
Proximal Humeral Fractures: Master Correct Plate Position for Optimal ORIF
Introduction & Epidemiology
Proximal humeral fractures represent approximately 5-6% of all fractures, ranking as the third most common fracture in individuals over 65, trailing only hip and distal radial fractures. The incidence is notably higher in elderly, osteoporotic women, typically resulting from low-energy falls. In younger, active populations, these fractures often occur due to high-energy trauma, frequently associated with additional injuries. The increasing global elderly population projects a continued rise in the incidence of these complex injuries, underscoring the importance of optimized treatment strategies.
The management of proximal humeral fractures is diverse, ranging from non-operative treatment to various surgical interventions, including open reduction and internal fixation (ORIF), intramedullary nailing, hemiarthroplasty, and reverse shoulder arthroplasty. The choice of treatment modality is dictated by numerous factors, including patient age, functional demands, bone quality, fracture morphology, and the presence of associated injuries. ORIF with locking plates has emerged as a widely accepted method for displaced and unstable fractures, aiming to restore anatomical alignment, provide stable fixation, and facilitate early rehabilitation. Despite advancements in implant design, complications such as avascular necrosis (AVN), nonunion, malunion, and hardware-related issues remain significant challenges, with correct plate positioning being a critical determinant of clinical success and complication avoidance.
Classification systems, primarily Neer and AO/OTA, are fundamental for communicating fracture characteristics and guiding treatment decisions. The Neer classification, based on the displacement of the four major segments (humeral head, greater tuberosity, lesser tuberosity, and humeral shaft), stratifies fractures into 2-, 3-, or 4-part injuries. The AO/OTA classification offers a more detailed, alphanumeric system that categorizes fractures by location, severity, and articular involvement. Accurate classification is imperative for both operative planning and prognostic assessment.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the proximal humerus is paramount for successful ORIF. The proximal humerus is a complex region, characterized by a spherical articular surface, the humeral head, which articulates with the glenoid. Key anatomical landmarks include the greater tuberosity (insertion of supraspinatus, infraspinatus, teres minor), lesser tuberosity (insertion of subscapularis), bicipital groove, and surgical neck.
The blood supply to the humeral head is critical for fracture healing and viability, primarily derived from the anterior and posterior circumflex humeral arteries. The arcuate artery, a branch of the anterior circumflex humeral artery, penetrates the humeral head through the bicipital groove and supplies the superior and anterior aspects. Damage to this tenuous blood supply, particularly in multi-part fractures with significant displacement or extensive soft-tissue stripping, significantly increases the risk of avascular necrosis.
Neurological structures in close proximity to the surgical field warrant meticulous protection. The axillary nerve, originating from the posterior cord of the brachial plexus, courses inferiorly and posteriorly to the surgical neck of the humerus, exiting the quadrangular space approximately 5-7 cm distal to the acromion. It supplies the deltoid and teres minor muscles and provides sensory innervation to the lateral shoulder. The radial nerve is also at risk, particularly during distal screw placement in the humeral shaft.
Biomechanical stability of the proximal humerus relies on both bone quality and integrity of the surrounding soft tissues, including the rotator cuff and joint capsule. The medial calcar region plays a crucial role in providing mechanical support against varus collapse, and its anatomical restoration is a key objective during fixation. Fractures often disrupt the load-bearing capabilities, and the goal of ORIF is to restore these biomechanical properties through stable internal fixation, allowing for early mobilization. Modern locking plates, with their fixed-angle constructs, provide improved stability in osteoporotic bone by creating an internal fixed-angle support system, independent of plate-to-bone compression.
Indications & Contraindications
The decision-making process for the treatment of proximal humeral fractures is multifactorial, balancing patient-specific factors with fracture characteristics. Non-operative management is often preferred for minimally displaced fractures, particularly in elderly patients with low functional demands or those with significant comorbidities precluding surgery. Operative intervention is generally indicated for displaced, unstable fractures where acceptable anatomical reduction and stable fixation are required to achieve optimal functional outcomes.
Indications
Operative Indications:
- Displaced 2-part fractures: Surgical neck fractures with significant angulation (>45 degrees) or displacement (>1 cm), or tuberosity fractures with significant retraction.
- 3-part fractures: Displaced greater or lesser tuberosity fractures combined with a surgical neck fracture.
- 4-part fractures: Especially those in younger, active patients, where preserving the humeral head is a priority, provided adequate reduction and fixation can be achieved.
- Fracture-dislocations: Proximal humerus fractures associated with glenohumeral dislocation.
- Open fractures: Require urgent debridement and stabilization.
- Neurovascular compromise: Acute vascular injury necessitating repair or progressive neurological deficit.
- Polytrauma patients: Often require early stabilization for pain control and mobilization.
- Young, active patients: Higher functional demands justify more aggressive interventions for optimal outcomes.
- Failed non-operative management: Progressive displacement or persistent pain.
Non-Operative Indications:
- Minimally displaced or stable 2-part fractures: Anatomical neck fractures with minimal displacement, surgical neck fractures with acceptable alignment (<45 degrees angulation, <1 cm displacement).
- Impacted fractures: Especially valgus-impacted fractures that are inherently stable.
- Elderly patients with low functional demands: When surgery carries high risks or expected functional gain is minimal.
- Significant comorbidities: Patients with medical conditions that contraindicate surgery (e.g., severe cardiopulmonary disease, uncontrolled diabetes).
- Severe osteoporosis: Where hardware purchase is poor, increasing the risk of cutout or failure (though locking plates have mitigated this to some extent).
Contraindications
Absolute contraindications for ORIF are rare but include active infection at the surgical site or a patient medically unfit for anesthesia and surgery. Relative contraindications encompass poor bone quality (severe osteoporosis), extensive soft-tissue compromise, severe communition precluding stable fixation, and patient non-compliance with post-operative rehabilitation. In such cases, alternative treatments like arthroplasty may be considered.
| Indication Type | Criteria for Operative Intervention | Criteria for Non-Operative Management |
|---|---|---|
| Fracture Pattern | Displaced 2-part (surgical neck >45° angulation, >1 cm displacement) | Minimally displaced 2-part (<45° angulation, <1 cm displacement) |
| 3-part fractures | Stable valgus-impacted 3-part fractures | |
| 4-part fractures (especially in younger patients) | ||
| Fracture-dislocations | ||
| Patient Factors | Young, active patients with high functional demands | Elderly, sedentary patients with low functional demands |
| Polytrauma patients requiring early mobilization | Significant medical comorbidities precluding surgery | |
| Acceptable bone quality for implant purchase | Severe osteoporosis with poor bone quality | |
| Associated Issues | Open fractures, neurovascular compromise | No associated neurovascular injury |
| Failed non-operative management |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful proximal humeral ORIF.
Imaging
Standard radiographic views, including true anteroposterior (AP) of the shoulder (Grashey view), scapular Y-view, and axillary view, are essential. A computed tomography (CT) scan with 3D reconstructions is highly recommended, especially for complex 3- and 4-part fractures, articular involvement, and precise assessment of tuberosity displacement. CT scans provide invaluable information regarding fracture morphology, fragment size, comminution, and bone stock, which directly influences implant selection and surgical strategy.
Templating and Implant Selection
Templating on radiographs, or increasingly with digital software using CT reconstructions, helps determine appropriate plate length, screw configuration, and potential need for bone grafting. The choice between a deltopectoral and an anterolateral approach can also be influenced by the fracture pattern and surgeon preference.
-
Plate Type:
Angular stable (locking) plates are the preferred implant for most displaced proximal humeral fractures, particularly in osteoporotic bone. These plates provide fixed-angle stability, reducing reliance on plate-bone compression and minimizing screw pullout. Standard plates, such as modified cloverleaf plates, may be considered in specific scenarios or when locking plates are unavailable.
- Plate Length: Should allow for at least three bicortical screws distal to the fracture in the humeral shaft.
- Screw Configuration: Locking screws are generally used in the humeral head, aiming for divergent trajectories to maximize purchase and construct stability. At least 4-6 head screws are recommended, with careful consideration for central calcar screws. Cortical screws are used distally in the shaft.
- Bone Grafting: Autogenous or allogenous bone graft (e.g., fibular strut graft, cancellous autograft) may be considered in cases of significant metaphyseal comminution or compromised medial calcar support to prevent varus collapse and promote healing.
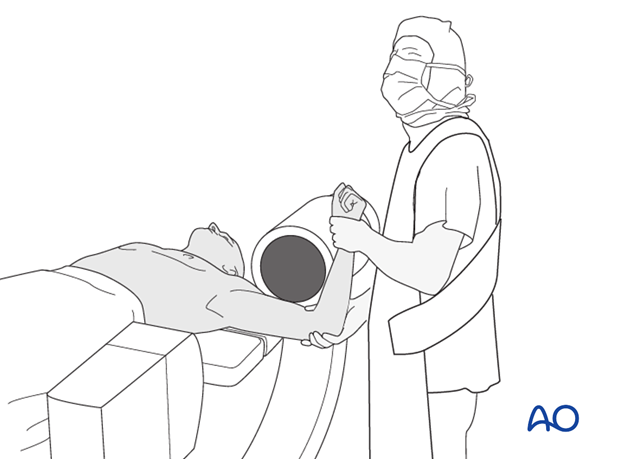
Patient Positioning
The patient is typically positioned in a supine or semi-beach chair position on a radiolucent operating table. The semi-beach chair position offers excellent access to the shoulder, reduces venous pressure, and minimizes bleeding. However, careful attention to cerebral perfusion is necessary. A sandbag or bolster is placed under the ipsilateral scapula to protract the shoulder, facilitating posterior access if needed and allowing the scapula to rotate freely. The arm is prepared and draped free to allow for full range of motion, crucial for reduction maneuvers and intraoperative fluoroscopic imaging. The image intensifier is positioned to allow orthogonal views (AP and axillary or outlet) without repositioning the patient. Anesthesia is typically general endotracheal, with regional block (interscalene brachial plexus block) often administered concurrently for post-operative pain management.
Detailed Surgical Approach / Technique
The surgical approach to the proximal humerus requires meticulous soft-tissue handling, precise anatomical reduction, and stable internal fixation. The choice of approach is often determined by the fracture pattern and surgeon preference.
1. Principles
Disimpaction: Disimpaction is paramount for successful reduction of these fractures. Often, the humeral head is impacted into the metaphysis, necessitating careful distraction and manipulation to restore anatomical length and alignment. This can be achieved with gentle traction, leverage, or specialized instruments.
Proper Reduction:
After disimpaction, reduction must restore correct alignment in both sagittal and coronal planes, along with appropriate rotational alignment. This includes:
*
Restoring Normal Valgus Alignment:
Crucial for stability and preventing varus collapse. The humeral head should be reduced against the plate, maintaining the anatomical valgus angle (typically 130-140 degrees).
*
Biceps Tendon Consideration:
Incarceration of the biceps tendon in the fracture site or between fragments can impede reduction. Careful inspection and release may be necessary.
*
Tuberosity Reduction:
Anatomical reduction of the greater and lesser tuberosities is essential for rotator cuff function and avoiding impingement.
Correct Plate Position: A correct plate position must be ensured to avoid loss of reduction, screw cutout, and subacromial impingement. This is a critical technical detail directly influencing long-term outcomes.
-
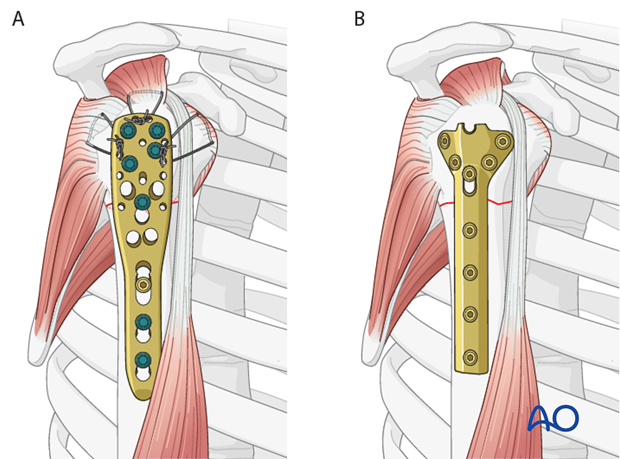
Angular stable versus standard plates:
This procedure describes proximal humeral fracture fixation with an angular stable plate (A). Sometimes, these implants are not available. Standard plates provide an alternative option, for example the modified cloverleaf plate (B). Presently, the specific indications, advantages, and disadvantages of angular stable and standard plates are being clarified. There is some evidence that angular stable plates provide better outcomes. In addition to type and technique of fixation, the quality of reduction, the soft-tissue handling, and the characteristics of the injury and patient significantly influence the results. There is no evidence that the use of angular stable plates will overcome these other factors.
2. Surgical Approach
A. Deltopectoral Approach
This is the most common approach for proximal humeral fractures, offering excellent visualization of the anterior and medial aspects of the proximal humerus and glenohumeral joint.
- Incision: A longitudinal incision is made from the coracoid process inferiorly along the deltopectoral groove for 10-15 cm.
- Dissection: The cephalic vein is identified within the deltopectoral groove and typically retracted laterally with the deltoid. Care is taken to protect it. The deltoid muscle is retracted laterally, and the pectoralis major medially, exposing the conjoint tendon and the clavipectoral fascia. The clavipectoral fascia is incised longitudinally to expose the coracobrachialis and short head of biceps.
- Internervous Plane: This approach utilizes the internervous plane between the deltoid (axillary nerve innervation) and the pectoralis major (medial and lateral pectoral nerves innervation).
- Deep Dissection: The anterior circumflex humeral artery and its branches, including the arcuate artery, are often encountered and should be meticulously preserved where possible. The axillary nerve typically lies 5-7 cm distal to the acromion and must be protected, especially when retracting the deltoid.
- Rotator Cuff Exposure: The subscapularis tendon can be identified and, if necessary for reduction or visualization of the humeral head, partially released from its insertion on the lesser tuberosity. Suture anchors can be used for later repair.
B. Anterolateral (Deltoid-Split) Approach
Less commonly used for complex fractures requiring extensive exposure, but can be useful for certain tuberosity or surgical neck fractures, particularly for direct visualization of the greater tuberosity.
- Incision: A longitudinal incision centered over the greater tuberosity.
- Dissection: The deltoid muscle fibers are split longitudinally, typically between the anterior and middle portions, taking care to avoid the axillary nerve which courses transversally 5-7 cm distal to the acromion. The length of the deltoid split should not exceed 5 cm to minimize the risk of axillary nerve injury.
- Advantages: Direct access to the greater tuberosity.
- Disadvantages: Limited exposure of the medial calcar and articular surface, higher risk of axillary nerve injury with extensive splitting.
3. Reduction Technique
- Initial Reduction: Gentle longitudinal traction on the arm is applied, often with an assistant, to disengage impacted fragments. External rotation of the arm can help reduce the greater tuberosity.
- Fragment Manipulation: K-wires, bone hooks, or reduction clamps (e.g., pointed reduction clamp, Verbrugge clamp) are used to manipulate fragments. Stay sutures placed through the rotator cuff tendons (supraspinatus, infraspinatus, subscapularis) can provide leverage for reducing and controlling the tuberosities and humeral head.
- Valgus Restoration: Restoring the valgus alignment of the humeral head relative to the shaft is critical. This often involves reducing the head onto the shaft in a slightly valgus position and ensuring the medial calcar is well-supported. A medial plate or strut graft can augment this support.
-
Temporary Fixation:
K-wires are frequently used to temporarily stabilize fragments in their reduced position prior to plate application. These should be placed strategically to avoid future screw paths.

4. Plate Application and Fixation
The ultimate goal is to achieve stable fixation while minimizing risks of impingement and hardware failure.
-
Plate Positioning:
This is the most critical step for optimal outcomes.
- Proximal-Distal Placement: The plate is positioned on the lateral aspect of the humerus. The superior edge of the plate should be placed approximately 5-8 mm distal to the superior aspect of the greater tuberosity (or slightly distal to the articular margin of the humeral head). This specific distance is crucial to prevent subacromial impingement, which can occur if the plate is placed too proximally, yet still allows for adequate purchase of the locking head screws in the humeral head. Intraoperative fluoroscopy with the arm abducted can confirm no impingement.
- Anterior-Posterior Placement: The plate is usually centered on the lateral aspect of the shaft, typically along the bicipital groove or slightly posterior to it. Avoid placing the plate too far anteriorly or posteriorly, which can compromise screw trajectories and increase nerve injury risk.
- Rotational Alignment: The plate should be aligned with the bicipital groove, which generally corresponds to the neutral rotation of the humeral head. Ensure the plate is not rotated, as this can lead to malreduction or malalignment.
-
Shaft Fixation:
- Once the plate is positioned correctly and provisionally secured (e.g., with K-wires or a holding clamp), the first screw is often placed in the oblong compression hole (if available) just distal to the fracture to achieve compression or to provisionally secure the plate. This can be a non-locking cortical screw to draw the plate to the bone.
- Subsequent screws in the shaft are typically locking screws, ensuring at least three bicortical locking screws distal to the fracture site.
-
Head Fixation:
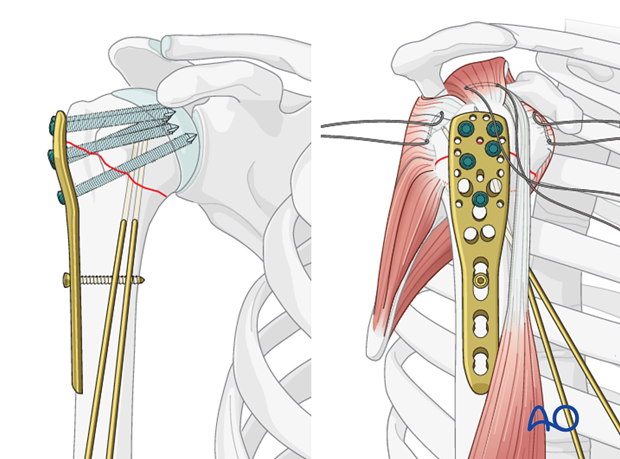
- Locking screws are drilled and inserted into the humeral head. The goal is to achieve divergent screw trajectories to maximize bone purchase and create a stable "cage" within the humeral head.
- Calcar Screws: At least one, preferably two, medial calcar screws are highly recommended. These screws are directed inferiorly and medially into the calcar region of the humeral head. They provide essential medial support, resisting varus collapse and improving construct stability, particularly in osteoporotic bone or comminuted fractures.
-
Screw Length and Penetration:
Fluoroscopy in multiple planes (AP and axillary) is essential to confirm appropriate screw length, ensuring screws do not penetrate the articular cartilage, which can lead to chondrolysis and pain. The screw tips should be flush with or slightly below the subchondral bone, typically 2-4 mm short of the articular surface.
- Suture Augmentation: Non-absorbable sutures can be passed through the holes in the plate and around the rotator cuff tendons (supraspinatus, infraspinatus, subscapularis, and teres minor) and their bone insertions. Tying these sutures provides additional rotator cuff repair, reinforces the reduction, and enhances fixation stability, particularly for tuberosity fragments.
- Final Assessment: Before closure, thoroughly assess the reduction and fixation stability under fluoroscopy, including passive range of motion to ensure no impingement and stability throughout the functional arc.
5. Wound Closure
After irrigation, close the rotator cuff if any portions were released. Repair the deltopectoral interval, and then close the subcutaneous tissues and skin in layers. A drain may be placed, though not always necessary.
Complications & Management
Despite advancements in surgical techniques and implants, complications following ORIF of proximal humeral fractures remain a significant concern, impacting patient outcomes and requiring revision surgery in a substantial proportion of cases.
Common Complications
- Avascular Necrosis (AVN) of the Humeral Head: Incidence ranges from 5-30%, significantly higher in 3- and 4-part fractures due to disruption of the humeral head blood supply. Risk factors include fracture type (especially 4-part), extensive soft-tissue stripping, and poor reduction. Management: Conservative for asymptomatic cases. For symptomatic AVN, treatment depends on pain, collapse, and patient age/demands, ranging from pain management to shoulder arthroplasty (hemiarthroplasty or reverse shoulder arthroplasty).
- Nonunion/Malunion: Nonunion rates vary, but can be up to 10-20%, particularly in osteoporotic bone, comminuted fractures, or poor reduction/fixation. Malunion (e.g., varus collapse, tuberosity malposition) can lead to pain, impingement, and functional deficits. Management: For nonunion, revision ORIF with bone grafting, or arthroplasty. For symptomatic malunion, osteotomy or arthroplasty.
- Screw Cutout/Loss of Fixation: Particularly problematic in osteoporotic bone, where screws may migrate through the humeral head articular cartilage. Often associated with varus collapse. Incidence up to 15-20%. Correct plate positioning, calcar screws, and anatomical reduction are crucial preventative measures. Management: Revision ORIF, hardware removal, or conversion to arthroplasty.
- Subacromial Impingement: Occurs when the plate is placed too proximally, causing irritation of the rotator cuff or subacromial bursa against the acromion, especially with arm abduction. Incidence can be 10-30%. Prevention: meticulous plate positioning 5-8 mm distal to the superior aspect of the greater tuberosity. Management: Hardware removal after fracture union, or revision surgery if severe and early.
- Infection: Superficial or deep wound infection. Incidence 1-5%. Management: Antibiotics, wound debridement, hardware removal (if deep infection and fracture union achieved).
- Nerve Injury: Axillary nerve injury is the most common, ranging from neuropraxia to complete transection. Radial nerve injury is less common but can occur during distal screw placement. Incidence 0.5-5%. Management: Observation for neuropraxia, neurolysis or repair if severe and persistent deficits.
- Stiffness/Adhesive Capsulitis: Common post-operatively due to immobilization and pain. Incidence 20-50%. Management: Aggressive physical therapy, pain control, glenohumeral injections, or manipulation under anesthesia/arthroscopic capsular release in refractory cases.
- Hardware Failure: Plate breakage or screw bending, often due to inadequate initial fixation or premature weight-bearing. Incidence 2-5%. Management: Revision surgery.
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Avascular Necrosis (AVN) | 5-30% | Conservative management (pain control), hemiarthroplasty, reverse shoulder arthroplasty (for symptomatic collapse/pain) |
| Nonunion / Malunion | 10-20% | Revision ORIF with bone grafting (autograft/allograft), osteotomy for malunion correction, conversion to arthroplasty (hemiarthroplasty or reverse shoulder arthroplasty) |
| Screw Cutout / Loss of Fixation | 10-20% | Revision ORIF with alternative fixation, hardware removal, conversion to arthroplasty (often reverse shoulder arthroplasty for severe cutout and poor bone quality) |
| Subacromial Impingement | 10-30% | Hardware removal (after fracture union), arthroscopic acromioplasty, revision plate positioning if ununited and severe |
| Infection | 1-5% | Antibiotics, surgical debridement, hardware removal (if deep and united), irrigation & debridement with retention of hardware (if stable fixation and early infection) |
| Nerve Injury (Axillary) | 0.5-5% | Observation for neuropraxia (up to 6-12 months), neurolysis, nerve grafting/repair for complete transection or persistent deficits |
| Stiffness / Adhesive Capsulitis | 20-50% | Intensive physical therapy, pain management, corticosteroid injections, manipulation under anesthesia, arthroscopic capsular release |
| Hardware Failure | 2-5% | Revision ORIF with stronger construct/plate, conversion to arthroplasty |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for achieving optimal functional outcomes and preventing stiffness while protecting the surgical repair. The protocol must be individualized based on fracture stability, bone quality, patient compliance, and surgeon preference. Generally, a phased approach is adopted.
Phase 1: Immobilization and Early Passive Range of Motion (0-6 weeks)
- Immobilization: The arm is typically placed in a sling for comfort and protection. The duration varies, but generally 2-4 weeks. Abduction slings or pillows may be used depending on fracture pattern and stability.
- Goals: Protect the repair, reduce pain and swelling, prevent stiffness of adjacent joints (elbow, wrist, hand).
-
Passive Range of Motion (PROM):
Initiated early (often within 1-2 weeks post-op for stable fixation) under strict guidance to prevent rotator cuff contracture and preserve glenohumeral motion.
- Pendulum exercises: Gentle, gravity-assisted swings.
- Supine PROM: Assisted external rotation, forward flexion (up to 90 degrees or as tolerated), and abduction (up to 90 degrees) with the therapist or the unaffected arm.
- Avoid: Active internal/external rotation, active abduction, and resisted exercises. Strict no-lifting restrictions.
- Activities: Emphasis on scapular mobility, elbow, wrist, and hand exercises to prevent stiffness.
Phase 2: Active-Assisted and Active Range of Motion (6-12 weeks)
- Goals: Gradually restore full, pain-free range of motion, improve muscle activation, and initiate light strengthening.
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM using pulleys, sticks, or the unaffected arm.
-
Active Range of Motion (AROM):
Once fracture healing is evident on radiographs (typically around 6-8 weeks), gentle AROM is introduced.
- Gradual progression: Forward flexion, abduction, external and internal rotation.
- Light Strengthening: Isometric exercises for the rotator cuff and deltoid, progressing to very light resistance bands.
- Avoid: Heavy lifting, sudden movements, or forceful stretching.
Phase 3: Progressive Strengthening and Functional Return (12+ weeks)
- Goals: Restore full strength, power, endurance, and functional capacity.
- Progressive Strengthening: Advance resistance exercises using bands, light weights, and bodyweight exercises. Focus on rotator cuff, deltoid, and scapular stabilizers.
- Proprioception and Neuromuscular Control: Introduce exercises using unstable surfaces or balance boards.
- Functional Training: Tailored to patient's activities of daily living, work, and recreational sports.
- Return to Activity: Gradual return to light activities typically begins around 3-4 months, with full return to sport or heavy labor often taking 6-12 months, depending on fracture consolidation and functional recovery.
- Hardware Removal: May be considered for symptomatic hardware (e.g., impingement, bursitis) typically after 12-18 months, once fracture healing is complete.
Throughout all phases, pain management, education on proper body mechanics, and adherence to activity restrictions are paramount. Regular clinical and radiographic follow-up is necessary to monitor fracture healing and guide rehabilitation progression.
Summary of Key Literature / Guidelines
The management of proximal humeral fractures, particularly with ORIF, continues to evolve, with ongoing research refining indications, techniques, and rehabilitation protocols.
Locking Plate Technology: Numerous studies and meta-analyses have consistently demonstrated the biomechanical superiority of locking plates over conventional non-locking plates, especially in osteoporotic bone. Locking screws create a fixed-angle construct, providing angular stability independent of plate-bone compression, thus reducing screw pullout and construct failure. However, clinical superiority in all fracture types and patient populations is not universally established. A 2013 Cochrane review found insufficient evidence to recommend one surgical intervention over another for proximal humeral fractures, highlighting the need for more high-quality comparative studies. More recent literature, such as the PROFHER trial (2015), suggested no significant difference in functional outcomes between ORIF and non-operative treatment for displaced proximal humeral fractures in adults. However, PROFHER has been critiqued for its broad inclusion criteria and high rate of protocol violations. The current consensus acknowledges that selected patients, particularly younger, active individuals with complex, unstable fractures, benefit from ORIF.
Importance of Correct Plate Position: The literature strongly emphasizes the critical role of accurate plate placement. Studies by Gardner et al. (2006) and others have clearly demonstrated that placing the plate 5-8 mm distal to the superior aspect of the greater tuberosity is crucial to avoid subacromial impingement. Malpositioning, especially proximal placement, is a common cause of pain and necessitates hardware removal. Optimal plate positioning also ensures adequate screw length and trajectory within the humeral head, specifically targeting the medial calcar.
Medial Calcar Support: The biomechanical significance of medial calcar support is well-documented. Augmentation with medial calcar screws or a strut graft (e.g., allograft fibula) has been shown to enhance construct stability and reduce the risk of varus collapse and screw cutout, particularly in comminuted or osteoporotic fractures (Sola et al., 2010; Chang et al., 2012). This concept has been integrated into modern plating systems and surgical techniques.
Suture Augmentation: The use of non-absorbable sutures passed through plate eyelets and around rotator cuff tendon insertions (suture-through-plate technique) has been shown to improve initial stability of tuberosity fragments and reduce the risk of secondary displacement, especially in osteoporotic bone. This technique provides additional compression and rotational stability to the tuberosities.
Avascular Necrosis (AVN) Prevention: While primary prevention of AVN remains challenging due to the nature of the injury, meticulous surgical technique, minimizing soft-tissue stripping, and anatomical reduction are paramount. Recent studies suggest that restoration of medial column support may indirectly help preserve blood supply by stabilizing the fracture and reducing further vascular compromise.
Future Directions: Research continues to focus on improving outcomes in elderly patients with osteoporotic bone, exploring novel biomaterials, augmented screw fixation, and comparing ORIF with arthroplasty options (hemiarthroplasty vs. reverse shoulder arthroplasty) for specific fracture patterns and patient demographics. The role of personalized surgical planning using 3D printing and navigation is also an area of emerging interest. Current guidelines underscore the need for shared decision-making, considering patient age, bone quality, fracture morphology, and functional demands when choosing the optimal treatment strategy.
