. The bicipital groove (intertubercular sulcus) separates the two tuberosities, housing the long head of the biceps tendon.
Vascular Supply
The vascularity of the humeral head primarily originates from the anterior and posterior humeral circumflex arteries, which anastomose to form the arcuate artery (ascending branch of the anterior humeral circumflex artery). This arcuate artery ascends within the bicipital groove and supplies the majority of the humeral head. While isolated GT fractures typically do not significantly compromise the main blood supply to the humeral head, extensive dissection during surgical approaches can risk injury to the ascending branches, emphasizing the need for meticulous technique.
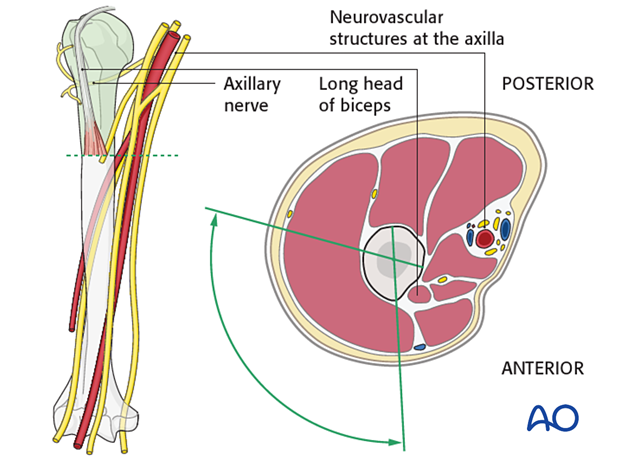
Neurological Structures
Several critical neurological structures are at risk during proximal humerus surgery. The axillary nerve is perhaps the most vulnerable, traversing posteriorly and inferiorly around the surgical neck of the humerus, approximately 5-7 cm distal to the acromion. It innervates the deltoid and teres minor muscles. The musculocutaneous nerve can be at risk with anterior approaches, particularly if dissection extends too far medially, supplying the coracobrachialis, biceps brachii, and brachialis. The radial nerve is located more distally but must be considered, especially with extensive humeral shaft exposure. Awareness of these "safe zones" for screw insertion and surgical dissection is paramount.
Biomechanics of Greater Tuberosity Fractures
The unique biomechanics of GT fractures dictate their characteristic displacement pattern and the rationale for surgical intervention. The rotator cuff muscles exert significant forces on the GT.
* The
supraspinatus
tendon pulls the fragment superiorly.
* The
infraspinatus
tendon pulls the fragment posteriorly.
* These combined forces lead to the typical superior and posterior displacement of the GT fragment.
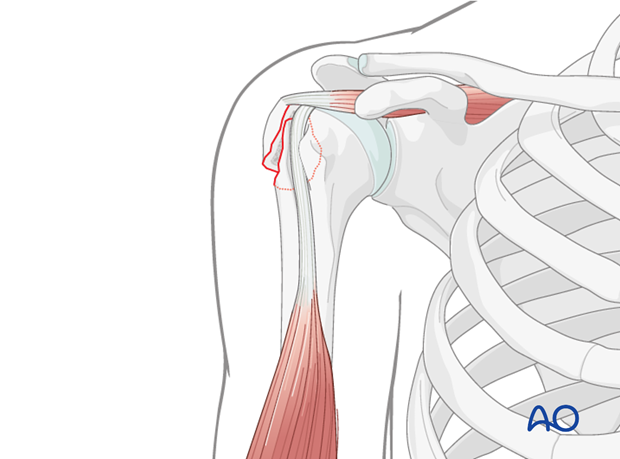
This illustration depicts a typical displaced greater tuberosity fracture (AO/OTA A1.2), highlighting the fragment's separation from the humeral head.
If the GT heals in a displaced position (typically >5 mm relative to the humeral head, though some literature suggests >3 mm for younger, active patients), it can lead to several adverse biomechanical consequences:
*
Subacromial Impingement:
The superiorly displaced fragment and its attached rotator cuff can impinge on the coracoacromial arch during shoulder elevation and abduction, causing chronic pain and restricted motion.
*
Rotator Cuff Dysfunction:
The displaced fragment alters the lever arm of the supraspinatus and infraspinatus, significantly weakening their ability to generate torque for abduction and external rotation. This biomechanical disadvantage impairs active shoulder motion.
*
Biceps Tendon Pathology:
The long head of the biceps tendon may become incarcerated within the fracture site or displaced from its groove, leading to pain and dysfunction.
*
Delayed Healing/Nonunion:
The powerful, unopposed muscle pull can contribute to continued displacement and micromotion at the fracture site, impeding bone healing.
Therefore, the primary surgical goals are to restore the anatomical position of the GT, re-establish the normal lever arm for the rotator cuff, prevent impingement, and ensure stable fixation to promote bone healing.
Indications & Contraindications
The decision to proceed with operative versus non-operative management for displaced extraarticular humeral fractures, particularly those of the greater tuberosity, requires careful consideration of fracture characteristics, patient demographics, functional demands, and comorbidities.
Operative Indications
Surgical intervention is generally indicated for displaced GT fractures when the displacement is deemed functionally significant and likely to lead to long-term sequelae if untreated.
*
Significant Displacement:
*
Translational Displacement:
Typically >5 mm in any plane (superior, posterior, medial). For young, active, high-demand patients, a threshold of >3 mm is often considered. This displacement is critical as it directly correlates with the risk of subacromial impingement and rotator cuff dysfunction.
*
Rotational Displacement:
Significant malrotation of the fragment, which can also disrupt normal shoulder kinematics.
*
Associated Injuries:
* Displaced GT fractures associated with glenohumeral instability (e.g., Bankart lesion, Hills-Sachs lesion) or subluxation.
* Associated rotator cuff tears requiring repair, especially if the GT fragment is small or comminuted.
* Biceps tendon incarceration or subluxation/dislocation requiring debridement or tenodesis/tenotomy.
*
Open Fractures:
Require urgent surgical debridement and stabilization.
*
Neurological Compromise:
Progressive neurological deficit associated with the fracture.
*
Failure of Non-Operative Management:
In rare cases where non-operative management was initially attempted for borderline displacement but failed due to progressive displacement or unacceptable pain/dysfunction.
*
Fracture Morphology:
Larger, singular GT fragments are generally more amenable to screw fixation and more likely to benefit from anatomical reduction.
Non-Operative Indications
Non-operative management is considered for patients with minimal displacement or those who are not surgical candidates.
*
Minimally Displaced Fractures:
Displacement less than 3-5 mm, where the risk of impingement and functional deficit is low.
*
Non-Displaced Fractures:
Stable, anatomically aligned fractures.
*
Elderly, Low-Demand Patients:
Individuals with significant comorbidities or limited functional expectations where the risks of surgery outweigh the potential benefits.
*
High Surgical Risk:
Patients with severe cardiac, pulmonary, or other medical conditions that contraindicate general anesthesia and surgery.
Contraindications
-
Absolute Contraindications:
- Active systemic or local infection.
- Severe soft tissue compromise (e.g., compartment syndrome, extensive open wounds, burns) precluding safe surgical access.
-
Relative Contraindications:
- Severe osteoporosis where bone quality is insufficient to achieve stable screw fixation. In such cases, alternative fixation methods like suture bridges or plate fixation might be considered, or even non-operative management if the patient's functional demands are low.
- Uncontrolled medical comorbidities that make the patient an unacceptably high anesthetic or surgical risk.
- Extremely comminuted GT fractures where a small fragment size precludes stable screw fixation.
Summary of Operative vs. Non-Operative Indications
| Indication | Operative Management | Non-Operative Management |
|---|---|---|
| Displacement (GT) | >5 mm (general); >3 mm (young, active patients) | <3-5 mm |
| Angulation | Significant malrotation or angular deformity | Minimal or no angular deformity |
| Rotator Cuff Impingement | High risk due to displacement (>5 mm) | Low risk |
| Patient Demand | High functional demand (active lifestyle, athlete) | Low functional demand (sedentary, elderly) |
| Associated Injuries | Glenohumeral instability, biceps incarceration, significant rotator cuff tear | None or minor |
| Open Fracture | Yes | No |
| Neurological Compromise | Progressive deficit | Stable neurological status |
| Comorbidities | Managed or low surgical risk | Unacceptably high surgical risk |
| Bone Quality | Sufficient for stable screw fixation | Severe osteoporosis precluding stable fixation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for successful outcomes in GT fracture fixation, encompassing comprehensive imaging, patient assessment, and precise positioning.
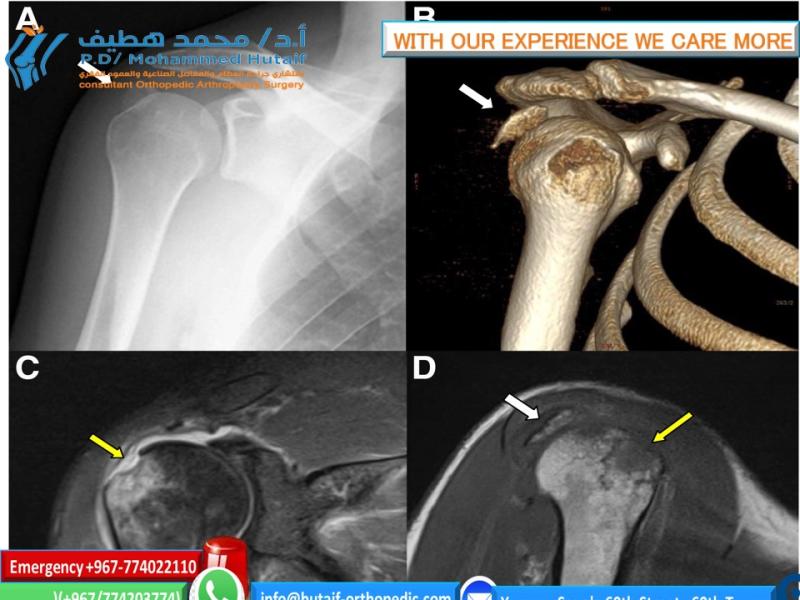
Imaging
-
Standard Radiographs:
- Anteroposterior (AP) view: Taken in the plane of the scapula (Grashey view), providing the best view of the glenohumeral joint space.
- Scapular Y view: Helps to assess anteroposterior displacement and angulation relative to the glenoid.
- Axillary view: Essential for determining medial-lateral displacement of the GT fragment and confirming its relationship to the humeral head. This view is often difficult to obtain in acute trauma settings due to pain, but crucial.
- Trauma Series: Additional views like a transthoracic lateral view may be useful in specific scenarios.
-
Computed Tomography (CT) Scan:
-
A CT scan with 3D reconstructions is highly recommended, if not mandatory, for displaced GT fractures. It provides invaluable information regarding:
- Precise assessment of displacement (translational and rotational).
- Fragment size and comminution, critical for planning screw trajectory and length.
- Articular involvement, though typically extraarticular, ruling out occult articular extension is important.
- Location of the biceps tendon and any potential incarceration.
-
Planning screw entry points and trajectory to avoid articular violation.
This image likely represents a CT scan or a schematic derived from CT data, aiding in detailed pre-operative assessment of fracture displacement and morphology.
-
A CT scan with 3D reconstructions is highly recommended, if not mandatory, for displaced GT fractures. It provides invaluable information regarding:
-
Magnetic Resonance Imaging (MRI):
-
While not routinely required for acute fracture diagnosis, an MRI can be beneficial in certain situations:
- To assess the integrity of the rotator cuff tendons, especially if a concomitant tear is suspected or if the fragment is very small (avulsion fracture).
- To confirm biceps tendon pathology (subluxation, dislocation, tearing, or incarceration).
- In cases of suspected ligamentous injury or glenohumeral instability.
-
While not routinely required for acute fracture diagnosis, an MRI can be beneficial in certain situations:
Patient Preparation & Positioning
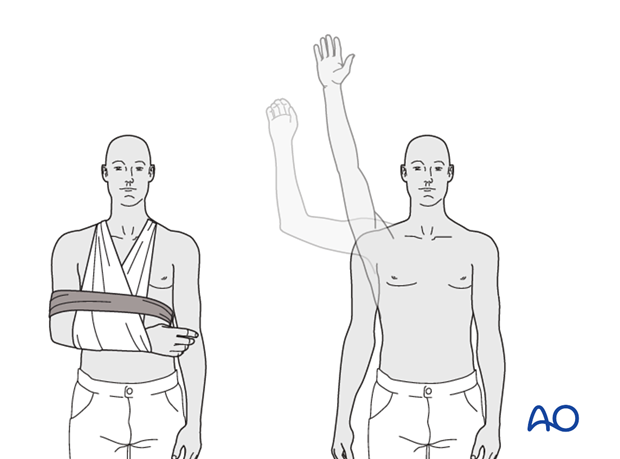
The optimal patient position for GT fracture fixation is the
beach chair position
, offering numerous advantages for exposure and manipulation.
*
Beach Chair Position:
* The patient is positioned semi-recumbent (30-70 degrees of trunk elevation).
* The head is secured in a headrest, ensuring the neck is neutral and venous drainage is uncompromised.
* The involved arm is draped free, allowing full manipulation (abduction, adduction, internal, and external rotation) to facilitate reduction maneuvers and confirm range of motion post-fixation.
* Padding is placed under pressure points (heels, sacrum, contralateral elbow).
* A beanbag can be used to stabilize the torso.
* This position allows for simultaneous access to the anterior and posterior aspects of the shoulder, should it be required, and facilitates fluoroscopic imaging.
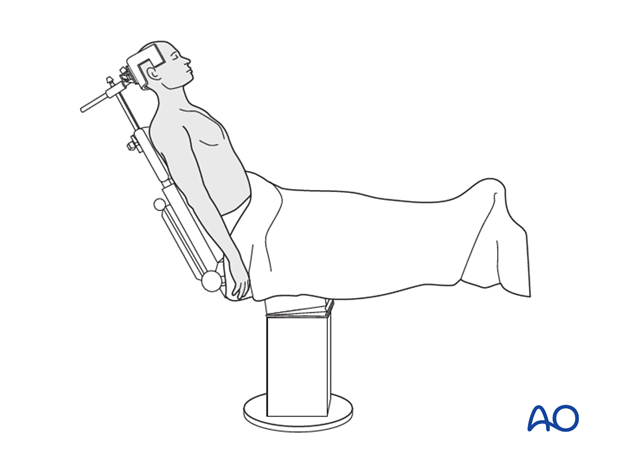
This illustration depicts a patient positioned in the beach chair configuration, which is standard for most shoulder procedures, including fixation of greater tuberosity fractures.
*
Fluoroscopy Setup:
* The C-arm fluoroscopy unit must be positioned to allow unobstructed AP, lateral (true scapular Y), and axillary views of the shoulder. It is critical to confirm the ability to obtain these views before draping.
*
Anesthesia:
General anesthesia is typically employed. A regional nerve block (e.g., interscalene block) can be considered pre-operatively for post-operative pain management, but its use during surgery may mask nerve irritation symptoms.
*
Sterile Preparation and Draping:
The shoulder and entire upper extremity, including the hand, are prepped and draped in a sterile fashion, allowing for full range of motion during the procedure.
Detailed Surgical Approach / Technique
The goal of surgical intervention is anatomical reduction of the greater tuberosity fragment and stable internal fixation, most commonly achieved with screw fixation.
Surgical Approach
The primary surgical approach for displaced greater tuberosity fractures is typically the deltopectoral approach , offering excellent visualization and broad access. In selected cases, often assisted by arthroscopy, a more limited deltoid-splitting approach may be considered for percutaneous screw placement, but this offers less exposure and increased risk of axillary nerve injury.
- Incision: A curvilinear skin incision is made from the coracoid process, extending distally along the deltopectoral groove for 8-10 cm.
- Deltopectoral Interval: The superficial fascia is incised, and the deltopectoral interval is identified. The cephalic vein typically lies within this groove and is carefully identified and retracted laterally with the deltoid, or ligated if necessary for improved exposure.
- Deep Dissection: The clavipectoral fascia is incised longitudinally, medial to the deltoid. This exposes the underlying conjoined tendon (coracobrachialis and short head of biceps) and the subscapularis muscle.
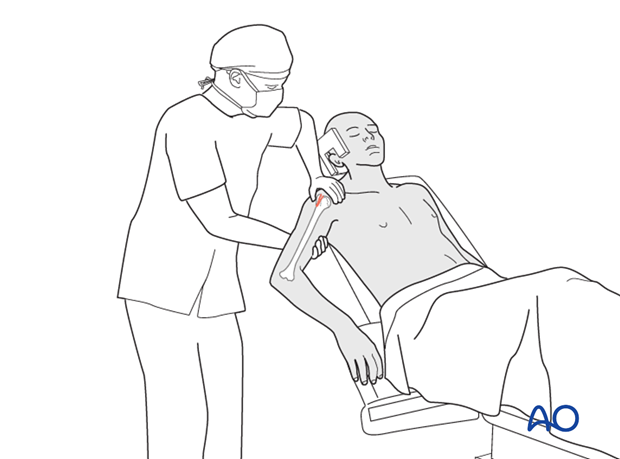
- Protecting the Axillary Nerve: Throughout the approach, constant vigilance is required to protect the axillary nerve. It runs roughly 5-7 cm distal to the acromial edge posteriorly. Careful, gentle retraction of the deltoid and avoiding excessive distal dissection are key.
-
Identifying the Fracture:
The fracture hematoma is evacuated, and the proximal humerus and the displaced greater tuberosity fragment are identified. The fragment is usually retracted superiorly and posteriorly by the supraspinatus and infraspinatus. Inspect the bicipital groove for integrity and position of the long head of the biceps tendon.
This image likely illustrates the initial exposure of the fracture site via the deltopectoral approach, revealing the displaced greater tuberosity fragment.
Reduction
Accurate reduction of the GT fragment is critical.
1.
Biceps Tendon Assessment:
First, assess the long head of the biceps tendon. It may be displaced, subluxated, or incarcerated within the fracture site. If incarcerated, it must be gently freed. If damaged or unstable, a tenodesis or tenotomy may be performed.
2.
Indirect Reduction:
Initial reduction attempts often involve gentle traction on the arm in slight abduction and external rotation. This can help to relax the rotator cuff and bring the fragment closer to its anatomical position.
3.
Direct Reduction:
* Using bone hooks or K-wires as joysticks, the GT fragment is carefully manipulated. The fragment typically needs to be pulled inferiorly and anteriorly to counteract the rotator cuff pull.
* Reduction clamps (e.g., pointed reduction forceps, Verbrugge clamp) can be applied carefully to compress the GT fragment back onto the humeral head.
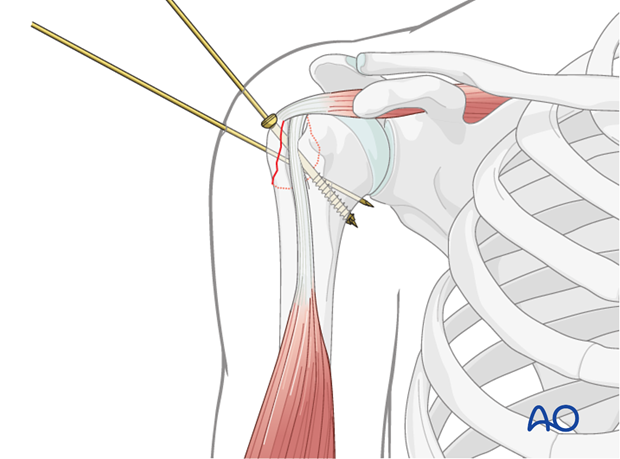
* Temporary K-wire fixation can be used to maintain reduction while definitive screw fixation is planned and applied.
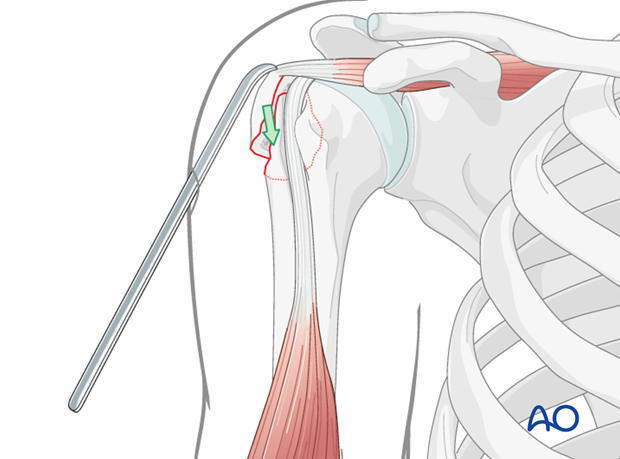
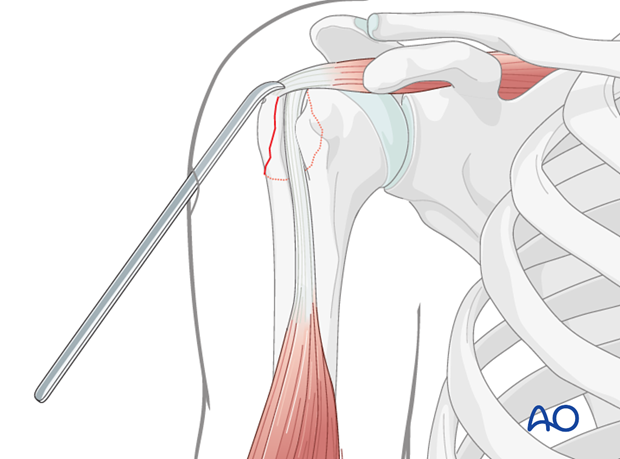
This image illustrates the use of a reduction instrument, likely a pointed reduction forceps, to manipulate and hold the greater tuberosity fragment in its anatomical position prior to definitive fixation.
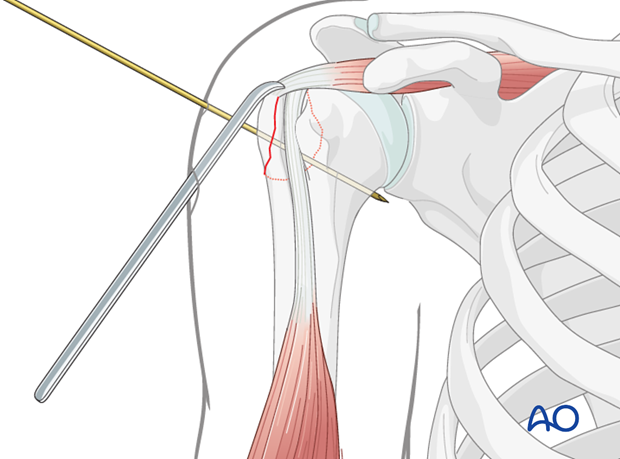
This image demonstrates the temporary K-wire fixation maintaining the reduced greater tuberosity fragment, a common step before inserting definitive screws.
Fixation with Screws
Screw fixation relies on adequate bone stock in both the fragment and the humeral head. The choice of screws depends on fragment size and bone quality.
1.
Principles of Screw Fixation:
*
Lag Screw Principle:
The primary goal is to achieve interfragmentary compression across the fracture line. This is accomplished using partially threaded screws where the threaded portion engages the far cortex (or cancellous bone within the humeral head), and the unthreaded portion slides through the near cortex (GT fragment). As the screw is tightened, the fragment is pulled towards the humeral head, creating compression.
*
Positional Screws:
Fully threaded screws can be used if fragment compression is not desired or feasible, acting more as neutralization screws to hold the fragment in position.
2.
Screw Selection:
*
Small fragment cortical screws:
Typically 2.7 mm or 3.5 mm diameter, either partially or fully threaded.
*
Headless compression screws:
Increasingly popular for GT fractures, especially for fragments that are large enough to accommodate them. They offer the advantage of being countersunk below the bone surface, minimizing soft tissue irritation and potential impingement, while providing excellent compression. Common sizes include 3.0 mm, 3.5 mm, or 4.0 mm.
3.
Screw Placement and Trajectory:
* Typically, 2 to 4 screws are used, depending on the size and comminution of the GT fragment.
* The screws are usually directed from the superior or posterolateral aspect of the GT into the cancellous bone of the humeral head.
*
Crucial consideration:
The trajectory must be carefully planned and executed under fluoroscopic guidance to ensure:
*
Optimal Compression:
Parallel to the long axis of the humeral shaft, engaging sufficient bone in the humeral head.
*
Avoid Articular Penetration:
Screws must not violate the glenohumeral joint space. This is confirmed with AP, lateral, and axillary fluoroscopic views.
*
Avoid Neurovascular Injury:
Maintaining screw placement within safe zones, away from the axillary nerve.
*
Secure Purchase:
Engaging dense cancellous bone or the far cortex for maximum hold.
This image demonstrates the drilling of the pilot hole for screw insertion after reduction and temporary fixation.
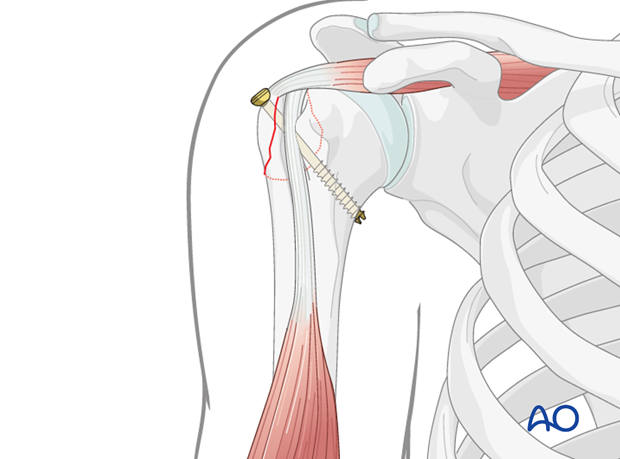
This image shows the measurement of screw length after drilling, ensuring appropriate purchase without violating the articular surface.
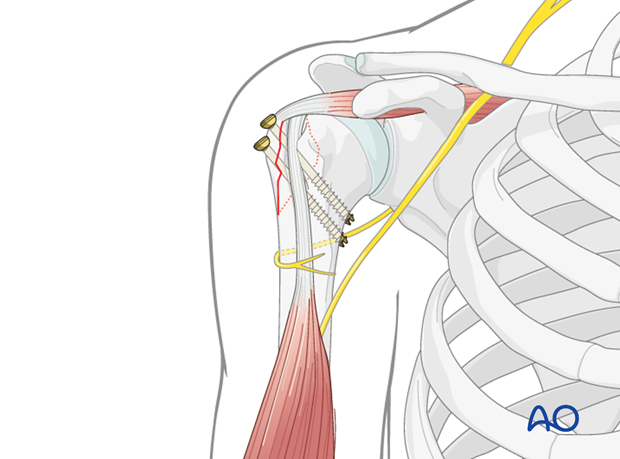
This image illustrates the final screw insertion, providing stable fixation of the greater tuberosity fragment.
This is likely a fluoroscopic image demonstrating optimal screw placement, confirming that the screws are entirely within the bone and not penetrating the joint.
-
Technique Steps (Lag Screw example):
- Drill Glide Hole: For the GT fragment, a drill bit matching the screw's outer diameter is used to drill a hole through the GT fragment. This is the "glide hole" which allows the screw to slide freely through the fragment.
- Drill Thread Hole: Using a smaller drill bit (matching the screw's core diameter), a pilot hole is drilled into the humeral head.
- Countersinking (Optional): If using a headed screw, countersinking the GT fragment can help seat the screw head flush and improve contact for compression. For headless screws, the design inherently allows countersinking.
- Measure Depth: A depth gauge is used to determine the appropriate screw length.
- Tap (if indicated): If using cortical screws in dense bone, tap the far segment. For cancellous screws, tapping may not be necessary in cancellous bone.
- Insert Screw: Insert the partially threaded screw and tighten gently to achieve compression.
- Repeat: Apply additional screws (typically 2-4) in a similar fashion.
- Suture Augmentation: In cases of comminution, osteoporotic bone, or when concomitant rotator cuff repair is performed, suture augmentation can be used in addition to screws. Sutures can be passed through the rotator cuff insertion on the GT and secured to the humeral shaft, providing additional rotational stability and compression.
Final Assessment
After fixation, the shoulder is taken through a full range of motion under fluoroscopic guidance to:
* Confirm stable fixation.
* Ensure no articular penetration of screws.
* Assess for any residual impingement or soft tissue restrictions.
* Confirm the ability to achieve full range of motion without redisplacement.
Wound Closure
The wound is irrigated thoroughly. The deltopectoral interval is loosely re-approximated, ensuring no tension. Subcutaneous tissue and skin are closed in layers. A sterile dressing is applied.
Complications & Management
Despite meticulous surgical technique, complications can arise following screw fixation for displaced greater tuberosity fractures. Prompt identification and appropriate management are crucial for optimizing patient outcomes.
Common Complications
| Complication | Incidence (approx.) | Salvage Strategy |
|---|---|---|
| Malunion/Nonunion | 10-30% |
Malunion:
If symptomatic (impingement, pain, weakness), revision osteotomy of GT with refixation; if severe and leading to early degenerative changes, shoulder arthroplasty (hemiarthroplasty or total shoulder arthroplasty).
Nonunion: Revision ORIF with bone grafting, potentially plate augmentation. |
| Hardware Prominence/Impingement | 10-20% | Surgical hardware removal after fracture union. For symptomatic impingement due to hardware, removal may be performed earlier. |
| Articular Penetration | 5-10% (can be higher with blind techniques) | Early revision surgery to remove and/or reposition offending screws. If significant articular damage has occurred, cartilage repair or arthroplasty may be considered in the long term. |
| Rotator Cuff Pathology | Variable (pre-existing or iatrogenic) | If persistent or new rotator cuff tear is symptomatic, surgical repair. This may involve formal rotator cuff repair and/or suture bridge augmentation of the GT fragment. |
| Shoulder Stiffness/Adhesive Capsulitis | 20-50% | Intensive physical therapy, manipulation under anesthesia (MUA) after ensuring fracture union, arthroscopic capsular release in refractory cases. |
| Infection (Superficial/Deep) | <2% |
Superficial:
Oral antibiotics, local wound care.
Deep: Surgical irrigation and debridement, IV antibiotics; hardware retention if stable and fracture healing is progressing, or hardware removal if fracture is united or deep infection persists. |
| Neurovascular Injury | <1% (Axillary nerve most common) |
Axillary Nerve:
Observation for motor recovery (up to 12-18 months). If no recovery, nerve exploration, neurolysis, or nerve grafting may be considered. Tendon transfers (e.g., latissimus dorsi) for persistent deltoid paralysis.
Vascular: Urgent surgical exploration and repair. |
| Avascular Necrosis (AVN) of Humeral Head | Rare in isolated GT, higher in multi-part fractures | Non-operative for early stages. Core decompression for early AVN. If progresses to collapse and pain, shoulder arthroplasty (hemiarthroplasty or total shoulder arthroplasty). |
| Hardware Failure/Pullout | 5-15% (especially in osteoporotic bone) | Revision surgery with stronger fixation (e.g., plate fixation, thicker screws), often with bone grafting or augmentation (e.g., calcium phosphate cement) for osteoporotic bone. |
| Complex Regional Pain Syndrome (CRPS) | <5% | Early diagnosis and multidisciplinary management: pain blocks, physical therapy, occupational therapy, psychological support, medications (neuropathic agents, bisphosphonates). |
Management Principles
- Early Recognition: Many complications are best managed with early recognition. Post-operative radiographs should be reviewed critically for articular penetration or loss of reduction. Persistent or worsening pain, unexplained swelling, or neurological deficits warrant immediate investigation.
- Imaging: Repeat radiographs, CT scans, or MRI may be necessary to fully characterize the complication.
- Patient-Specific Approach: Management decisions must be tailored to the individual patient, considering their functional demands, age, comorbidities, and the specific nature of the complication.
- Multidisciplinary Care: Management of complex complications, such as CRPS or significant neurovascular injury, often benefits from a multidisciplinary team approach involving pain specialists, neurologists, and physical therapists.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following screw fixation of a displaced greater tuberosity fracture is a carefully structured, phased program designed to protect the surgical repair while progressively restoring motion, strength, and function. The specific protocol will be modulated based on the stability of fixation, bone quality, any concomitant rotator cuff repair, and patient-specific factors.
General Principles
- Protection of Fixation: The primary goal in the early phase is to protect the fracture fixation from excessive stresses that could lead to redisplacement or hardware failure.
- Early, Controlled Motion: While protecting the repair, early initiation of controlled passive and then active-assisted motion is crucial to prevent stiffness, adhesion formation, and optimize cartilage health.
- Progressive Loading: Strengthening exercises are introduced gradually, respecting bone healing and soft tissue recovery timelines.
- Pain Management: Adequate pain control is essential to facilitate patient compliance with the rehabilitation program.
Phased Rehabilitation Protocol
Phase I: Immobilization and Early Protected Motion (Weeks 0-6)
Goals:
* Protect fracture fixation.
* Control pain and swelling.
* Initiate gentle, passive range of motion (PROM) to prevent stiffness.
Management:
*
Immobilization:
Arm in a sling (e.g., shoulder immobilizer) for 4-6 weeks. The duration depends on the surgeon's assessment of fixation stability and bone quality. The sling should be removed for exercises and personal hygiene.
*
Pain & Swelling Control:
Ice application, appropriate analgesia.
*
Exercises (Daily):
*
Elbow, Wrist, Hand AROM:
Encourage frequent active range of motion of the elbow, wrist, and hand to prevent stiffness and promote circulation.
*
Pendulum Exercises:
Gentle, gravity-assisted swings of the arm while leaning forward, to initiate glenohumeral motion without active muscle contraction of the shoulder.
*
Passive External Rotation:
Typically limited to 0-30 degrees initially, using the contralateral hand or a stick. Avoid stretching into painful ranges.
*
Passive Forward Flexion/Abduction:
Supported by a therapist or with the contralateral hand, within pain-free limits, usually not exceeding 90 degrees in the initial weeks.
*
Scapular Mobilization:
Gentle scapular retraction and protraction exercises.
*
Restrictions:
*
NO active shoulder motion.
*
NO lifting.
*
NO weight-bearing through the affected arm.
*
NO sudden movements or reaching overhead/behind the back.
Phase II: Active-Assisted Range of Motion (AAROM) and Gentle Strengthening (Weeks 6-12)
Goals:
* Gradually increase active range of motion.
* Initiate gentle strengthening of rotator cuff and scapular musculature.
* Improve neuromuscular control.
Management:
*
Progression:
Transition from sling to intermittent use or discontinue use as comfort and stability allow.
*
Exercises (Progressive):
*
Active-Assisted ROM (AAROM):
Using a stick, pulley system, or assistance from the contralateral arm to increase forward flexion, abduction, and external rotation (aiming for near full AROM by end of this phase).
*
Active Range of Motion (AROM):
Once AAROM is well-tolerated, progress to unassisted active motion as tolerated.
*
Light Isometrics:
Gentle, pain-free isometric exercises for the rotator cuff (internal/external rotation) and deltoid, with the arm in neutral or slight abduction.
*
Scapular Stabilization Exercises:
Progress with exercises for the rhomboids, trapezius, and serratus anterior.
*
Theraband Exercises:
Begin with very light resistance for internal and external rotation, scapular retraction.
*
Restrictions:
*
NO heavy lifting.
*
NO pushing or pulling activities.
*
Continue to avoid abrupt movements or extreme ranges.
Phase III: Progressive Strengthening and Return to Activity (Weeks 12-24+)
Goals:
* Achieve full, pain-free range of motion.
* Restore full strength and endurance of shoulder musculature.
* Facilitate return to sport or occupational activities.
Management:
*
Strengthening:
* Progressive resistive exercises for all major shoulder muscle groups (deltoid, rotator cuff, scapular stabilizers).
* Increase resistance and repetitions with elastic bands, light weights, and machine weights.
* Emphasis on eccentric training.
* Closed kinetic chain exercises.
*
Neuromuscular Re-education:
Proprioceptive exercises, balance, and coordination drills.
*
Functional Training:
Incorporate activity-specific or sport-specific movements.
*
Return to Activity:
Gradual return to activities of daily living (ADLs), occupational duties, and recreational sports. Full return to overhead sports or heavy manual labor may take 6 months or more, depending on individual progress and fracture healing.
*
Continued Home Program:
Emphasize the importance of maintaining a lifelong home exercise program to prevent recurrence of stiffness or weakness.
Key Considerations
- Bone Healing: Radiographic confirmation of fracture union is important before advancing to more aggressive strengthening.
- Individualization: Rehabilitation must be tailored to the individual's progress, pain levels, and specific goals.
- Communication: Close communication between the surgeon, physical therapist, and patient is paramount for successful outcomes.
- Complications: Be vigilant for signs of stiffness (adhesive capsulitis), persistent pain, or signs of hardware complications, which may require modification of the protocol or further investigation.
Summary of Key Literature / Guidelines
The management of displaced greater tuberosity fractures of the proximal humerus has evolved significantly, with screw fixation emerging as a reliable method for achieving anatomical reduction and stable internal fixation. A review of the literature provides crucial insights into current best practices.
Consensus on Displacement Thresholds
The critical displacement threshold for operative intervention in GT fractures remains a subject of ongoing debate, though a general consensus exists. Neer's initial classification suggested 5 mm of displacement as the criterion for a 2-part fracture, often necessitating surgical repair. More contemporary literature often advocates for a lower threshold, particularly in younger, active patients.
*
M.P. Neer (1970):
Emphasized that >5 mm displacement or >45 degrees angulation in multi-part proximal humeral fractures warrants surgical consideration.
*
Modern Consensus:
While >5 mm remains a widely accepted threshold, many surgeons consider >3 mm displacement in the GT fragment to be clinically significant, especially if associated with rotator cuff dysfunction or a high risk of impingement. This is particularly true for anterior or superior displacement, which directly correlates with impingement potential.
*
Cikic et al. (2014):
A systematic review highlighted that functional outcomes are superior with operative management for significantly displaced GT fractures compared to non-operative treatment, particularly for patients with higher functional demands.
Biomechanical Studies on Screw Configurations
Biomechanical studies have explored various screw fixation techniques for GT fractures, providing evidence for optimal stability.
*
Lag Screw Principle:
The use of lag screws to achieve interfragmentary compression is biomechanically superior for fracture stability compared to simple positional screws, as it reduces shear forces at the fracture site.
*
Screw Number and Trajectory:
Studies generally support the use of at least two, and often three or four, well-placed screws to provide adequate fixation, particularly against the strong pull of the rotator cuff. The screws should ideally traverse the fracture line perpendicularly to maximize compression and achieve good purchase in the dense cancellous bone of the humeral head.
*
Headless Compression Screws:
Several studies advocate for headless compression screws due to their low profile, which reduces the risk of subacromial impingement and soft tissue irritation post-operatively, while still providing robust compression.
*
Suture Augmentation:
Biomechanical models and clinical studies suggest that combining screw fixation with suture augmentation (e.g., suture anchors or transosseous sutures through the rotator cuff to the humeral shaft) can enhance rotational stability and resistance to pullout, especially in osteoporotic bone or when there's an associated rotator cuff tear.
Comparative Outcomes
While the primary focus is screw fixation, it's important to understand its place relative to other techniques.
*
Screw vs. Suture Fixation:
For large, single GT fragments, screw fixation generally offers more rigid and immediate stability, allowing for earlier mobilization. Suture fixation alone is often reserved for highly comminuted fragments or when screws cannot achieve adequate purchase, frequently used in conjunction with a plate or as a tension band.
*
Screw vs. Plate Fixation:
Plate fixation (e.g., locking plates) is typically reserved for more complex proximal humeral fractures (e.g., 3- or 4-part fractures involving the surgical neck) where stability of the tuberosities to the humeral shaft is also compromised. For isolated GT fractures, direct screw fixation is often less invasive and sufficient.
*
Arthroscopically-Assisted Fixation:
Arthroscopically-assisted percutaneous screw fixation has gained popularity, offering advantages of minimally invasive surgery, direct visualization of the articular surface to confirm anatomical reduction and rule out articular penetration, and simultaneous assessment/repair of intra-articular pathology (e.g., rotator cuff tears, biceps pathology). While technically demanding, studies have shown comparable outcomes to open fixation with potentially less soft tissue dissection.
Recent Trends and Ongoing Research
- Patient-Reported Outcome Measures (PROMs): The emphasis in clinical research has shifted towards patient-centered outcomes, evaluating functional scores (e.g., ASES, Constant-Murley, UCLA scores) and quality of life measures.
- Biological Augmentation: Research into the use of biological adjuncts (e.g., platelet-rich plasma, bone marrow aspirate concentrate) to enhance bone healing in conjunction with screw fixation is ongoing, particularly in cases of delayed healing or osteoporotic bone.
- 3D Printing and Pre-operative Planning: Advanced 3D printing of anatomical models based on CT data is being explored to allow for more precise pre-operative planning of reduction maneuvers and screw trajectories.
In conclusion, mastering screw fixation for displaced extraarticular humeral fractures, particularly those of the greater tuberosity, requires a profound understanding of surgical anatomy, biomechanics, appropriate indications, meticulous surgical technique, and a structured rehabilitation protocol. Adherence to established guidelines and a critical appraisal of new literature will continue to refine outcomes for these challenging injuries.
Clinical & Radiographic Imaging