
Patient Presentation & History
A 38-year-old male, generally fit and healthy, presented to the emergency department following a fall from a height of approximately 15 feet while working on a construction site. He landed directly on his feet. He reported immediate, severe pain in his right ankle and foot, rendering him unable to bear weight. He denied any head injury, loss of consciousness, or other significant traumatic injuries. His past medical history was unremarkable, with no known allergies or regular medications. He was a non-smoker and consumed alcohol socially. The mechanism of injury, a high-energy axial load with possible varus or valgus component, immediately raised suspicion for complex intra-articular injuries to the hindfoot or ankle.
Clinical Examination
Upon arrival, the patient was hemodynamically stable.
*
Inspection:
The right ankle and foot were markedly swollen and ecchymotic, particularly dorsally and medially. There was a palpable deformity over the midfoot/hindfoot area. Skin integrity was preserved, with no open wounds, significant blistering, or areas of impending skin necrosis observed at initial presentation. However, the skin was tense, indicating significant soft tissue swelling.
*
Palpation:
Diffuse tenderness was elicited over the anterior ankle joint, talar neck, medial and lateral malleoli, and sinus tarsi. There was significant pain with any attempt to palpate the calcaneus or midfoot. Crepitus was noted with gentle manipulation. The integrity of the deltoid and lateral collateral ligament complexes was difficult to ascertain definitively due to pain and swelling, but gross instability was not appreciated.
*
Range of Motion (ROM):
Actively, the patient was unable to perform any ankle or subtalar motion due to excruciating pain. Passively, gross ROM was severely limited and painful.
*
Neurological Assessment:
Sensation to light touch was intact in all major dermatomes (sural, saphenous, superficial peroneal, deep peroneal, medial and lateral plantar nerves). Great toe extension and ankle dorsiflexion/plantarflexion were possible but severely limited by pain.
*
Vascular Assessment:
Dorsalis pedis and posterior tibial pulses were palpable and strong bilaterally. Capillary refill was brisk in all toes (<2 seconds). Compartment pressures were not initially elevated, but the extremity was closely monitored for any signs of developing compartment syndrome given the high-energy mechanism and significant swelling.
*
Systemic Assessment:
No other obvious injuries were identified on initial secondary survey.
Imaging & Diagnostics
Initial plain radiographs of the right ankle and foot were obtained in the emergency department.
*
Anteroposterior (AP) Ankle View:
Demonstrated widening of the medial clear space, suggesting a potential deltoid ligament injury or medial malleolar fracture, though a clear fracture line was not visualized.
*
Mortise View:
Showed subtle widening of the syndesmosis and increased talar tilt.
*
Lateral Ankle View:
Revealed a comminuted fracture involving the talar neck, with significant displacement and angulation. The fracture line extended into the subtalar joint. There was evidence of dorsomedial displacement of the talar head relative to the body, consistent with a severe talar neck injury. The body of the talus appeared posteriorly displaced and plantarflexed within the ankle mortise.
Given the complex nature of the injury and the significant articular involvement, a Computed Tomography (CT) scan of the right ankle and foot was immediately performed for comprehensive characterization of the fracture pattern and surgical planning.
*
CT Scan Findings:
*
Axial Views:
Confirmed a comminuted talar neck fracture with extension into the talar body and significant articular disruption of both the ankle and subtalar joints. Identified multiple small comminuted fragments.
*
Coronal Views:
Provided detailed insight into the articular surface involvement, particularly the superior aspect of the talar body within the ankle mortise, and the extent of comminution.
*
Sagittal Views:
Crucially demonstrated the degree of displacement and angulation of the talar head relative to the body. They clearly delineated the fracture extension into the posterior subtalar joint and the extent of plantarflexion and posterior migration of the talar body.
*
3D Reconstructions:
Offered an invaluable perspective on the overall deformity and helped visualize the spatial relationship of the fragments, aiding in pre-operative templating.
Following the CT scan, and prior to definitive surgical intervention, an Magnetic Resonance Imaging (MRI) scan of the right foot and ankle was obtained. This was considered essential for evaluating soft tissue integrity, cartilage status, and assessing the vascularity of the talar body, particularly given the high risk of avascular necrosis (AVN) associated with talar neck fractures. The initial plain radiographs and CT scan suggested a Hawkins Type III injury.
-
Crucial MRI Sagittal Insights:
The MRI sagittal images proved indispensable for a complete understanding of the injury pattern, exceeding the capabilities of CT for soft tissue and cartilage assessment.- Ligamentous Integrity: Sagittal views provided excellent visualization of the calcaneofibular ligament, posterior talofibular ligament, and particularly the deltoid ligament complex. In this case, significant edema and partial tearing of the deep deltoid ligament were noted, correlating with the medial clear space widening on X-ray. Sagittal images are also superior for assessing the interosseous talocalcaneal ligament, a critical stabilizer of the subtalar joint, which showed signs of disruption.
- Articular Cartilage Assessment: While CT shows bone, MRI sagittal views exquisitely demonstrate the integrity of the articular cartilage. We observed areas of chondral bruising and early subchondral edema on the talar dome, consistent with impaction. Furthermore, articular step-offs and incongruity in both the tibiotalar and subtalar joints were precisely quantified, guiding the need for meticulous anatomical reduction.
- Talar Head and Neck Morphology: The sagittal images provided a detailed profile of the fracture lines through the talar neck and body, allowing for precise measurement of anterior, posterior, and superior displacement and angulation. This was critical for understanding the extent of shortening and the specific vector required for reduction. They also helped identify small, non-displaced fracture lines or occult fractures that might be missed on CT, particularly in areas of complex anatomy.
- Subtalar Joint Involvement: The sagittal plane is paramount for evaluating the posterior facet of the subtalar joint. In our patient, the fracture clearly extended into this joint, with significant displacement of the posterior talar facet, highlighting the necessity for accurate reduction of this weight-bearing surface to prevent post-traumatic arthrosis.
- Associated Soft Tissue Injuries: Beyond ligaments, MRI sagittal views allowed assessment of surrounding tendons (e.g., flexor hallucis longus, posterior tibialis, Achilles tendon), demonstrating tenosynovitis or contusion which could impact post-operative recovery. Assessment of the posterior neurovascular bundle can also be achieved.
- Vascularity Assessment (Indirect): While direct visualization of vessels requires angiography, MRI provides indirect signs related to vascular compromise. The extent of fracture displacement and soft tissue injury can correlate with the risk of AVN. Advanced sequences, though not routine for initial trauma, can sometimes show perfusion changes.
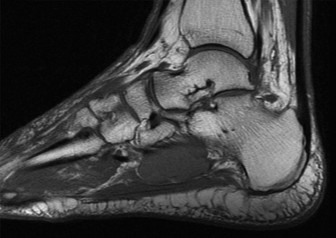
Figure 1: Representative Sagittal T2-weighted MRI image demonstrating a severely displaced talar neck fracture (Hawkins type III/IV). Note the significant angulation and posterior displacement of the talar body relative to the ankle mortise, and extensive bone marrow edema. The fracture line extends into the posterior subtalar joint. Soft tissue swelling and potential ligamentous injury are also evident.

Figure 2: Coronal T1-weighted MRI image from the same patient, highlighting the comminution of the talar neck and body, and involvement of the subtalar joint. The image further elucidates the articular damage and subchondral bone changes not fully appreciated on plain radiographs or CT.
Pre-operative templating was performed meticulously using the CT scans and 3D reconstructions to determine optimal screw length, trajectory, and plate positioning to achieve stable internal fixation while avoiding neurovascular structures and respecting articular surfaces.
Differential Diagnosis
Given the presentation of a high-energy axial load injury to the foot and ankle, several complex fracture patterns must be considered. While imaging clearly delineated a talar neck fracture in this specific case, the following table compares common differential diagnoses that share similar mechanisms and clinical presentations, emphasizing the role of imaging in differentiation.
| Feature | Talar Neck Fracture (e.g., Hawkins Type III) | Calcaneal Fracture (Intra-articular, Tongue or Joint Depression) | Pilon Fracture (e.g., Ruedi-Allgöwer Type III) | Lisfranc Injury (Homolateral/Divergent) |
|---|---|---|---|---|
| Mechanism of Injury | High-energy axial load (fall from height), forced dorsiflexion | High-energy axial load (fall from height), landing on heel | High-energy axial load (fall from height, MVC), impaction of talus into tibia | Axial load on a plantarflexed foot, direct crush, MVA |
| Clinical Presentation | Severe ankle/hindfoot pain, swelling, deformity, inability to bear weight. Possible open injury. | Heel pain, widening of heel, tenderness over calcaneus, ecchymosis (Mondor's sign). | Severe ankle pain, significant swelling, ecchymosis, often open injury. | Midfoot pain/swelling, inability to bear weight, plantar ecchymosis (pathognomonic). |
| Initial X-ray Findings | Talar neck fracture line, displacement/angulation, possible subtalar/ankle dislocation. | Loss of Böhler's angle, Gissane's angle disruption, increased calcaneal height/width. | Tibial plafond comminution, articular impaction, fibular fracture (often). | Widening between 1st/2nd metatarsal bases, loss of alignment (AP/oblique), fleck sign (avulsion). |
| CT Scan Utility | Defines comminution, displacement, articular involvement (subtalar/ankle), fragments. Critical for Hawkins staging. | Essential for Sanders classification, articular depression, sustentacular involvement. | Essential for Ruedi-Allgöwer/AO classification, articular comminution, bone loss. | Defines subtle displacement, impaction fractures, specific ligament avulsions. |
| MRI Sagittal Insights | Crucial for extent of articular cartilage damage, ligamentous injury (deltoid, interosseous), occult fractures, indirect vascular compromise signs. | Assesses soft tissue edema, peroneal tendon integrity, potential for compartment syndrome, subtle articular damage. | Evaluates cartilage integrity, syndesmotic injury, distal tibiofibular joint, posterior malleolar fragment extension. | Visualizes Lisfranc ligament disruption (primary injury), plantar plate tears, stress edema in midfoot bones. |
| Surgical Management | ORIF for most displaced fractures. External fixation for severe open injuries. | ORIF for displaced intra-articular fractures. | ORIF typically with staged approach, external fixation, fibular osteotomy. | ORIF with K-wires/screws for unstable injuries, primary arthrodesis for severe comminution. |
| Key Complications | Avascular necrosis (AVN), nonunion, malunion, post-traumatic arthrosis (ankle/subtalar). | Post-traumatic arthrosis (subtalar), peroneal impingement, sural nerve irritation, wound complications. | Post-traumatic arthrosis (ankle), infection, wound complications, nonunion. | Post-traumatic arthrosis, flatfoot deformity, chronic pain, hardware complications. |
Surgical Decision Making & Classification
The decision for operative intervention in this patient was straightforward. Given the severe displacement and comminution of the talar neck fracture, involvement of both the ankle and subtalar joints, and the high-energy mechanism, non-operative management would invariably lead to severe malunion, chronic pain, and profound functional impairment, including severe post-traumatic arthrosis of both the ankle and subtalar joints, and likely avascular necrosis of the talar body due to compromise of its blood supply.
The fracture was classified using the
Hawkins Classification System
for talar neck fractures:
*
Hawkins Type I:
Non-displaced vertical fracture of the talar neck. Low risk of AVN.
*
Hawkins Type II:
Displaced talar neck fracture with subtalar subluxation or dislocation, but the ankle joint remains congruent. Increased risk of AVN (20-50%).
*
Hawkins Type III:
Displaced talar neck fracture with both subtalar and ankle joint dislocation/subluxation. High risk of AVN (70-90%).
*
Hawkins Type IV (Canale and Kelly modification):
Displaced talar neck fracture with subtalar, ankle, and talonavicular joint dislocation/subluxation. Highest risk of AVN.
Based on the plain radiographs and CT scans showing significant displacement of the talar body posteriorly from the ankle mortise and dislocation of the subtalar joint, our patient’s injury was classified as a Hawkins Type III talar neck fracture . This classification mandates urgent operative intervention to achieve anatomical reduction and stable internal fixation, aiming to restore articular congruity and optimize the chances of revascularization of the talar body, thereby reducing the risk of AVN. The associated deltoid ligament injury further highlighted the need for open reduction to assess and potentially repair soft tissue damage contributing to instability.
Surgical Technique / Intervention
The surgical goal was anatomical reduction of the talar neck fracture and stable internal fixation to restore articular congruity of both the ankle and subtalar joints. Given the severity of the soft tissue swelling, a two-stage approach was considered but deemed unnecessary as the skin integrity was excellent and no fracture blisters or significant skin tension were present to preclude immediate surgery.
- Patient Positioning: The patient was positioned supine on a radiolucent operating table. A bump was placed under the ipsilateral hip to allow for neutral rotation of the limb. A tourniquet was applied high on the thigh. Image intensification (fluoroscopy) was positioned to allow for AP, lateral, and oblique views of the ankle and foot.
-
Surgical Approach:
A dual approach was utilized for optimal exposure and reduction:
- Anteromedial Approach: A curvilinear incision was made anterior to the medial malleolus, curving distally along the talar neck. The saphenous vein and nerve were identified and protected. The tibialis anterior tendon sheath was incised and retracted. This approach provides access to the medial aspect of the talar neck, the talonavicular joint, and facilitates reduction of medial displacement. The deep deltoid ligament was identified, and its injury confirmed.
- Anterolateral Approach (Sinus Tarsi Approach): A second curvilinear incision was made over the sinus tarsi, extending from the tip of the lateral malleolus towards the base of the fourth metatarsal. Care was taken to protect the superficial peroneal nerve branches. The extensor digitorum brevis muscle belly was elevated and retracted. This approach allows access to the lateral aspect of the talar neck, the lateral subtalar joint, and facilitates visualization of the posterolateral talar body.
-
Reduction Techniques:
- Initial Distraction: Longitudinal traction was applied to the foot to help disengage the impacted fragments and achieve ligamentotaxis. This was often augmented with a distracter (e.g., small external fixator or specialized traction device) across the ankle joint to gain space.
- Indirect Reduction: Using joysticks (K-wires inserted into the talar head and body fragments), gentle manipulation was performed under fluoroscopic guidance. The displaced talar body was notoriously difficult to reduce due to its plantarflexed and posteriorly migrated position. We used specific maneuvers involving dorsiflexion and distraction to guide the body back into the ankle mortise.
- Direct Reduction: Through both approaches, specific reduction instruments (e.g., pointed reduction clamps, bone hooks, dental picks) were used to anatomically reduce the talar neck fracture fragments. The talar head was aligned with the talar body, paying meticulous attention to rotational alignment. The posterolateral talar body, often displaced, was brought into reduction with careful elevation and anterior translation. Articular reduction of the subtalar joint was verified directly.
- Temporary Fixation: Once anatomical reduction was achieved, it was maintained with multiple K-wires placed percutaneously or through the approaches. Fluoroscopy was used extensively to confirm all planes of reduction.
-
Fixation Construct:
- Once reduction was deemed anatomical and stable with temporary K-wires, definitive internal fixation was applied. Typically, two to three cannulated screws (e.g., 3.5mm or 4.0mm) were inserted.
- Medial Screw: A screw was inserted from the medial talar neck, directed into the talar body, engaging the dense bone of the posterior process. This screw helped compress the fracture and prevent collapse.
- Lateral Screws: One or two screws were inserted from the lateral talar neck, directed into the talar body. Care was taken to ensure these screws provided good purchase without violating the articular surfaces of the subtalar or talonavicular joints.
- Screw Placement Considerations: Screws were placed in a divergent fashion to maximize stability. Due to the limited space and complex anatomy, careful planning of screw trajectory was paramount. All screws were countersunk to prevent soft tissue irritation.
- The fractured deep deltoid ligament was repaired with non-absorbable sutures through the anteromedial approach.
- Final fluoroscopic images in AP, lateral, and mortise views confirmed anatomical reduction and stable internal fixation.
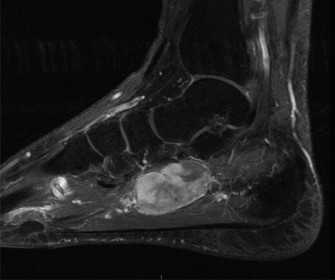
Figure 3: Intraoperative fluoroscopic image (lateral view) demonstrating stable internal fixation of a talar neck fracture with two cannulated screws. Note the anatomical alignment of the talar neck and body, restoration of the ankle and subtalar joint congruity. The distal screws achieve optimal purchase in the talar body.
Post-Operative Protocol & Rehabilitation
Post-operative management is crucial to optimize outcomes and minimize complications following a severe talar neck fracture.
-
Immediate Post-Operative Period (0-2 weeks):
- Immobilization: The limb was placed in a well-padded, bulky posterior splint or a removable CAM boot in a neutral position to protect the soft tissues and maintain fixation.
- Pain Management: Multimodal analgesia was initiated, including opioid and non-opioid medications.
- Wound Care: Wounds were monitored closely for signs of infection or skin complications. Dressings were changed as needed.
- Elevation: Strict elevation of the limb above heart level was maintained to reduce swelling.
- DVT Prophylaxis: Chemical prophylaxis (e.g., low molecular weight heparin) was initiated.
- Weight Bearing: Strict non-weight bearing (NWB) was maintained on the affected extremity.
-
Early Rehabilitation Phase (2-6 weeks):
- Cast/Boot: The splint was typically replaced with a non-weight-bearing short leg cast or CAM boot.
- ROM: Gentle, non-weight-bearing ankle and subtalar range of motion exercises were initiated around 2-3 weeks post-operatively, as pain and swelling allowed, to prevent stiffness. Active-assisted and passive ROM within pain limits were encouraged, often guided by a physical therapist. Care was taken not to stress the fracture site.
- Perfusion Monitoring: Ongoing vigilance for signs of AVN, although clinical signs are typically delayed.
-
Mid-Rehabilitation Phase (6-12 weeks):
- Imaging: Repeat radiographs were obtained at 6 weeks to assess fracture healing. If radiographic union was evident and pain free, gradual progression to partial weight-bearing (PWB) was initiated in a protective boot or brace.
- Strengthening: Progressive strengthening exercises for ankle dorsiflexors, plantarflexors, invertors, and evertors.
- Proprioception: Balance and proprioceptive training began as PWB commenced.
- Gait Training: Gradual transition from crutches to single crutch, then cane.
-
Late Rehabilitation Phase (12 weeks onwards):
- Full Weight Bearing: Once solid radiographic union was confirmed (typically 12-16 weeks), full weight-bearing was permitted.
- Advanced Strengthening: Continued strengthening, power development, and endurance training.
- Return to Activity: Gradual return to activities of daily living and eventually sport-specific training, guided by functional assessment.
- Monitoring: Long-term follow-up for potential complications such as post-traumatic arthrosis, AVN, or nonunion. Serial radiographs are essential, often extending for 1-2 years to monitor for AVN.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Pre-operative MRI is invaluable: While CT defines bone architecture, sagittal MRI views are paramount for assessing articular cartilage integrity, occult chondral/osteochondral lesions, ligamentous injuries (e.g., deltoid, interosseous talocalcaneal), and providing indirect information about talar vascularity. These insights critically inform surgical planning, particularly regarding the need for soft tissue repair and prognosis for post-traumatic arthrosis and AVN.
- Urgency is key: Displaced talar neck fractures, especially Hawkins Type III/IV, require urgent anatomical reduction to optimize blood flow to the talar body and minimize the risk of avascular necrosis. Delay beyond 6-8 hours significantly increases the risk.
- Anatomical Reduction is Non-Negotiable: Restoration of articular congruity of both the ankle and subtalar joints is the single most important factor for preventing post-traumatic arthrosis. This requires meticulous reduction of all displaced fragments, especially the posterior facet of the subtalar joint.
- Dual Approach: Often necessary (anteromedial and anterolateral/sinus tarsi) to achieve complete visualization and reduction of all fragments and to manage the soft tissue envelope effectively.
- Stable Fixation: Use divergent cannulated screws (typically 2-3) to achieve bicortical purchase in the talar body. The screws should be countersunk to prevent soft tissue irritation and avoid joint penetration.
- Soft Tissue Management: Meticulous handling of the soft tissues, careful flap creation, and identification/protection of neurovascular structures (saphenous nerve/vein medially, superficial peroneal nerve laterally) are critical to avoid wound complications and neurological deficits.
- Post-operative Surveillance: Long-term follow-up is mandatory, often for 2+ years, to monitor for avascular necrosis, nonunion, malunion, and the development of post-traumatic arthritis, which may necessitate secondary procedures such as ankle or subtalar arthrodesis.
- Hawkins Sign: While not a "pearl" for acute management, recognizing the Hawkins sign (subchondral lucency of the talar dome on plain radiographs, typically seen 6-8 weeks post-injury) is a favorable prognostic indicator suggesting viable talar body revascularization and a lower risk of AVN. Its absence, however, does not definitively confirm AVN.
Pitfalls
- Inadequate Reduction: Failure to achieve anatomical reduction, particularly rotational malalignment or residual step-offs/gaps >1-2mm, significantly increases the risk of post-traumatic arthrosis. Sagittal images are key in pre-op to fully grasp the 3D deformity.
- Missed Soft Tissue Injuries: Over-reliance on plain radiographs and CT alone can lead to missed significant ligamentous (e.g., deep deltoid, interosseous talocalcaneal) or chondral injuries that impact long-term stability and function. This is where MRI excels.
- Over-Distraction: While distraction aids reduction, excessive or prolonged distraction can strain vascular structures, potentially increasing the risk of AVN.
- Improper Screw Placement: Screws that are too long can violate articular surfaces or irritate soft tissues. Screws that are too short or poorly oriented may not provide adequate fixation. Avoid placing screws through the articular cartilage.
- Wound Complications: The talus has a tenuous soft tissue envelope. Aggressive retraction, prolonged surgical time, or excessive swelling can lead to skin necrosis, infection, or dehiscence. Staging the procedure for severe swelling can be prudent.
- Failure to Protect Neurovascular Structures: Injury to the saphenous nerve and vein medially or superficial peroneal nerve branches laterally can lead to chronic pain, numbness, or venous insufficiency.
- Premature Weight-Bearing: Initiating weight-bearing before adequate fracture healing or before ruling out early signs of AVN can result in fixation failure, nonunion, or collapse of the talar body.
- Complacency Regarding AVN: Avascular necrosis is a devastating complication. Even with anatomical reduction, the risk remains high for Hawkins Type III/IV fractures. Patients must be counselled appropriately, and long-term surveillance is crucial. Management of AVN can range from conservative to core decompression, vascularized bone grafting, or eventually arthrodesis.
