INTRODUCTION TO NEUROVASCULAR FREE TISSUE TRANSFER
The neurovascular supply to the web space between the great and second toes renders this anatomical region exceptionally suitable for free tissue transfer. Specifically, it is the gold standard for restoring sensibility and durable soft tissue coverage to the hand, with particular emphasis on thumb reconstruction. Following the pioneering anatomical studies and the first successful clinical application by Gilbert et al. in 1975, the first web space, pulp, and hemipulp neurovascular free flaps have become indispensable techniques in the armamentarium of the reconstructive microsurgeon.
The primary objective of these flaps is not merely wound closure, but the restoration of tactile gnosis, pinch biomechanics, and aesthetic contour. The unique properties of the foot's plantar skin closely mirror those of the palmar hand, making this donor site unparalleled for digital resurfacing.
Advantages of the First Web and Pulp Donor Area
- Superior Functional Sensibility: The first web space possesses an excellent potential for sensory recovery. The two-point discrimination (2-PD) on the native toe pulps ranges from 10 to 18 mm, which can be reliably transferred and re-educated in the recipient bed.
- Optimal Tissue Match: The pulp skin is glabrous, highly specialized, and closely approximates the biomechanical and histological properties of digital palmar skin.
- Robust Vascularity: The first web space boasts a highly reliable and predictable blood supply, primarily driven by the first dorsal metatarsal artery (FDMA).
- Versatile Surface Area: The relatively large area available permits comprehensive resurfacing of the thumb, especially when utilized as a "wraparound" flap.
- Composite Potential: If larger surface areas are required, the flap can be seamlessly extended to incorporate a dorsalis pedis flap in continuity with the first web space.
- Acceptable Donor Morbidity: When meticulously harvested and successfully covered with a split-thickness skin graft (STSG), donor site morbidity is minimized, allowing for normal ambulation.
Disadvantages and Limitations
Despite its profound advantages, the procedure carries inherent challenges:
* Resource Intensive: The complexity of the procedure typically necessitates a two-team approach to minimize ischemic time and operative duration.
* Microsurgical Risks: As with all free tissue transfers, there is a baseline risk of vascular thrombosis, which can lead to catastrophic loss of the entire flap.
* Donor Site Complications: Delayed healing, skin graft failure, or hypertrophic scarring at the donor site can be troublesome and prolong rehabilitation.
* Sensory Disturbances: Some patients report limited usefulness due to residual pain, hypersensitivity, or cold intolerance at either the donor or recipient sites.
Clinical Pearl: Patient selection is paramount. Avoid this flap in patients with severe peripheral vascular disease, uncontrolled diabetes mellitus, or a history of significant trauma to the donor foot, as these conditions exponentially increase the risk of both flap failure and donor site morbidity.
SURGICAL ANATOMY
A profound understanding of the vascular and neural anatomy of the foot is the cornerstone of successful flap elevation. The anatomy of the first web space is characterized by significant variability, demanding meticulous preoperative planning and intraoperative adaptability.
Venous Drainage
The venous drainage of the foot and the first web space relies on a dual system: the superficial and deep venous networks. The superficial system is predominantly utilized for venous outflow in free flap surgery due to its accessibility and larger caliber.

FIGURE 63-52: Venous drainage of the foot. Tributaries to the greater and lesser saphenous venous systems are utilized to drain the dorsalis pedis and toe free flaps.
The dorsal venous arch collects blood from the dorsal digital veins. The medial aspect of this arch drains into the greater saphenous vein, while the lateral aspect drains into the lesser saphenous vein. When elevating the first web space flap, the dorsal veins accompanying the first metatarsal space must be carefully preserved and traced proximally to ensure adequate venous outflow.
Cutaneous Innervation
Sensory restoration is achieved by coapting the nerves of the flap to the recipient digital nerves. The innervation of the adjacent sides of the great and second toes is supplied by a triad of nerve systems.




FIGURE 63-53: Cutaneous innervation of the foot. (A) Dorsal sensory supply of the foot and toes. (B) Plantar sensory supply of the foot and toes. Note the distributions of the sural nerve, deep peroneal nerve, superficial peroneal nerve, and the medial/lateral plantar nerves.
- Plantar Digital Nerves (Primary): The most critical innervation to the lateral side of the great toe pulp and the medial side of the second toe pulp is delivered via the plantar digital branches of the common digital nerve to the first web space (derived from the medial plantar nerve). These proper digital branches are typically 1 to 1.5 mm in diameter. They can be dissected proximally and separated via intraneural dissection into the common digital nerve to yield sufficient length for tension-free neurorrhaphy at the recipient site.
- Deep Peroneal Nerve (Secondary): Two terminal branches of the deep peroneal nerve enter the web space dorsally, supplying the dorsal surfaces of the adjacent sides of the great and second toes. These branches can be harvested with the flap to provide supplementary dorsal innervation.
- Superficial Peroneal Nerve: The terminal branches of this nerve are extremely diminutive and terminate too far proximally on the dorsum to effectively innervate the first web or pulp flaps; thus, they are generally not utilized for this specific transfer.
Arterial Supply and Variations
The arterial anatomy of the first web space is complex and highly variable. The primary supply is the First Dorsal Metatarsal Artery (FDMA), which arises from the dorsalis pedis artery just before it dives plantarly as the deep plantar artery.
May et al. conducted extensive anatomical studies demonstrating that the distal communicating artery (DCA)—the terminal continuation of the FDMA—exhibits three distinct patterns of communication with the plantar digital arterial system.
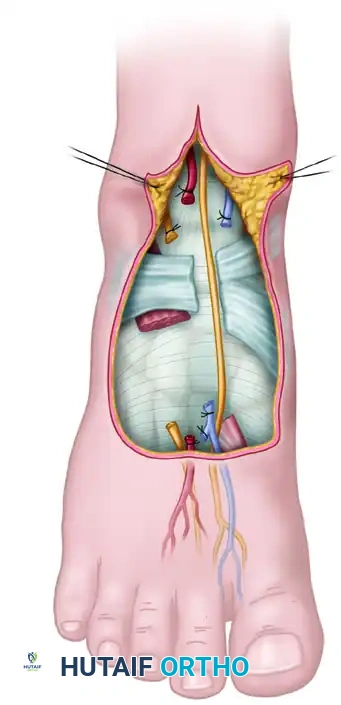
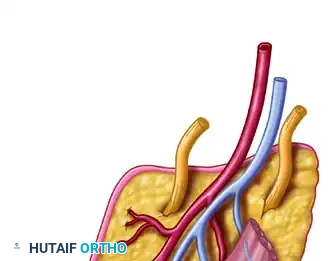
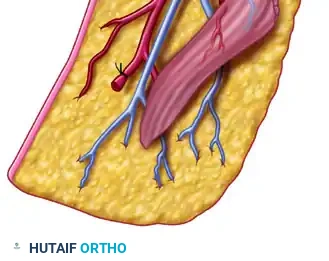
FIGURE 63-55: Variations in circulation to the first web space. Three patterns of communication between the distal communicating artery (DCA) and the plantar digital arterial system have been identified. DDA, dorsal digital artery; FDMA, first dorsal metatarsal artery; FPMA, first plantar metatarsal artery; PDA, plantar digital artery; TML, transverse metatarsal ligament.
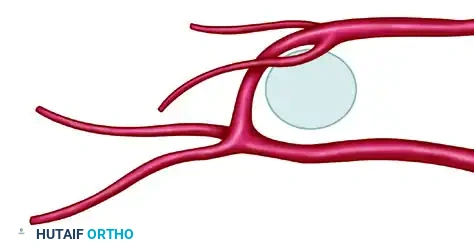
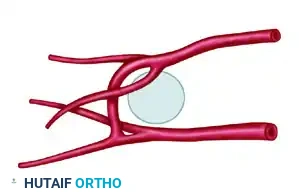
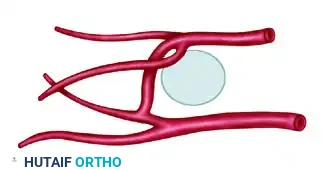
Detailed views of the arterial variations (DDA 1, DDA 2, PDA 1, PDA 2, TML, DCA, FDMA, FPMA).
The three identified patterns of the DCA are:
1. Pattern 1 (28%): The DCA joins at the bifurcation of the first plantar metatarsal artery (FPMA).
2. Pattern 2 (26%): The DCA joins with the first plantar digital artery (supplying the great toe).
3. Pattern 3 (38%): The DCA joins with the second plantar digital artery (supplying the second toe).
Furthermore, the dorsal portion of the first web is supplied by the first and second dorsal digital arterial branches of the FDMA.
Surgical Warning: These anatomical variations dictate that dissection must proceed with extreme caution. If the FDMA is found to be hypoplastic or absent (a Type III pattern according to Gilbert's classification), the surgeon must be prepared to trace and utilize the First Plantar Metatarsal Artery (FPMA) as the dominant pedicle.
PREOPERATIVE PREPARATION
Thorough preoperative evaluation is non-negotiable.
* Vascular Assessment: The arterial supply to the foot must be assessed preoperatively using a handheld Doppler probe. In cases of ambiguity or previous trauma, formal angiography (CT angiography or conventional arteriography in two planes) is mandatory to confirm the patency and dominance of the FDMA versus the FPMA.
* Templating: The recipient defect on the hand is meticulously measured. A template (often using Esmarch bandage or sterile foil) is created to represent the exact dimensions of the required skin paddle.
* Patient Counseling: The patient must be fully informed regarding the expected donor site morbidity, the necessity of skin grafting, and the prolonged rehabilitation required for sensory re-education.
SURGICAL TECHNIQUE: FIRST WEB SPACE AND PULP FLAP
The procedure is ideally performed using a two-team approach. Team A prepares the recipient site in the hand, isolating the recipient artery (e.g., radial artery branches or princeps pollicis), veins (cephalic vein tributaries), and nerves (proper digital nerves). Team B simultaneously harvests the flap from the foot.
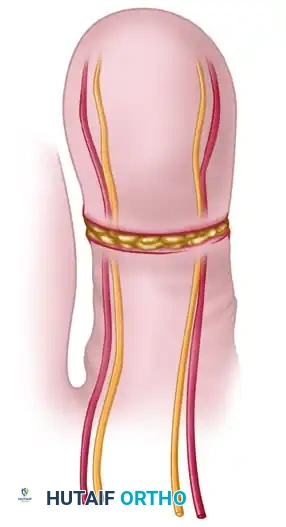
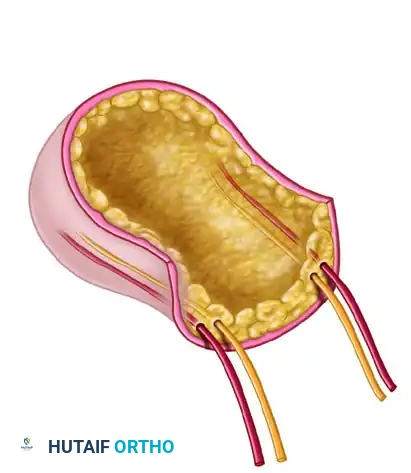
FIGURE 63-56: Scheme for pulp free flap. (A) Flap outlined and toe dissection begun for the skin flap. (B) Flap separated from the toe, isolating the digital arteries, venae comitantes, and nerves.
🔪 Operative Steps (Technique 63-31)
1. Marking and Exsanguination
* On the skin of the dorsum of the foot, mark the course of the dorsalis pedis artery and the FDMA as determined by palpation and Doppler mapping.
* Identify the venous pattern by allowing the foot to hang dependently over the edge of the operating table until the veins engorge. Mark the course of the dominant superficial veins draining the first web space.
* Determine the exact amount of skin required by measuring the recipient area on the thumb or finger. Flaps measuring from 6 × 10 cm up to 8 × 12 cm can be safely harvested from the first web. If a massive defect exists, plan to incorporate the dorsalis pedis skin flap in continuity with the first web skin.
* Outline the flap in the first web space with a surgical marker, ensuring the margins correspond to the templated defect.
* Exsanguinate the limb by wrapping it with an Esmarch bandage, and inflate the pneumatic thigh tourniquet to the appropriate pressure (typically 250-300 mmHg).
2. Dorsal Dissection and Pedicle Isolation
* Begin the dissection over the arterial pedicle with a curved or zigzag incision on the dorsum of the foot, coursing between the first and second metatarsals.
* Elevate the skin flaps carefully to preserve the marked superficial venous system. Isolate a robust superficial vein to serve as the primary venous drainage for the flap.
* With meticulous microsurgical dissection, identify the dorsalis pedis artery. Follow it distally to the point where it gives off the deep plantar branch.
* Ligate and divide the deep plantar branch to mobilize the pedicle, then follow the First Dorsal Metatarsal Artery (FDMA) distally into the first web space.
* To facilitate exposure of the artery, elevate and divide the extensor hallucis brevis (EHB) tendon.
* Identify and include the deep peroneal nerve alongside the arterial pedicle, as it provides dorsal sensibility to the flap.
3. Plantar Dissection and Nerve Isolation
* Extend the incisions plantarly to outline the pulp or hemipulp components of the flap.
* Identify the common digital nerve to the first web space. Perform an intraneural dissection to separate the proper digital branches supplying the lateral aspect of the great toe and the medial aspect of the second toe.
* Trace these nerves proximally to obtain sufficient length for the recipient site neurorrhaphy.
* Identify the plantar digital arteries. Depending on the anatomical variation (as described by May et al.), ligate the branches supplying the non-harvested tissues while meticulously preserving the distal communicating artery (DCA) and its connections to the flap.
4. Flap Elevation and Ischemia Time
* Elevate the flap from distal to proximal, ensuring the plantar digital nerves, the FDMA (or FPMA if dominant), and the venous outflow tract remain in continuity with the skin paddle.
* Once the flap is completely isolated on its neurovascular pedicle, deflate the tourniquet.
* Observe the flap for robust perfusion. The edges should bleed, and the capillary refill should be brisk (1-2 seconds). Allow the foot to perfuse for at least 20-30 minutes before pedicle division.
* Communicate with the hand team to ensure the recipient vessels are fully prepared. Once confirmed, ligate the pedicle proximally and transfer the flap to the hand. Record the exact ischemia time.
5. Donor Site Management
* Meticulous hemostasis of the foot is achieved using bipolar electrocautery.
* The donor defect in the first web space cannot be closed primarily. It requires resurfacing with a thick split-thickness skin graft (STSG) or a full-thickness skin graft (FTSG) harvested from the groin or thigh.
* Secure the graft with a tie-over bolster dressing to prevent shearing forces and hematoma formation.
* Apply a well-padded short leg splint, maintaining the ankle in neutral dorsiflexion and protecting the toes from pressure.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of a neurovascular free flap extends far beyond the operating room. Strict adherence to postoperative microsurgical protocols is critical.
Flap Monitoring
- Clinical Assessment: The flap must be monitored every hour for the first 24-48 hours, then every 2-4 hours for the next 3 days. Assess color, capillary refill, tissue turgor, and temperature.
- Instrumental Monitoring: Surface Doppler probes or implantable venous Doppler systems are highly recommended to continuously monitor arterial inflow and venous outflow.
- Environment: The patient's room should be kept warm to prevent vasospasm. The patient must be strictly hydrated, and all forms of nicotine or caffeine are absolutely contraindicated.
Anticoagulation
- Protocols vary by institution, but a common regimen includes intravenous Dextran 40 or subcutaneous Heparin for 5 days postoperatively, followed by daily oral aspirin (81 mg or 325 mg) for 4 to 6 weeks.
Donor Site Care
- The foot is kept elevated for 10 to 14 days to minimize edema and optimize skin graft take.
- Strict non-weight-bearing status is enforced for 2 to 3 weeks.
- Once the skin graft is fully incorporated, progressive weight-bearing in a stiff-soled postoperative shoe is initiated.
Sensory Re-education
- Once the recipient site wounds have healed and the nerve coaptations begin to regenerate (typically advancing 1 mm per day), a formal sensory re-education program is initiated under the guidance of a specialized hand therapist.
- This involves progressive tactile stimulation, moving from perception of constant touch to moving touch, and eventually to fine two-point discrimination exercises.
COMPLICATIONS AND PITFALLS
- Vascular Thrombosis: The most dreaded complication. Venous congestion usually presents within the first 24 hours (bluish discoloration, brisk capillary refill, dark bleeding). Arterial insufficiency presents as a pale, cool flap with absent capillary refill. Immediate return to the operating theater for pedicle exploration and thrombectomy is mandatory.
- Donor Site Morbidity: Failure of the skin graft on the foot can lead to prolonged healing, infection, and debilitating scar contracture in the web space. Meticulous graft securing and strict elevation are preventative.
- Cold Intolerance: A frequent long-term complaint in both the reconstructed digit and the donor toe. Patients must be counseled to protect the extremities in cold weather.
- Neuroma Formation: Improper handling or excessive tension on the nerve coaptations can lead to painful neuromas, severely limiting the functional outcome of the reconstruction.
