INTRODUCTION TO CHRONIC NONINSERTIONAL ACHILLES TENDINOSIS
Chronic noninsertional Achilles tendinosis is a debilitating degenerative condition characterized by angiofibroblastic hyperplasia, mucoid degeneration, and a disorganized collagen matrix, typically occurring 2 to 6 centimeters proximal to the calcaneal insertion. This region corresponds to the vascular watershed area of the tendon. When conservative measures—such as eccentric loading protocols, extracorporeal shockwave therapy, and immobilization—fail, surgical intervention becomes necessary.
For mild to moderate degeneration, simple debridement and tubularization may suffice. However, when aggressive debridement leaves a defect comprising more than 50% of the tendon's cross-sectional area, the remaining tissue is biomechanically insufficient to withstand the forces of normal ambulation. In these advanced cases, augmentation with a tendon transfer is strictly indicated.
The Flexor Hallucis Longus (FHL) is the gold standard for Achilles augmentation. It is preferred over the flexor digitorum longus (FDL) or peroneus brevis due to its superior cross-sectional area, in-phase firing pattern during the gait cycle, and the highly vascularized low-lying muscle belly, which provides crucial blood supply to the avascular degenerative zone of the Achilles.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the posterior ankle and plantar midfoot anatomy is essential for safe FHL harvest and transfer.
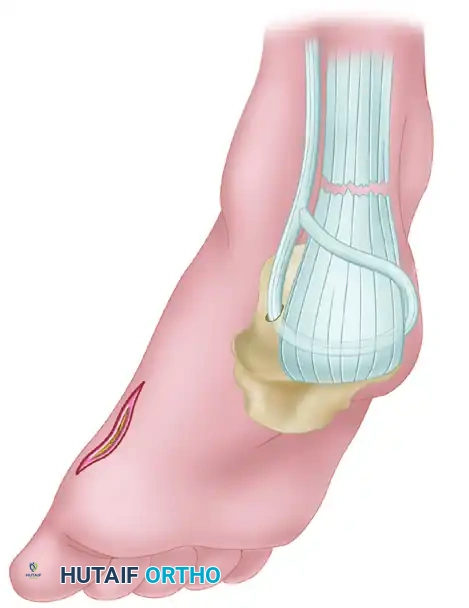
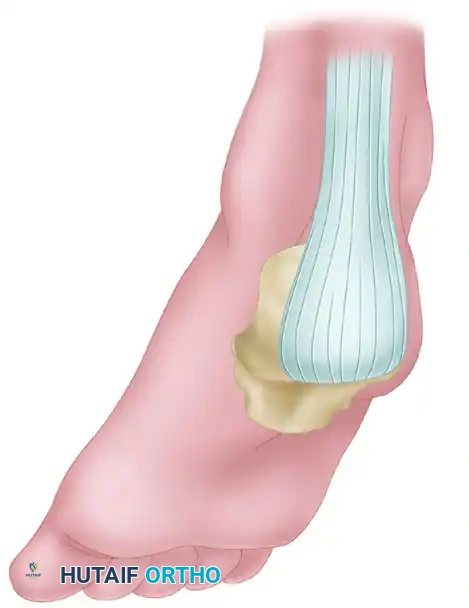
- FHL Muscle and Tendon: The FHL originates from the posterior surface of the fibula and the interosseous membrane. Its muscle belly extends distally, often as far as the tibiotalar joint, providing a robust vascular bed.
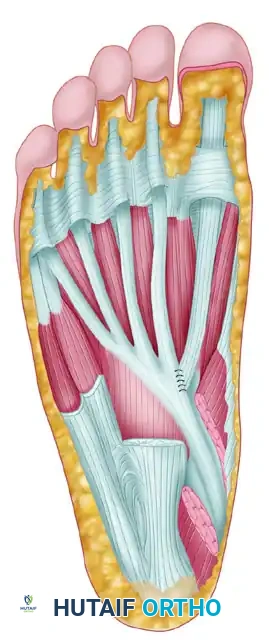
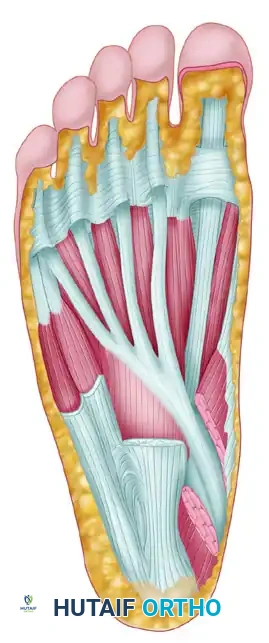
- The Master Knot of Henry: Located in the plantar midfoot, this is the anatomical decussation where the FHL tendon crosses dorsal to the FDL tendon.
- Neurovascular Proximity: The medial plantar nerve and artery lie immediately deep and lateral to the FHL tendon at the level of the Master Knot of Henry. Iatrogenic injury here can lead to devastating plantar numbness and vascular compromise.
- Biomechanics: The FHL is the second strongest plantarflexor of the ankle (after the triceps surae). Its axis of pull closely mimics that of the Achilles, making it the ideal synergistic transfer.
Clinical Pearl: The low-lying muscle belly of the FHL is not merely a structural augment; it acts as a vascularized pedicle graft. Suturing this muscle belly directly into the debrided Achilles defect significantly enhances local angiogenesis and healing.
INDICATIONS AND PREOPERATIVE PLANNING
Indications for FHL Transfer
- Chronic noninsertional Achilles tendinosis with >50% tendon degeneration.
- Failed conservative management exceeding 6 months.
- Revision Achilles tendon surgery.
- Chronic Achilles tendon ruptures with a gap >3 cm that cannot be opposed with maximal equinus.
Preoperative Evaluation
- Clinical Examination: Assess resting tension, palpable gaps, and perform the Thompson test. Evaluate hallux plantarflexion strength to establish a baseline.
- Imaging: Weight-bearing radiographs rule out Haglund's deformity or insertional calcific tendinosis. Magnetic Resonance Imaging (MRI) is mandatory to quantify the extent of tendinosis, measure the gap in chronic ruptures, and assess the quality of the FHL muscle belly (ruling out fatty infiltration).
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Patient Positioning and Anesthesia
- Administer a satisfactory general anesthetic or regional neuraxial block.
- Place the patient in the prone position on the operating table. Ensure all bony prominences are meticulously padded.
- Apply a high thigh tourniquet to provide a bloodless surgical field.
- Prep and drape the entire lower extremity from the toes to the proximal thigh to allow intraoperative assessment of resting equinus tension.
2. Incision and Achilles Exposure
- Make a longitudinal incision just medial to the Achilles tendon, approximately 10 cm in length, centered over the nodular, diseased section of the tendon. A medial approach avoids the sural nerve, which courses laterally.
- Carefully incise the paratenon. Preserve this tissue meticulously, as it will be required for closure to prevent skin tethering.
- Remove any inflammatory peritendinitis or adhesions with a rongeur.
- Retract the medial border of the tendon posteriorly using a double skin hook retractor to gain access to the deep, involved portion of the tendon.
3. Achilles Debridement
- Sharply debride the area of degeneration until healthy, normal-appearing tendon is reached. Healthy tendon will appear pearly white with parallel collagen fibers, whereas tendinotic tissue is dull, yellowish, and disorganized.
- The 50% Rule: If less than 50% of the tendon is involved, close the defect with interrupted 2-0 braided, nonabsorbable sutures. Do not excessively strip the vascular supply of the mesotenon on the deep surface of the Achilles.
- If substantially more than 50% of the tendon is excised, proceed with the FHL transfer.
4. FHL Identification and Midfoot Harvest
- Make a longitudinal incision just deep to the Achilles tendon in the posterior compartment. Cauterize the numerous small veins present in this area.
- Develop the interval between the FHL and the peroneal tendons.
- Surgical Warning: Take extreme care to avoid the posterior tibial neurovascular bundle by staying strictly at or lateral to the FHL tendon during deep dissection.
- Once the FHL is identified posteriorly, transition to the medial foot to maximize graft length. Make a longitudinal incision over the medial aspect of the dorsal arch of the abductor hallucis muscle.
- Deepen the incision with plantar retraction of the abductor hallucis muscle to expose the plantar fascia and deep structures.
- Identify the Master Knot of Henry proximally.
- Surgical Warning: The medial plantar nerve and artery generally lie just deep and lateral to the FHL tendon. Meticulous blunt dissection is required here.
- Dissect distally to allow sufficient harvest of the tendon. The length required depends on the Achilles defect. If the entire insertion of the Achilles tendon is compromised, a maximum-length tendon graft is necessary.
5. Tenodesis of FHL to FDL
- To prevent postoperative hallux malleus and loss of great toe push-off strength, the distal stump of the FHL must be secured.
- With the toes held in plantarflexion, suture the distal stump of the FHL tendon to the adjacent FDL tendon using interrupted 2-0 Vicryl (polyglactin 910) sutures.
6. Tendon Delivery and Transfer
- Harvest the FHL tendon by transecting it proximal to the tenodesis site.
- Release all fascial connections and slips between the FHL and the FDL.
- Deliver the FHL tendon proximally into the posterior calf incision.
- For Noninsertional Achilles Tendinosis: Sew the FHL muscle belly and tendon directly into the defect created by the debridement. The muscle belly provides a rich vascular supply to the healing tendon, while the tendon itself acts as a biomechanical bridge.
7. Calcaneal Fixation (For Insertional Variants or Complete Ruptures)
- If complete debridement of the Achilles insertion was required, the FHL must be anchored directly into the calcaneus.
- Use successively larger drill bits to create a transverse or dorsal-to-plantar bone tunnel in the calcaneal tuberosity. Generally, a 3/8-inch tunnel is satisfactory to allow smooth passage of the tendon.
- Weave the FHL tendon through the remaining Achilles tendon stump using a Pulvertaft weave technique to maximize surface area contact.
- Pass the FHL tendon through the calcaneal bone tunnel.
- Tensioning: Tension the graft with the ankle in moderate equinus (approximately 15 to 20 degrees of plantarflexion). Ensure that the ankle can be brought to neutral after final suturing. Proper tensioning is critical to restore sufficient push-off power postoperatively.
- Suture the tendon onto itself with interrupted No. 2 Ethibond or equivalent heavy nonabsorbable sutures.
- Alternative Fixation: An interference-type absorbable biocomposite screw can be utilized within a dorsal-to-plantar bone tunnel to secure the FHL tendon directly into the calcaneus, providing excellent biomechanical pull-out strength.
8. Closure
- Thoroughly irrigate the wound.
- Close the paratenon meticulously over the repair with interrupted 2-0 absorbable sutures. This layer is vital to prevent the skin from adhering to the underlying tendon transfer.
- Close the subcutaneous tissue and skin in a routine, layered fashion. Apply a sterile, non-adherent dressing.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative protocol must balance the protection of the tendon transfer with the prevention of arthrofibrosis and muscle atrophy.
Phase 1: Maximum Protection (Weeks 0 to 4)
- Immobilization: The patient is placed in a strict non-weight-bearing (NWB) short leg cast or rigid splint with the ankle in slight equinus (15-20 degrees) to remove tension from the repair.
- Edema Control: Strict elevation of the operative limb above the level of the heart is required for the first 7-10 days to mitigate swelling and optimize wound healing.
- Wound Check: At 2 weeks, the cast is bi-valved, sutures are removed, and the patient is placed back into a NWB cast or rigid boot in equinus.
Phase 2: Progressive Weight-Bearing (Weeks 4 to 8)
- Immobilization: At 4 weeks, transition the patient to a prefabricated controlled ankle motion (CAM) walking brace.
- Heel Lifts: Insert multiple heel lifts (approximately 2.5 to 3 inches in total height) into the boot to maintain the equinus position.
- Weight-Bearing: Initiate progressive partial weight-bearing.
- Wedge Removal: Remove one wedge of the heel lift each week as the patient gradually increases weight-bearing on the foot. By week 8, the ankle should be in a neutral position within the walking boot.
Phase 3: Range of Motion and Strengthening (Weeks 8 to 14)
- Physical Therapy: At 8 weeks, formal physical therapy commences.
- Range of Motion: Begin active and active-assisted range-of-motion exercises. Gentle calf stretching is initiated, avoiding aggressive passive dorsiflexion.
- Strengthening: Introduce isometric plantarflexion exercises, progressing to concentric and eventually eccentric loading as tolerated.
- Footwear: Transition from the CAM boot to a supportive athletic shoe with a small silicone heel cup.
Phase 4: Return to Activity (3.5 Months and Beyond)
- Gradual return to low-impact activities (cycling, swimming) is permitted around 3.5 months.
- High-impact activities, running, and sports involving explosive push-off are delayed until 5 to 6 months postoperatively, contingent upon the recovery of at least 80% of contralateral plantarflexion strength and complete resolution of pain.
COMPLICATIONS AND PITFALLS
While highly successful, the FHL transfer carries specific risks that the orthopedic surgeon must anticipate:
- Sural Nerve Injury: Can occur during the posterior incision if dissection drifts laterally. Always maintain a medial bias.
- Medial Plantar Nerve Injury: The highest risk occurs during the harvest at the Master Knot of Henry. Meticulous blunt dissection is mandatory.
- Hallux Malleus: Failure to adequately tenodese the distal FHL stump to the FDL can result in a clawed great toe and subjective weakness during the toe-off phase of gait.
- Wound Dehiscence: The posterior ankle has tenuous vascularity. Excessive retraction, failure to close the paratenon, or premature mobilization can lead to skin necrosis and deep infection.
- Over-lengthening / Weakness: Securing the transfer with the ankle in excessive dorsiflexion will result in a lengthened Achilles-FHL complex, leading to a permanent calcaneus gait and profound push-off weakness. Always tension in moderate equinus.
