Extensor Tenosynovitis: Pathophysiology and Clinical Presentation
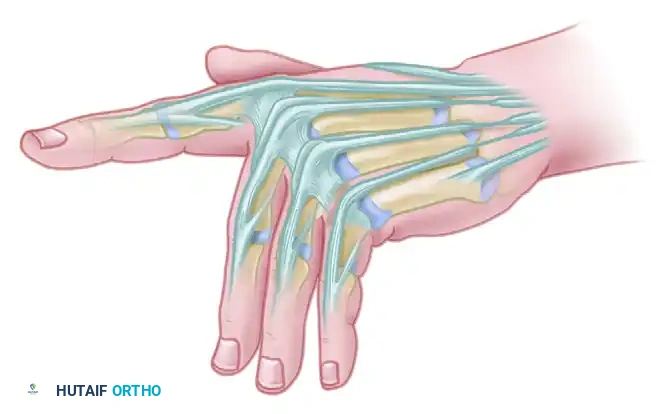
Extensor tenosynovitis of the wrist and digits is a hallmark manifestation of inflammatory arthritides, most notably rheumatoid arthritis (RA), though it may also present in seronegative spondyloarthropathies, crystalline arthropathies, or as an idiopathic condition. Clinically, it manifests as a visible, boggy swelling over the dorsal aspect of the wrist and hand. Unlike acute infectious tenosynovitis, inflammatory extensor tenosynovitis is usually relatively painless, which often leads to a delay in patients seeking medical attention.
This condition is predominantly observed at the wrist level, where the extensor tendons pass beneath the tight, unyielding extensor retinaculum. The presence of mobile, longitudinal masses that move synchronously with the excursion of the extensor tendons is a critical diagnostic sign. This mobility distinguishes extensor tenosynovitis from dorsal capsular synovitis (which remains static during tendon excursion) and dorsal carpal ganglion cysts (which are typically more focal, firm, and transilluminate).
As the synovial tissue hypertrophies, the resulting nodules and thickened paratenon may impinge on the distal or proximal edges of the extensor retinaculum. This mechanical impingement produces discomfort, a sensation of catching, and limits concomitant wrist and finger extension. If left unchecked, the chronic inflammatory milieu—characterized by the release of matrix metalloproteinases and collagenases—combined with mechanical friction, inevitably leads to attritional tendon damage and subsequent rupture.
Clinical Pearl: The "hourglass" sign is frequently observed in severe extensor tenosynovitis. The hypertrophic synovium bulges proximally and distally to the extensor retinaculum, while the retinaculum itself constricts the swelling in the center, creating an hourglass appearance on the dorsal wrist.
Nonoperative Management and Its Limitations
Initial management of extensor tenosynovitis is inherently conservative, focusing on mitigating the inflammatory response and protecting the vulnerable tendon structures.
- Medical Management: Optimization of systemic disease control is paramount. The use of Disease-Modifying Antirheumatic Drugs (DMARDs) and biologic agents has drastically reduced the incidence of severe tenosynovitis and subsequent tendon ruptures in the modern era.
- Splinting: Volar resting splints that place the wrist in slight extension can relieve tension on the extensor tendons and reduce mechanical friction beneath the retinaculum, often leading to symptom resolution in early stages.
- Corticosteroid Injections: The use of local corticosteroid injections in the dorsal compartments is highly controversial. While they may provide transient relief of synovial swelling, they carry a significant risk of accelerating tendon degeneration and precipitating iatrogenic extensor tendon rupture. Therefore, their use is strictly limited and generally discouraged in the presence of advanced disease or impending rupture.
If there is no substantial clinical improvement in the tenosynovitis following 3 to 6 months of aggressive nonoperative treatment, or if there are signs of impending tendon rupture (such as sudden loss of active extension in a single digit), an extensor tenosynovectomy is strongly recommended.
Extensor Tendon Rupture: Biomechanics and Patterns
Rheumatoid tenosynovitis is a leading cause of spontaneous tendon rupture, resulting in profound deformity and functional disability. The pathophysiology of rupture is multifactorial, involving both enzymatic degradation by the invasive pannus and mechanical abrasion.
Caput Ulnae and Vaughn-Jackson Syndrome
A critical biomechanical contributor to extensor tendon rupture is the dorsal subluxation of the distal ulna, commonly referred to as caput ulnae syndrome. In the rheumatoid wrist, destruction of the distal radioulnar joint (DRUJ) ligaments and the triangular fibrocartilage complex (TFCC) allows the ulnar head to subluxate dorsally. Concurrently, the carpus supinates and subluxates volarly.
The diseased extensor tendons are forced to glide between the sharp, arthritic, and dorsally prominent distal ulnar head and the tight, intact dorsal carpal ligament. This creates a severe abrasive point.
The rupture pattern is highly predictable and sequential, known as Vaughn-Jackson syndrome.
1. The extensor digiti minimi (EDM) and the extensor digitorum communis (EDC) to the small finger are typically involved first due to their immediate proximity to the subluxated ulnar head.
2. The rupture then progresses radially to involve the EDC of the ring finger.
3. Subsequently, it sequentially affects the more radial digital extensors (middle and index fingers).
Surgical Warning: The clinical examination usually underestimates the true extent of tendon irritation, thinning, and rupture. A patient may present with a dropped small finger, but intraoperative exploration frequently reveals impending ruptures of the ring and middle finger extensors. The surgeon must be prepared for a more complex reconstruction than anticipated.
Extensor Pollicis Longus (EPL) Rupture
The extensor pollicis longus (EPL) tendon is another frequent casualty of rheumatoid tenosynovitis. Because of its tortuous course around Lister's tubercle—where it angles sharply through an enclosed fibro-osseous tunnel (the third dorsal compartment)—it is subjected to immense mechanical stress. The combination of increased compartmental pressure from synovitis and the mechanical fulcrum of the tubercle frequently leads to attritional rupture of the EPL, presenting as an inability to actively extend the interphalangeal joint of the thumb and retropulse the thumb.
The "Pseudotendon" Phenomenon
At the time of surgical exploration, the surgeon may observe a white strip of connective tissue bridging the gap of the ruptured tendon. This is a pseudotendon—a fibrous band formed by the thickened paratenon and surrounding scar tissue. While it may transmit enough force to allow for some weak, limited metacarpophalangeal (MCP) joint extension, it is not a true tendon and lacks the structural integrity required for normal function. It must be excised during reconstruction.
Preoperative Evaluation and Surgical Timing
If a ruptured extensor tendon is diagnosed within a few days of the event, direct primary repair may be possible, provided the remaining tendon ends are of adequate quality. However, in the context of rheumatoid arthritis, the tendon ends are often severely frayed, degenerated, and retracted, making direct repair impossible even in acute settings.
If surgery must be delayed for several days due to medical optimization or scheduling, it is imperative to splint the wrist in extension. This relieves the constant tension on the remaining intact tendons, preventing further sequential ruptures.
When the ruptured tendon is diagnosed after several weeks (chronic rupture), the muscle belly will have contracted, and the tendon ends will have degenerated further. In these scenarios, direct repair is obsolete, and the surgeon must resort to segmental tendon grafting or side-to-side tendon transfers.
Surgical Technique: Tenosynovectomy and Reconstruction
The surgical management of extensor tenosynovitis and tendon rupture requires a meticulous, step-wise approach to eradicate the inflammatory tissue, address bony prominences, and restore biomechanical function.
1. Positioning and Approach
- The patient is positioned supine with the arm on a hand table. A well-padded pneumatic tourniquet is applied to the proximal arm.
- A dorsal longitudinal incision is made in the midline of the wrist, extending from the distal radius to the mid-metacarpal level. Alternatively, a gently curved or lazy-S incision can be utilized to prevent scar contracture.
- Full-thickness fasciocutaneous flaps are elevated. Extreme care must be taken to identify and protect the superficial branch of the radial nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly.
2. Extensor Retinaculum Management and Synovectomy
- The extensor retinaculum is identified. To prevent postoperative bowstringing while allowing access to the compartments, the retinaculum is typically divided over the 6th dorsal compartment and reflected radially, or step-cut to allow for later lengthening and repair.
- A radical extensor tenosynovectomy is performed. All hypertrophic, diseased synovium is meticulously dissected from the extensor tendons. The surgeon must inspect each tendon circumferentially, removing pannus that invades the tendon substance while preserving the intrinsic longitudinal blood supply.
- A synovectomy is always indicated in the region of the rupture and the planned repair.
3. Addressing the Distal Ulna
- If caput ulnae syndrome is present, the abrasive bony prominence must be eliminated to prevent failure of the tendon reconstruction.
- This is typically achieved via a distal ulnar resection (Darrach procedure) or a distal radioulnar arthrodesis with proximal ulnar pseudarthrosis (Sauvé-Kapandji procedure).
- The dorsal capsule over the DRUJ must be meticulously repaired to provide a smooth gliding surface for the reconstructed tendons.
4. Tendon Reconstruction Strategies
The choice of reconstruction depends on the number of ruptured tendons and the availability of local donor motors.
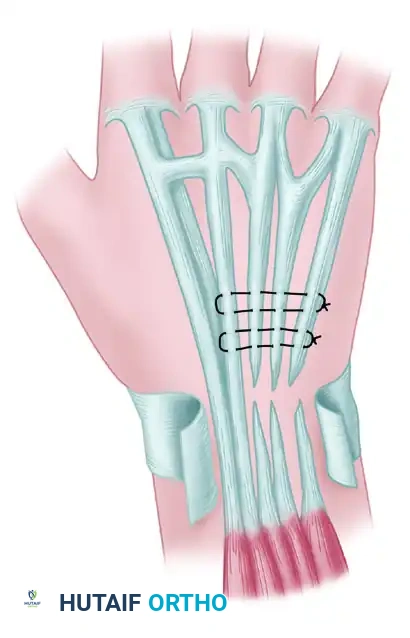
A. Single or Double Tendon Rupture (e.g., Ring and Little Fingers)
If the tendon of the ring finger or little finger alone is ruptured, or if both are ruptured, repair can be accomplished by suturing the distal segments of the ruptured tendons to the adjacent intact middle finger extensor tendon (EDC III).
* This is performed as a side-to-side tendon transfer under appropriate tension.
* The proximal stumps of the ruptured tendons are excised or sutured to the intact tendon to provide additional motor force.
B. Alternative Motors for the Little Finger
* The extensor indicis proprius (EIP) can be harvested and transferred to the distal stump of the EDM or EDC V to restore independent small finger extension.
* Another alternative is the transfer of the extensor pollicis brevis (EPB) as a motor. However, this is only viable if it is also necessary to arthrodese the metacarpophalangeal (MCP) joint of the thumb due to advanced rheumatoid destruction.
C. Multiple Tendon Ruptures (Three or More)
When three extensor tendons (middle, ring, and little fingers) have been ruptured for an extended period, side-to-side transfers to the index finger are insufficient and will result in an extensor lag. The transfer of a robust, independent motor is indicated.
* An acceptable and highly effective source for this motor is the flexor digitorum superficialis (FDS) of the ring finger.
* The FDS tendon is harvested, routed through the interosseous membrane or around the radial border of the forearm, and interwoven into the distal stumps of the ruptured extensors.
* This tendon has excellent excursion and might be even more effective because of the tenodesing effect—when the wrist is flexed, the transferred tendon naturally tightens, augmenting digital extension.
D. Extensor Pollicis Longus (EPL) Reconstruction
* EPL tendon rupture is most reliably repaired by transfer of the extensor indicis proprius (EIP).
* The EIP is identified at the index MCP joint (it lies ulnar to the EDC tendon), divided, and withdrawn to the wrist. It is then rerouted towards the thumb and interwoven into the distal EPL stump using a Pulvertaft weave.
* This is a highly useful and predictable transfer, applicable not only in rheumatoid arthritis but also when the EPL ruptures from other causes (e.g., distal radius fractures).
5. Closure and Splinting
- Following tendon reconstruction, the extensor retinaculum is repositioned. It is often placed deep to the extensor tendons to provide a smooth, vascularized barrier between the tendons and the underlying carpal bones/radiocarpal joint capsule, preventing future abrasion.
- Repair the capsule, centralize the common extensor tendon, and perform intrinsic releases and transfers when indicated to correct associated deformities (e.g., ulnar drift).
- The skin is closed over a suction drain to prevent hematoma formation.
Postoperative Protocol and Rehabilitation
The success of extensor tendon reconstruction relies heavily on strict adherence to a phased postoperative rehabilitation protocol. The repaired or transferred tendons must be protected from excessive tension while allowing enough glide to prevent restrictive adhesions.
- Immediate Postoperative Phase (0-3 Weeks):
- Apply a rigid volar splint in the operating room.
- Positioning: The wrist is immobilized in 10 to 15 degrees of extension, the metacarpophalangeal (MCP) joints in full extension (0 degrees), and the proximal interphalangeal (PIP) joints left free or in slight flexion to prevent collateral ligament contracture.
- Strict elevation is maintained to minimize edema.
- Intermediate Phase (3-6 Weeks):
- The rigid surgical splint is transitioned to a custom thermoplastic dynamic or static progressive splint.
- Active flexion and passive extension exercises are initiated under the strict guidance of a certified hand therapist.
- The tenodesis effect is utilized to safely glide the tendons without overloading the repair sites.
- Late Phase (6-12 Weeks):
- Gradual weaning from the splint during the day.
- Active extension exercises are initiated.
- Progressive strengthening begins at 8 weeks, tailored to the patient's underlying rheumatoid disease status and overall joint stability.
By combining meticulous surgical technique—addressing both the inflammatory soft tissue and the abrasive bony pathology—with rigorous postoperative therapy, the orthopedic surgeon can successfully restore function and prevent further disability in patients suffering from extensor tenosynovitis and tendon rupture.
📚 Medical References
- extensor tenosynovitis of the extensor carpi ulnaris tendon sheath, Am J Orthop 31:637, 2002.
- Long WT, Filler BC, Cox E II, et al: Toxic shock syndrome after a human bite to the hand, J Hand Surg 13A:957, 1988.
- Louis DB, Jebson PJ: Mimickers of hand infections, Hand Clin 14:519, 1998.
- Lunn JV, Rahman KJ, Macey AC: Streptococcus milleri infection, J Hand Surg 26:56, 2001.
- MacLennan JD: The histotoxic clostridial infection of man, Bacteriol Rev 26:177, 1962.
- Mahajan AL, Ajmal N, Barry J, et al: Could your case of necrotizing fasciitis be pyoderma gangrenosum? Br J Plast Surg 58:409, 2005.
- Majeski JA, Alexander JW: Early diagnosis, nutritional support, and immediate extensive debridement improve survival in necrotizing fasciitis, Am J Surg 145:784, 1983.
- Malinowski RW, Strate RG, Perry JF Jr, et al: The management of human bite injuries of the hand, J Trauma 19:655, 1979.
- Maloon S, de Beer J de V, Opitz M, et al: Acute fl exor tendon sheath infections, J Hand Surg 15A:474, 1990.
- Mathews RE, Gould JS, Kashlan MB: Diffuse pigmented villonodular tenosynovitis of the ulnar bursa, J Hand Surg 6A:64, 1981.
- Matsui T: Acute nonspecifi c fl exor tenosynovitis in the digits, J Orthop Sci 6:234, 2001.
- McAuliffe JA, Seltzer DG, Hornicek FJ: Upper extremity infections in patients seropositive for human immunodefi ciency virus, J Hand Surg 22A:1084, 1997.
- McCabe SJ, Murray JF, Ruhnke HL, et al: Mycoplasma infection of the hand acquired from a cat, J Hand Surg 12A:1085, 1987.
- Mehdi SA, Dunlop DG, Oliver CW: “Uneasy lies the hand in which rests the crown”: an unusual foreign body following a punch injury, J Hand Surg 25B:221, 2003.
- Mentec H, Chosidow O, Lafaurie P, et al: Necrotizing fasciitis caused by Neisseria meningitidis simultaneously involving an arm and a leg, Ann Dermatol Venereol 12:889, 1993.
- Miller JD: The importance of early diagnosis and surgical treatment of necrotizing fasciitis, Surg Gynecol Obstet 157:197, 1983.
- Minkin BI, Mills CL, Bullock DW, et al: Mycobacterium kansasii osteomyelitis of the scaphoid, J Hand Surg 12A:1092, 1987.
- Murray PM: Septic arthritis of the hand and wrist, Hand Clin 14:579, 1998.
- Nee PA, Lunn PG: Isolated anterior interosseous nerve palsy following herpes zoster infection: case report and review of the literature, J Hand Surg 14B:447, 1989.
- Neviaser RJ: Closed tendon sheath irrigation for pyogenic fl exor tenosynovitis, J Hand Surg 3A:462, 1978.
- Neviaser RJ: Tenosynovitis, Hand Clin 5:525, 1989.
- Neviaser RJ, Gunther SF: Tenosynovial infections of the hand— diagnosis and management: I. Acute pyogenic tenosynovitis of the hand, Instr Course Lect 29:108, 1980.
- Newman ED, Harrington TM, Torretti D, et al: Suppurative extensor tenosynovitis caused by Staphylococcus aureus, J Hand Surg 14A:849, 1989.
- O’Halloran LE, Bennett LL, Grothaus PC, et al: Sweet’s syndrome presenting as an acute hand infection, Plast Reconstr Surg 116:497, 2005.
- Patino JF: Necrotizing lesions of soft tissue: a review, World J Surg 15:235, 1991.
- Patzakis MJ, Wilkins J, Bassett RL: Surgical fi ndings in clenchedfi st injuries, Clin Orthop Relat Res 220:237, 1987.
- Peeples E, Boswick JA Jr, Scott FA: Wounds of the hand contaminated by human or animal saliva, J Trauma 20:393, 1980.
- Phair IC, Quinton DN: Clenched fi st human bite injuries, J Hand Surg 14B:86, 1989.
- Phillips CS, Falender R, Mass DP: The fl exor synovial sheath anatomy of the little fi nger: a macroscopic study, J Hand Surg 20A:636, 1995.
- Pinzur MS, Bednar M, Weaver F, et al: Hand infections in the diabetic patient, J Hand Surg 22B:1997.
- Prince H, Ispahani P, Baker M: A Mycobacterium malmoense infection of the hand presenting as a carpal tunnel syndrome, J Hand Surg 13B:328, 1988.
- Raborn GW, Grace M: Herpes simplex type 1 orofacial infections, Herpes 6:1, 1999.
- Rayan GM, Putnam JL, Cahill SL, et al: Eikenella corrodens in human mouth fl ora, J Hand Surg 13A:953, 1988.
- Reilly KE, Linz JC, Stern PJ, et al: Osteomyelitis of the tubular bones of the hand, J Hand Surg 22A:644, 1997.
- Reyes FA: Infections secondary to intravenous drug abuse, Hand Clin 5:629, 1989.
- Riehl J, Schmitt H, Bergmann D, et al: Tuberculous tenosynovitis of the hand: evaluation with B-mode ultrasonography, J Ultrasound Med 16:369, 1997.
- Rouse TM, Melangoni MA, Schulte WJ: Necrotizing fasciitis: a preventable disaster, Surgery 92:765, 1982.
- Said R, Volpin G, Grimberg B: Hand infections due to noncholera Vibrio after injuries from St. Peter’s fi sh ( Talapia zilii ), J Hand Surg 23B:808, 1998.
- Sanger JR, Stampfl DA, Franson TR: Recurrent granulomatous synovitis due to Mycobacterium kansasii in a renal transplant recipient, J Hand Surg 12A:436, 1987.
- Schecter WP, Markison RE, Jeffrey RB, et al: Use of sonography in the early detection of suppurative fl exor tenosynovitis, J Hand Surg 14A:307, 1989.
- Schecter W, Meyer A, Schecter G, et al: Necrotizing fasciitis of the upper extremity, J Hand Surg 7A:15, 1982.
- Schmidt DR, Heckman JD: Eikenella corrodens in human bite infections of the hand, J Trauma 23:478, 1983.
- Schnall SB, Vu-Rose T, Holtom PD, et al: Tissue pressures in pyogenic fl exor tenosynovitis of the fi nger:
