FOOT AND ANKLE AMPUTATIONS: TRANSTIBIAL (BELOW-KNEE) AMPUTATIONS
Following the seminal reports of Burgess and other pioneers who demonstrated successful transtibial amputations in more than 85% of patients with peripheral vascular disease, this procedure has firmly established itself as the most common major lower extremity amputation. The biomechanical and physiological importance of preserving the patient’s native knee joint cannot be overemphasized. Retention of the knee joint reduces the energy expenditure of ambulation by approximately 40% compared to a transfemoral amputation, dramatically increasing the likelihood of successful postoperative rehabilitation and independent community ambulation.
Although numerous variations in surgical technique exist, all transtibial amputation procedures are fundamentally bifurcated into two distinct categories based on vascularity: techniques for nonischemic limbs and techniques for ischemic limbs.
These two overarching methodologies vary primarily in the architectural design of the skin flaps and the specific muscle stabilization techniques employed. The appropriate level of amputation and the specific surgical approach must be meticulously determined for each individual patient, balancing the need for adequate soft tissue coverage, optimal prosthetic lever arm length, and the absolute necessity of primary wound healing.
BIOMECHANICS AND LEVEL SELECTION
Transtibial amputations can be conceptually divided into three levels: proximal, middle, and distal thirds of the tibia. The optimal level of amputation is traditionally chosen to provide a residual limb (stump) length that allows a controlling lever arm for the prosthesis, while ensuring sufficient vascular perfusion for primary healing and adequate soft tissue for protective end-weight bearing.
The Ideal Residual Limb Length
In adult patients, the ideal bone length for a transtibial amputation stump is 12.5 to 17.5 cm, depending on the patient's overall body height.
Clinical Pearl: The Rule of Thumb for Tibial Resection
A highly reliable, time-tested heuristic for selecting the level of bone section is to allow 2.5 cm of bone length for each 30 cm of patient body height. In standard practice, the most satisfactory and biomechanically efficient level is approximately 15 cm distal to the medial tibial articular surface.
Considerations for Suboptimal Lengths
- Distal Third Amputations: A longer residual limb theoretically provides a more normal gait appearance and a longer lever arm. However, stumps extending into the distal third of the leg are generally considered suboptimal. The distal third of the leg is relatively avascular, lacking robust muscle bulk, which leads to slower healing and less soft tissue available for distal padding. Furthermore, an excessively long stump leaves insufficient clearance within the prosthetic socket to accommodate modern energy-storing ankle-foot mechanisms.
- Short Stumps (< 12.5 cm): A stump less than 12.5 cm long is biomechanically less efficient due to the shortened lever arm, which increases the pressure exerted on the anterior distal tibia and posterior proximal socket during the stance phase of gait. Stumps lacking functional quadriceps control are essentially useless for prosthetic ambulation.
- Extremely Short Stumps (< 8.8 cm): Historically, in very short stumps, it was recommended to excise the entire fibula along with its associated muscle bulk to allow the stump to fit more easily into a prosthetic socket. However, modern prosthetists strongly advocate for the retention of the fibular head whenever possible. Contemporary total-contact sockets obtain superior purchase and rotational control on a short stump when the fibular head is preserved. Transecting the hamstring tendons to allow a short stump to seat deeper into the socket may be considered in extreme cases; while this weakens knee flexion, genu recurvatum has rarely been reported as a significant complication.
NONISCHEMIC LIMBS
Rehabilitation following transtibial amputations in nonischemic limbs is generally highly successful. This is largely attributable to the patient demographic, which typically comprises a younger, healthier population with fewer systemic comorbidities. Amputations in nonischemic limbs are most frequently necessitated by severe high-energy trauma, aggressive musculoskeletal tumors, intractable infections (e.g., chronic osteomyelitis), or severe congenital anomalies.
In these scenarios, the underlying pathology dictates the level of amputation and the choice of skin flaps. Advances in microvascular techniques have revolutionized limb salvage and amputation surgery, making the preservation of functional transtibial stumps possible through the use of distant free tissue transfers and "spare part" fillet flaps harvested from the amputated distal limb.
Muscle Stabilization: Myodesis vs. Myoplasty
In nonischemic limbs, robust muscle stabilization techniques are paramount to prevent muscle atrophy, provide a dynamic distal cushion, and enhance venous return.
* Tension Myodesis: Transected muscle groups (primarily the gastrocnemius-soleus complex and anterior compartment musculature) are sutured directly to the distal tibia through pre-drilled osseous holes under physiological tension. This provides the firmest stabilization and is highly advocated in young, active, and athletic individuals.
* Myoplasty: Muscle is sutured to opposing soft tissue structures, such as antagonistic muscle groups or deep fascia over the distal bone end. While myoplastic closures are more frequently performed due to technical ease, they offer slightly less rigid stabilization than myodesis.
🔪 Surgical Technique 11-1: Classic Transtibial Amputation (Nonischemic)
The classic approach utilizes equal anterior and posterior flaps, providing excellent coverage and a centralized distal scar.
Positioning and Preparation:
* Place the patient supine on the operating table.
* Apply a well-padded pneumatic tourniquet to the proximal thigh to ensure meticulous hemostasis during the dissection.
Incision and Flap Design:
* Beginning proximally at the anteromedial joint line, measure distally to the desired length of bone resection (typically 15 cm), and mark that level over the tibial crest with a sterile skin marking pen.
* Outline equal anterior and posterior skin flaps. The length of each flap must be exactly equal to one-half the anteroposterior diameter of the leg at the anticipated level of bone section.
* Begin the anterior incision medially or laterally at the intended level of bone section. Swing it convexly distalward to the previously determined flap apex, and then proximally to end at a corresponding position on the opposite side of the leg.
* When crossing the tibial crest, deepen the incision sharply through the periosteum and mark the bone with a scalpel cut to establish a fixed point for future measurement.
* Begin the posterior incision at the same medial/lateral apices as the anterior incision. Carry it first convexly distalward and then proximally, mirroring the anterior incision.
* Deepen the posterior incision through the dermis, subcutaneous fat, and deep fascia, but do not separate the skin or deep fascia from the underlying muscle mass, as this preserves the critical musculocutaneous perforators.
Anterior Dissection:
* Reflect the anterior flap as a single, full-thickness layer containing skin, subcutaneous tissue, deep fascia, and periosteum over the anteromedial surface of the tibia.
* Continue this subperiosteal dissection proximally to the level of intended bone section.
* Crucial Step: Because the anterior flap contains elastic tissues that contract upon incision, it cannot be reliably used to measure the level of intended bone section retrospectively. Instead, utilize the mark previously made in the tibial periosteum to reestablish the exact level of bone section. Mark the bone at this point with a saw.
Nerve and Vessel Management (Anterior/Lateral):
* Insert a curved hemostat into the natural cleavage plane at the lateral aspect of the tibia. Guide its tip along the interosseous membrane, passing over the anterior aspect of the fibula to emerge just anterior to the peroneus brevis muscle.
* Identify and isolate the superficial peroneal nerve in the interval between the extensor digitorum longus and peroneus brevis. Apply gentle distal traction, divide it sharply high with a fresh scalpel blade, and allow it to retract well proximal to the end of the stump, burying it deep within the muscle belly to prevent neuroma formation.
* Divide the muscles in the anterior compartment of the leg at a point 0.6 cm distal to the level of bone section. This slight distal allowance ensures the muscle retracts perfectly flush with the end of the bone.
* During sectioning, meticulously identify, isolate, and protect the anterior tibial vessels and the deep peroneal nerve.
* Ligate and divide the anterior tibial vessels just proximal to the level of intended bone section.
* Exert gentle traction on the deep peroneal nerve, divide it sharply, and allow it to retract proximally.
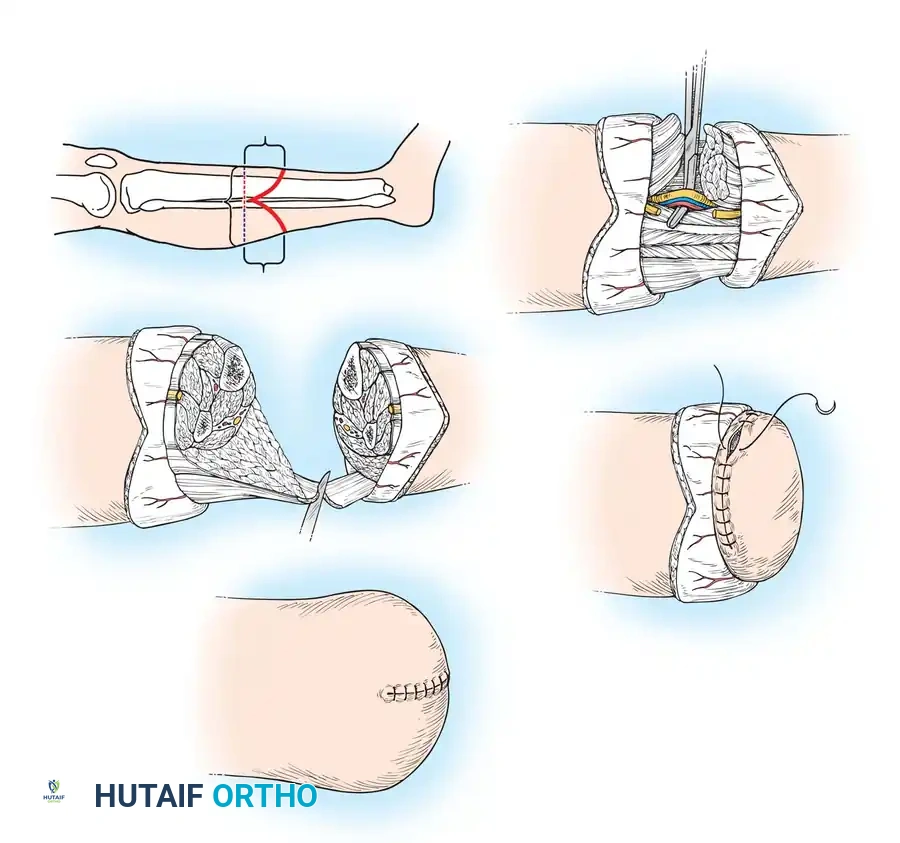
Bone Resection:
* Before sectioning the tibia transversely, bevel its anterior crest. Begin the bevel cut 1.9 cm proximal to the level of the transverse bone section, cutting obliquely distalward to cross the transverse level 0.5 cm anterior to the medullary cavity. This prevents a sharp bony prominence from eroding through the anterior skin flap.
* Section the tibia transversely with an oscillating saw.
* Section the fibula 1.2 to 1.5 cm proximal to the level of the tibial resection. A fibula left too long will bear disproportionate weight and cause severe prosthetic socket pain.
* Grasp the distal segments of the tibia and fibula with heavy bone-holding forceps. Pull them anteriorly and distally to expose the deep posterior muscle mass.
Posterior Dissection and Closure:
* Divide the muscles in the deep posterior compartment 0.6 cm distal to the level of bone section. This exposes the posterior tibial vessels, peroneal vessels, and the tibial nerve lying on the anterior surface of the gastrocnemius-soleus muscle group.
* Doubly ligate and divide the vessels. Apply gentle traction to the tibial nerve, section it sharply, and ensure it retracts well proximal to the bone end.
* With a large amputation knife, bevel the gastrocnemius-soleus muscle mass to form a robust myofascial flap long enough to reach across the end of the tibia to the anterior fascia.
* Smoothly round the cut ends of the tibia and fibula with a bone rasp. Copiously irrigate the wound with sterile saline to remove all bone dust, which can cause heterotopic ossification.
* Deflate the tourniquet. Achieve meticulous hemostasis via electrocautery and suture ligation of all bleeding points.
* Bring the gastrocnemius-soleus muscle flap anteriorly over the ends of the bones. Suture it securely to the deep fascia and the periosteum anteriorly (Myoplasty) or through drill holes in the tibia (Tension Myodesis).
* Place a closed-suction drain deep to the muscle flap, bringing it out laterally through the skin 10 to 12 cm proximal to the stump end.
* Tailor the skin flaps to eliminate "dog ears" and ensure a smooth, tension-free closure. Suture the skin edges with interrupted nonabsorbable sutures.
ISCHEMIC LIMBS
Patients presenting with ischemic limbs (typically due to severe peripheral arterial disease, often compounded by diabetes mellitus) possess significant systemic comorbidities. This demands stringent precautionary measures, comprehensive preoperative optimization, and close multidisciplinary interaction with a vascular surgical team.
Because the vascular arborization to the skin is significantly more robust on the posterior and medial aspects of the leg (supplied by the sural and posterior tibial arteries) compared to the anterior or anterolateral sides (supplied by the often-occluded anterior tibial artery), transtibial amputation techniques for the ischemic limb are fundamentally characterized by skin flaps that favor the posterior and medial leg.
Surgical Warning: Contraindications in Ischemic Limbs
1. Tension Myodesis: Suturing muscle to bone under tension is strictly contraindicated in ischemic limbs, as the tension will strangulate the microcirculation and precipitate muscle necrosis.
2. Tourniquet Use: The use of a pneumatic tourniquet is generally avoided to prevent further ischemic insult to already compromised tissues and to allow real-time assessment of tissue viability and bleeding during the procedure.
The long posterior flap technique, popularized by Burgess, remains the gold standard. However, alternative techniques such as equal medial and lateral flaps (Persson), skew flaps, and long medial flaps are utilized depending on specific angiographic perfusion patterns. All techniques for ischemic limbs stress the absolute necessity of preserving intact vascular connections between skin and muscle by avoiding dissection along superficial tissue planes, thereby constructing true myocutaneous flaps. Furthermore, amputations in ischemic limbs are customarily performed at a slightly higher level (e.g., 10 to 12.5 cm distal to the joint line) to ensure adequate perfusion for healing.
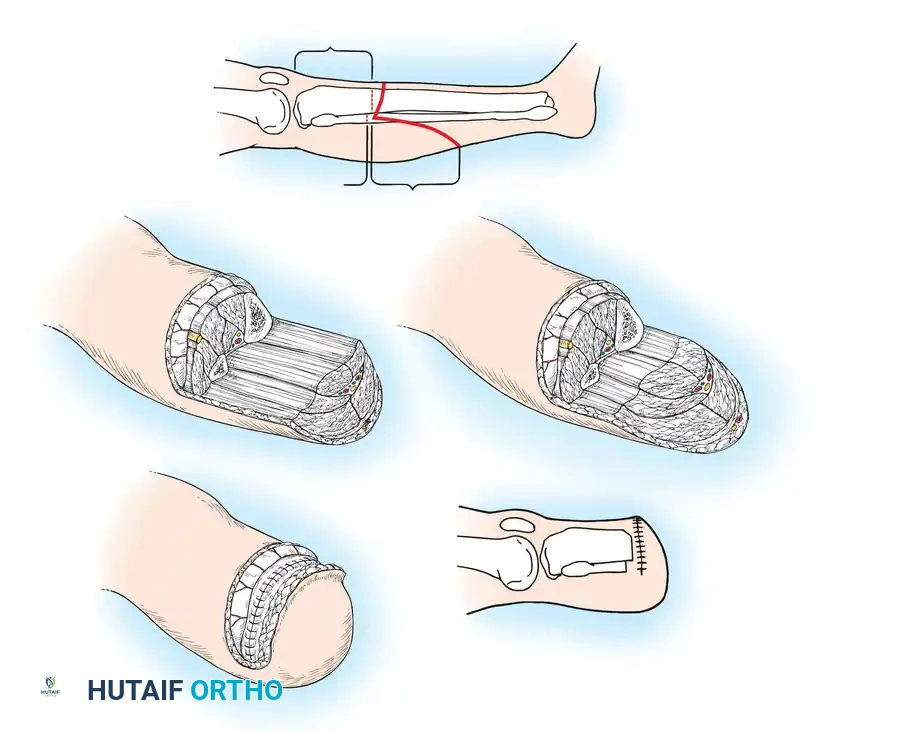
🔪 Surgical Technique 11-2: Long Posterior Flap (Burgess Technique for Ischemic Limbs)
Positioning and Preparation:
* Position the patient supine on the operating table. Do not apply a tourniquet.
* Prepare and drape the limb extensively so that an above-knee (transfemoral) amputation can be seamlessly performed if intraoperative assessment reveals insufficient bleeding and tissue viability to support a transtibial amputation.
* For ischemic limbs, the recommended level of tibial resection is 8.8 to 12.5 cm distal to the knee joint line.
Incision and Flap Design:
* Outline a long posterior flap and a very short (or absent) anterior flap. The length of the posterior flap should measure 1 cm more than the anteroposterior diameter of the leg at the level of bone division to ensure tension-free coverage.
* Fashion the anterior transverse incision at or slightly distal to the anticipated level of tibial section.
Anterior Dissection and Bone Resection:
* Reflect the anterior flap as a single, full-thickness layer (skin, deep fascia, and periosteum) over the anteromedial surface of the tibia.
* Divide the anterolateral muscles directly down to the intermuscular septum. Ligate and divide the anterior tibial vessels and deep peroneal nerve as they are encountered.
* Section the tibia transversely with a saw.
* Section the fibula at a level 0.9 to 1.3 cm higher (more proximal) than the tibial cut.
* Carefully round the distal tibia with a rasp and form a short, smooth bevel on its anterior and medial aspects to prevent pressure necrosis of the overlying ischemic skin.
Posterior Dissection and Flap Creation:
* Dissect the soft tissues from the posterior aspect of the tibia and fibula distally to the level of the posterior transverse skin division.
* Separate and remove the amputated distal leg, carefully ligating and dividing the posterior tibial vessels, peroneal vessels, and the tibial nerve.
* Bevel and tailor the posterior muscle mass (gastrocnemius and soleus) to thin the distal aspect of the flap, reducing unnecessary bulk while preserving the critical myocutaneous perforators.
Closure:
* Carry the long posterior myocutaneous flap anteriorly over the beveled bone ends.
* Suture the deep fascia of the posterior flap directly to the deep fascia and periosteum of the anterior flap. Do not perform tension myodesis.
* Obtain meticulous hemostasis. In ischemic limbs, postoperative hematoma formation is catastrophic and invariably leads to wound dehiscence and infection.
* Place a plastic closed-suction drainage tube deep to the muscle flap and fascia, bringing it out laterally through the skin 10 to 12.5 cm proximal to the end of the stump. (A through-and-through Penrose drain may be used if preferred, though it is more difficult to manage postoperatively).
* Close the skin edges with interrupted, non-strangulating nonabsorbable sutures (e.g., nylon) or surgical staples, ensuring absolutely no tension on the skin edges.
POSTOPERATIVE MANAGEMENT AND REHABILITATION
The postoperative protocol is dictated by the patient's vascular status, cognitive function, and overall physiological reserve.
Nonischemic Limbs
Rehabilitation after transtibial amputation in a nonischemic limb is generally aggressive. Unless the patient is immunocompromised, requires complex skin grafting, or possesses concomitant polytrauma precluding early mobilization, early prosthetic fitting is the standard of care.
* Immediate Postoperative Prosthesis (IPOP) / Rigid Dressing: Application of an immediate postoperative rigid cast dressing is highly recommended. It effectively controls stump edema, prevents knee flexion contractures (a devastating complication that precludes prosthetic use), and protects the vulnerable surgical site from external trauma.
* Early Mobilization: A prosthetist can apply a pylon jig to the rigid cast, allowing for early, touch-down weight bearing. Initial ambulation is strictly supervised, utilizing bilateral upper extremity support (parallel bars or a walker).
* Progression: The rigid cast is typically changed every 5 to 7 days to inspect the wound. Within 3 to 4 weeks, assuming primary wound healing, the patient is transitioned to a removable temporary prosthesis. The patient is instructed in the rigorous use of elastic figure-of-eight wrapping or a compressive stump shrinker to continuously contour the residual limb.
Ischemic Limbs
In patients with peripheral vascular disease, the primary goal is absolute wound protection.
* Dressing Strategy: While rigid dressings can be used, they must be applied with extreme caution by experienced personnel to avoid pressure necrosis over bony prominences. Often, soft compressive dressings or removable rigid dressings (RRDs) are preferred to allow frequent wound inspection.
* Delayed Fitting: Weight-bearing and prosthetic fitting are significantly delayed compared to nonischemic patients. The wound must be completely healed, and the sutures removed (often left in place for 3 to 4 weeks due to delayed healing in ischemic tissue) before any prosthetic casting occurs.
* Contracture Prevention: Positioning in bed is critical. The knee must be kept in full extension. Pillows under the knee are strictly prohibited, as they rapidly induce severe flexion contractures.
Long-Term Prosthetic Transition
The transition from a temporary to a definitive permanent prosthesis may take several months as the residual limb undergoes physiological atrophy and volume stabilization. Endoskeletal prosthetic designs are currently favored due to their modularity, allowing the prosthetist to make simple alignment and component modifications as the patient's gait mechanics evolve. Formal inpatient rehabilitation is usually brief, with the majority of intensive gait training and prosthetic optimization conducted in the outpatient setting under the guidance of a multidisciplinary team comprising physiatrists, physical therapists, and prosthetists.
📚 Medical References
- Transtibial amputation: surgical procedures and immediate postsurgical management. In Bowker JH, Michael JW, eds: Atlas of limb prosthetics: surgical, prosthetic, and rehabilitation principles, 2nd ed, St Louis, 1992, Mosby. Bowker JH, Keagy RD, Poonekar PD: Musculoskeletal complications in amputees: their prevention and management. In Bowker JH, Michael JW, eds: Atlas of limb prosthetics: surgical, prosthetic, and rehabilitation principles, 2nd ed, St Louis, 1992, Mosby. Burgess EM, Matsen FA: Current concepts review: determining amputation levels in peripheral vascular disease, J Bone Joint Surg 63A:1493, 1981.
- Burgess EM, Matsen FA, Wyss CR, et al: Segmental transcutaneous measurement of Po 2 in patients requiring below-the-knee amputation for peripheral vascular insuffi ciency, J Bone Joint Surg 64A:378, 1982.
- Cauchy E, Marsigny B, Allamel G, et al: The value of technetium 99 scintigraphy in the prognosis of amputation in severe frostbite injuries of the extremities: a retrospective study of 92 severe frostbite injuries, J Hand Surg 25A:969, 2000.
- Chapman MW, Olson SA:
