DEFINITION
Multiple techniques have been described for the release of elbow contractures. The medial approach has the advantages of direct access to both the anterior and posterior aspects of the ulnohumeral joint and direct visualization of the ulnar nerve. Medial-based releases were initially proposed by Wilner,24 whose technique involved medial epicondylectomy and wide dissection.Weiss and Sachar23 subsequently has described splitting the flexor-pronator mass rather than complete release of the flexor-pronator mass.Mansat et al12 popularized this approach to deal with extrinsic contracture of the elbow and ulnar nerve involvement.Itoh et al10 and Wada et al22 underlined the importance of the posterior oblique band of the medial collateral ligament as a critical structure to identify and release if an extension contracture exists.
ANATOMY
The medial compartment of the elbow includes the medial side of the ulnohumeral joint, the medial collateral ligament, the flexor-pronator mass, the ulnar nerve, and the medial antebrachial cutaneous nerve (FIG 1A).The medial ulnohumeral joint is composed of the medial column, the medial epicondyle, the medial side of the proximal aspect of the ulna, and the coronoid process.The medial collateral ligament consists of three parts: anterior, posterior, and transverse segments (FIG 1B).The anterior bundle is the most discrete component, the posterior portion being a thickening of the posterior capsule, and is well defined only in about 90 degrees of flexion.The transverse component appears to contribute little or nothing to elbow stability.The medial collateral ligament originates from a broad anteroinferior surface of the epicondyle but not fromthe condylar elements of the trochlea just inferior to the axis of rotation.18 The ulnar nerve rests on the posterior aspect of the medial epicondyle, but it is not intimately related to the fibers of the anterior bundle of the medial collateral ligament itself.The flexor-pronator mass includes the pronator teres, the most proximal of the flexor-pronator group; the flexor carpi radialis, which originates just inferior to the origin of the pronator teres at the anteroinferior aspect of the medial epicondyle; the palmaris longus muscle, which arises from the medial epicondyle and from the septa it shares with the flexor carpi radialis and flexor carpi ulnaris; the flexor carpi ulnaris, which is the most posterior of the common flexor tendons originating from the medial epicondyle and from the medial border of thecoronoid and the proximal medial aspect of the ulna; and the flexor digitorum superficialis, which is the deepest from the common flexor tendon but superficial to the flexor digitorum profundus.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Diagnosis of the contracture is usually made by identifying a characteristic history and performing a physical examination.Joint involvement is confirmed by plain radiographs. The anteroposterior (AP) view gives good visualization of the joint line, whereas the lateral view can demonstrate osteophytes on the coronoid and at the tip of the olecranon, even when the joint space is preserved.The details of the extent of any boney involvement are best observed on computed tomography. Transverse imaging by magnetic resonance imaging (MRI) has little use in our practice.
NONOPERATIVE MANAGEMENT
Several options have been proposed for the treatment of elbow contracture.Nonoperative treatment with mobilization of the elbow through the use of alternating flexion and extension splints17 or dynamic splints8 can provide a good result if it is initiated soon after the contracture develops. Manipulation with the patient under anesthesia have also been recommended, but loss of motion and ulnarnerve injury have been reported.6Recently, botulinum toxin has been used to release muscle contracture in order to facilitate elbow rehabilitation and regain motion.20Nonoperative treatment usually is successful only for extrinsic stiffness that has been present for 6 months or less, and the results can be unpredictable. With failure of nonoperative treatment, surgical release may be indicated. Recently, arthroscopic techniques for capsular release of the elbow have been described; however, open release remains a safe, reproducible option for regaining elbow motion.
SURGICAL MANAGEMENT
INDICATIONS
Contracture release Stiff elbowDegenerative arthritis with anterior and posteromedial osteophytes Ulnar nerve symptoms
ADVANTAGES
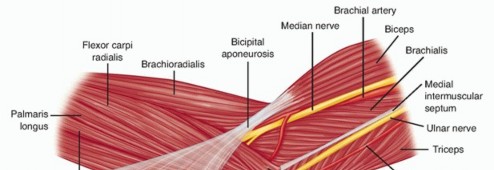
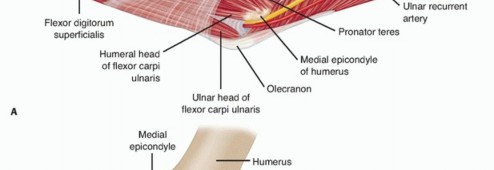
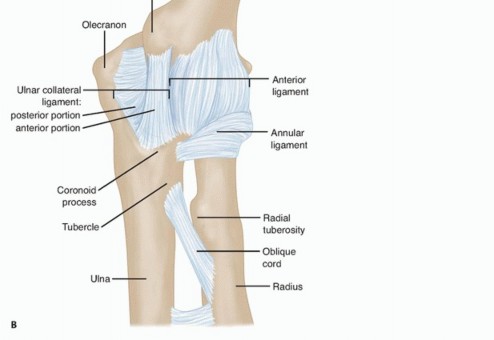
FIG 1 • Superficial (A) and deep (B) anatomy of the medial side of the elbow.
DISADVANTAGES
Difficulty in removing heterotopic bone on the lateral side of the joint Affords poor access to radial head
PREOPERATIVE PLANNING
Before surgery, the decision must be made to approach the capsule from the lateral or medial aspect.If the ulnar nerve is to be addressed or there is extensive medial or coronoid arthrosis, the medial approach is of value.If the radiohumeral joint is involved or if a simple release is all that is required, the lateral “column” procedure is carried out.
POSITIONING
The patient is usually positioned supine, supported by an elbow or a hand table.Two folded towels should be placed under the scapula. A sterile tourniquet is positioned.P.1191To expose the posterior joint, the patient's shoulder should have fairly free external rotation; otherwise, the arm should be positioned over the chest.
APPROACH
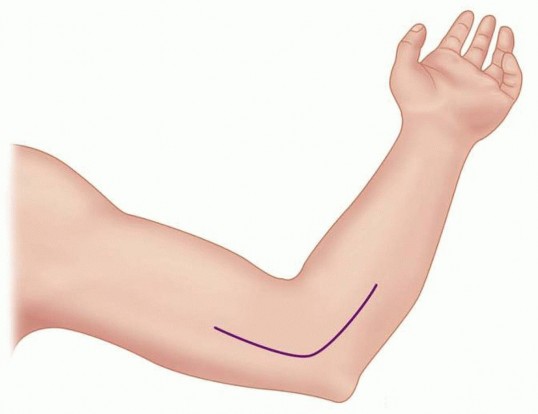
FIG 2 • SKIN INCISION.
TECHNIQUE
Exposing the Ulnar Nerve and the Medial Fascia


TECH FIG 1 • Exposure of the ulnar nerve and medial fascia.
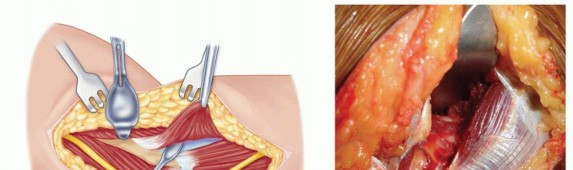
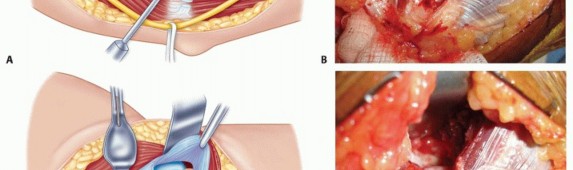
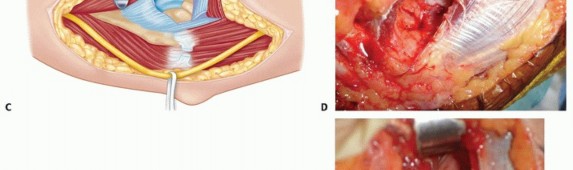
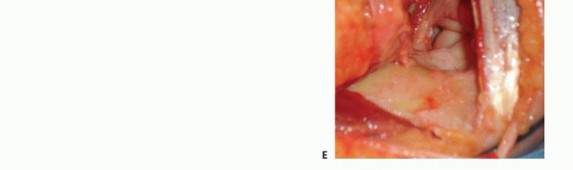
TECH FIG 2 • A,B. Exposure of the anterior capsule. C-E. After excision of the anterior capsule, visualization of the ulnohumeral joint down to the radiocapitellar joint.


TECH FIG 3 • A,B. Exposure of the posterior compartment. In contracture release, the posterior capsule and posterior band of the medial collateral ligament should be excised.The medial joint line up to the anterior band of the medial collateral ligament should also be exposed and the capsule excised. This area is the floor of the cubital tunnel.In contracture release and in primary osteoarthritis, the tip of the olecranon usually must be excised to achieve full extension.The posteromedial joint line is easily visualized, but the posterolateral side must also be carefully palptated to ensure clearance.3. Ulnar Nerve TranspositionP.1194The ulnar nerve should be transposed and secured with a fascial sling to prevent posterior subluxation.The sling can be fashioned by elevating two overlapping rectangular flaps of fascia or by using a medially based flap attached to the underlying subcutaneous tissue.Once this maneuver is completed, the nerve must not be compressed or kinked. The joint should be flexed and extended to ensure that the nerve is free to move.4. ClosureThe flexor-pronator mass should be reattached to the supracondylar ridge with nonabsorbable braided 1-0 or 0 suture.If a large enough cuff of tissue was left on the medial epicondyle, no holes need to be drilled in bone.Otherwise, drill holes in the edge of the supracondylar ridge can be made to secure the flexor-pronator mass (TECH FIG 4).
TECH FIG 4 • CLOSURE.


PEARLS AND PITFALLS
POSTOPERATIVE CARE
If the neurologic examination findings in the recovery room are normal, a brachial plexus block is established and maintained with a continuous pump through a percutaneous catheter.The arm is elevated as much as possible, and mechanical continuous passive motion exercise are begun the day of surgery and adjusted to provide as much motion as pain or the machine itself allows.After 2 days, the plexus block is discontinued, and at day 3, the continuous passive motion machine is stopped.Physical therapy is not used, but a detailed program of splint therapy is prescribed.Adjustable splints are prescribed, depending on the motion before and after the procedure. The splints include a hyperextension or a hyperflexion brace or both.A detailed discussion regarding heat, ice, and antiinflammatory medication, along with a visual schedule for bracing, is provided.During the first 3 months, the patient sleeps with the splint adjusted to maximize flexion or extension, whichever is more needed; it should not be so uncomfortable as to prevent sleeping for at least 6 hours.P.1195Because the principal objective is to gain motion but to avoid pain, swelling, and inflammation, routine use of an anti-inflammatory medication is prescribed.Therapy with splints is continued for about 3 months, during which time the patient is seen at 2- to 4-week intervals, if possible.After 4 weeks, an arc of about 80 degrees of motion is obtained, and the amount of time that each splint is worn is gradually decreased.Splinting at night is continued for as long as 6 months if flexion contracture tends to recur when the splint is not used.Patients are advised that it may take a year to realize full correction.
OUTCOMES
Recent reports on the results of surgical arthrolysis reveal an absolute gain in the flexion-extension arc between 30 and 60 degrees.1,3,4,5,7,9,10,11,14,15,16,19,21A functional arc of motion between 30 and 130 degrees is obtained in more than 50% of cases, and some improvement in motion in more than 90% of the cases has been reported in the literature.1,3,4,5,7,9,10,11,14,15,16,19,21In Europe, a combined lateral and medial approach has been used for many years, and gains in flexion arc have averaged between 40 and 72 degrees (in about 400 procedures).1,3,7,14 Some preferred a posterior extensile approach if medial and lateral exposures are anticipated.The importance of sequential release of tissues has been emphasized, based on an experience with44 of 46 patients (95%) who were satisfied with such an approach.13 The preoperative arc improved from 45 to 99 degrees.The authors emphasize the need to release the exostosis and the collateral ligament when contracted, especially noting the need to release the posterior portion of the medial collateralligament and decompress the ulnar nerve when ulnar nerve symptoms exist preoperatively.13 Using a medial approach, Wada et al22 obtained improvement of the mean arc of movement of 64degrees. A functional arc of flexion-extension (30 to 130 degrees) was obtained in 7 of the 14 elbows.None of the patients developed symptoms related to the ulnar nerve. According to those authors, the medial approach has several advantages over both the anterior and lateral approaches:Pathologic changes in the posterior oblique bundle of the medial collateral ligament can be observed and excised under direct vision.Anterior and posterior exposure is possible through one medial incision, through which a complete soft tissue release and excision of part of the olecranon and coronoid process can be undertaken if necessary. Additional lateral exposure is indicated only if the medial approach has proved to be inadequate.In the medial approach, the ulnar nerve is routinely released and protected under direct vision, which decreases the risk of damage.
COMPLICATIONS
A most important emerging consideration of the proper treatment of elbow stiffness is the vulnerability of the ulnar nerve.The most common cause of failure of treatment has been in patients whose preoperative ulnar nerve symptoms were not appreciated or addressed, or patients in whom ulnar nerve symptoms developed postoperatively without adequate treatment. This is attributable to traction neuritis caused by the abrupt increase in elbow flexion or extension during the operation.Even in the absence of preoperative neurologic symptoms, the nerve may be compromised subclinically and become symptomatic as elbow motion increases after surgery. Therefore, all patients who have stiff elbows must be evaluated for the presence or absence of ulnar nerve symptoms.Antuna et al2 recommended that elbows with preoperative flexion limited from 90 to 100 degrees in which we expect to improve the motion by 30 or 40 degrees should be treated with inspection and often prophylactic decompression or translocation of the nerve, depending on the appearance of the nerve once the surgical procedure is finished.Furthermore, all patients with preoperative ulnar nerve symptoms, even if they are mild, are treated with mobilization of the nerve.These authors stated that manipulation of the elbow in the early postoperative period must be avoided if the nerve has not been decompressed or translocated.
REFERENCES
- Allieu Y. Raideurs et arthrolyses du coude. Rev Chir Orthop 1989;75(suppl 1):156-166.
- Antuna SA, Morrey BF, Adams RA, et al. Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: long-term outcome and complications. J Bone Joint Surg Am 2002;84-A(12):2168-2173.
- Chantelot C, Fontaine C, Migaud H, et al. Etude retrospective de 23 arthrolyses du coude pour raideur post-traumatique: facteurs prédictifs du résultat. Rev Chir Orthop 1999;85:823-827.
- Cikes A, Jolles BM, Farron A. Open elbow arthrolysis for posttraumatic elbow stiffness. J Orthop Trauma 2006;20:405-409.
- Cohen MS, Hastings H II. Posttraumatic contracture of the elbow. Operative release using a lateral collateral ligament sparing approach. J Bone Joint Surg Br 1998;80(5):805-812.
- Duke JB, Tessler RH, Dell PC. Manipulation of the stiff elbow with patient under anesthesia. J Hand Surg Am 1991;16:19-24.
- Esteve P, Valentin P, Deburge A, et al. Raideurs et ankyloses post-traumatiques du coude. Rev Chir Orthop 1971;57(suppl 1):25-86.
- Gelinas JJ, Faber KJ, Patterson SD, et al. The effectiveness of turnbuckle splinting for elbow contractures. J Bone Joint Surg Br 2000;82:74-78.
- Husband JB, Hastings H II. The lateral approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg Am 1990;72(9):1353-1358.
- Itoh Y, Saegusa K, Ishiguro T, et al. Operation for the stiff elbow. Int Orthop 1989;13:263-268.
- Mansat P, Morrey BF. The column procedure: a limited surgical approach for the treatment of stiff elbows. J Bone Joint Surg Am 1998;80(11):1603-1615.
- Mansat P, Morrey BF, Hotchkiss RN. Extrinsic contracture: the column procedure, lateral and medial capsular releases. In: Morrey BF, ed. The Elbow and Its Disorders, ed 3. Philadelphia: WB Saunders, 2000:447-456.
- Marti RH, Kerkhoffs GM, Maas M, et al. Progressive surgical release of a posttraumatic stiff elbow: technique and outcome after 2-18 years in 46 patients. Acta Orthop Scand 2002;73:144-150.
- Merle D'Aubigne R, Kerboul M. Les opérations mobilisatrices des raideurs et ankylose du coude. Rev Chir Orthop 1966;52:427-448.
- Morrey BF. Post-traumatic contracture of the elbow: operative treatment, including distraction arthroplasty. J Bone Joint Surg Am 1990;72(4):601-618.P.1196
- Morrey BF. The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.
- Morrey BF. The use of splints for the stiff elbows. Perspect Orthop Surg 1990;1:141-144.
- O'Driscoll SW, Horii E, Morrey BF. Anatomy of the attachment of the medial ulnar collateral ligament. J Hand Surg Am 1992;17:164.
- Park MJ, Kim HG, Lee JY. Surgical treatment of post-traumatic stiffness of the elbow. J Bone Joint Surg Br 2004;86(8):1158-1162.
- Rosenwasser M. Sequelae of fractures of the elbow. Presented at 11th Trauma Course, AIOD, Strasbourg, 2005.
- Urbaniak JR, Hansen PE, Beissinger SF, et al. Correction of posttraumatic flexion contracture of the elbow by anterior capsulotomy. J Bone Joint Surg Am 1985;67(8):1160-1164.
- Wada T, Ishii S, Usui M, et al. The medial approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg Br 2000;82:68-73.
- Weiss AP, Sachar K. Soft tissue contractures about the elbow. Hand Clin 1994;10:439-451.
- Willner P. Anterior capsulectomy for contractures of the elbow. J Int Coll Surg 1948;11:359-362.
