Precise Surgical Exposure of the Shaft of the Ulna: Technique & Uses
Introduction & Epidemiology
The ulna, a critical component of the forearm skeleton, functions primarily as the stable column of the forearm, articulating proximally with the humerus and radius, and distally with the radius and the triangular fibrocartilage complex (TFCC). Its anatomical position, particularly the subcutaneous dorsal border, renders it the most accessible long bone in the forearm, making direct surgical exposure relatively straightforward. This accessibility facilitates intervention for a spectrum of pathologies, ranging from acute traumatic injuries to chronic conditions requiring reconstructive procedures.
Fractures of the ulnar shaft are common, occurring as isolated "nightstick" fractures, as components of both-bone forearm fractures (often in conjunction with radial shaft fractures), or as part of complex Monteggia fracture-dislocations. The epidemiology of ulnar fractures varies by age group and mechanism of injury, with isolated ulnar fractures frequently resulting from direct trauma, while both-bone forearm fractures and Monteggia injuries often involve higher energy mechanisms. The stability and functional integrity of the forearm are paramount for upper limb function, necessitating precise anatomical reduction and stable fixation when operative intervention is indicated. Beyond acute trauma, the ulnar shaft approach is indispensable for addressing delayed unions, nonunions, osteomyelitis, and performing corrective osteotomies for limb length discrepancies or rotational deformities, as well as for excising tumors or addressing congenital anomalies. Understanding the precise surgical anatomy and meticulous technique is fundamental to optimizing outcomes and minimizing complications.
Surgical Anatomy & Biomechanics
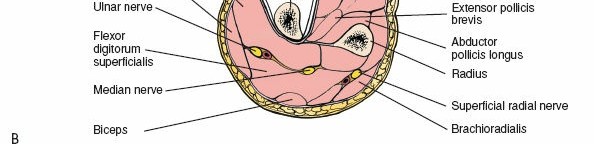
A thorough understanding of the ulnar anatomy and surrounding neurovascular structures is paramount for safe and effective surgical exposure. The ulna is an irregularly shaped long bone, broader proximally where it forms the trochlear notch for articulation with the trochlea of the humerus and the radial notch for articulation with the radial head. Distally, it tapers to a small head and a styloid process, articulating with the radius via the distal radioulnar joint (DRUJ) and indirectly with the carpus through the TFCC.
Osseous Landmarks
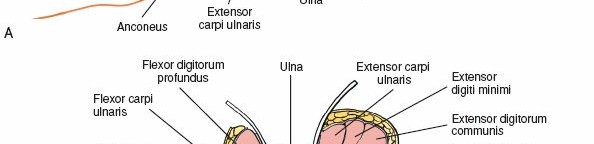
The most superficial and surgically relevant landmark is the subcutaneous border of the ulna (often referred to as the dorsal or posterior border). This sharp crest extends from the olecranon proximally to the ulnar styloid distally, serving as the attachment site for the shared aponeurosis of the flexor carpi ulnaris (FCU) and extensor carpi ulnaris (ECU) muscles. This border is palpable throughout its length, providing an excellent guide for skin incision and subsequent dissection.
Muscular Attachments & Fascial Planes
Several muscles attach to or originate from the ulna, but the most critical for this approach are the FCU and ECU, as they define the internervous plane.
- Flexor Carpi Ulnaris (FCU): Originates from the medial epicondyle (humeral head) and the medial aspect of the olecranon and upper two-thirds of the posterior border of the ulna (ulnar head). It is innervated by the ulnar nerve. Its fibers are medial to the subcutaneous border.
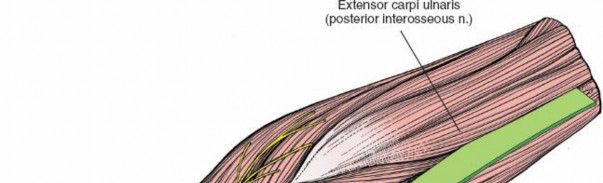
- Extensor Carpi Ulnaris (ECU): Originates from the lateral epicondyle (humeral head) and the posterior border of the ulna (ulnar head). It is innervated by the posterior interosseous nerve (PIN), a deep branch of the radial nerve. Its fibers are lateral to the subcutaneous border.
The internervous plane for this approach lies between the FCU (ulnar nerve innervation) and the ECU (radial nerve/PIN innervation). This is considered a true internervous plane, minimizing muscle denervation during exposure. However, as noted in the seed content, both muscles share a common aponeurosis attaching to the subcutaneous border of the ulna. This shared attachment makes separating them at their origin challenging, often necessitating a longitudinal incision through this common aponeurosis directly along the bone border. Subsequent subperiosteal elevation then mobilizes the muscle masses.
Other muscles relevant to broader ulnar exposure:
*
Flexor Digitorum Profundus (FDP):
Originates from the proximal three-fourths of the anterior and medial surfaces of the ulna and the interosseous membrane. Its fibers are deep and anterior to the FCU.
*
Pronator Quadratus:
Originates from the distal anterior ulna, crucial for distal ulnar and DRUJ stability.
*
Anconeus:
Originates from the lateral epicondyle and inserts into the lateral surface of the olecranon and proximal ulna. Can be partially reflected proximally.
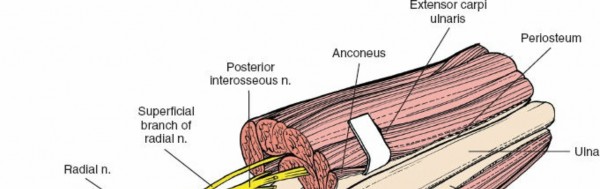
Neurovascular Structures
The direct ulnar approach is considered relatively safe regarding major neurovascular structures due to their anatomical position.
*
Ulnar Nerve and Artery:
Located on the medial side of the forearm, deep to the FCU muscle. With careful subperiosteal elevation of the FCU anteriorly, these structures are protected. They are not typically encountered directly unless dissection extends significantly anteriorly beyond the FDP.
*
Dorsal Ulnar Cutaneous Nerve:
A branch of the ulnar nerve, it typically arises in the distal forearm, passes dorsally beneath the FCU, pierces the deep fascia, and becomes superficial over the ulnar aspect of the wrist and hand. It is vulnerable during distal skin incision and subcutaneous dissection. Meticulous skin incision and careful blunt dissection in the subcutaneous plane are essential to minimize risk of injury or neuroma formation.
*
Posterior Interosseous Nerve (PIN):
As the motor branch of the radial nerve, the PIN is located on the radial side of the forearm, deep within the supinator muscle, and then continues between the superficial and deep extensors. It is generally not at direct risk during a pure posterior ulnar approach unless dissection is carried excessively laterally and deep into the extensor compartment, particularly proximally.
*
Perforating Vessels:
Small branches from the ulnar artery and posterior interosseous artery supply the periosteum and bone. Careful subperiosteal elevation minimizes disruption but some may require cauterization.
Biomechanics
The ulna serves as the fixed axis for forearm rotation, with the radius pivoting around it. Its stability is crucial for effective pronation and supination. The strong interosseous membrane connecting the ulna and radius transmits axial load from the radius to the ulna. Maintaining the anatomical length, alignment, and rotation of the ulna is critical for preserving DRUJ mechanics, elbow stability, and overall forearm function. A malunion or nonunion of the ulna can lead to significant functional impairment, including restricted forearm rotation, elbow stiffness, and pain.
Indications & Contraindications
The precise surgical exposure of the ulnar shaft is a versatile approach, indicated for a broad range of traumatic, degenerative, infectious, neoplastic, and developmental conditions.
Indications
The uses of the approach include the following:
1.
Open reduction and internal fixation (ORIF) of ulnar fractures:
* Isolated ulnar shaft fractures (nightstick fractures) with significant displacement, angulation, or rotational deformity.
* Displaced, comminuted, or unstable ulnar shaft fractures as part of both-bone forearm fractures.
* Ulnar shaft fractures associated with Monteggia fracture-dislocations, where stable ulnar fixation is critical for reducing and stabilizing the radiocapitellar joint.
2.
Treatment of delayed union or nonunion of ulnar fractures:
Requires revision surgery, often with debridement of fibrous tissue, bone grafting, and more rigid internal fixation.
3.
Osteotomy of the ulna:
* Corrective osteotomies for malunited fractures causing forearm rotational deformities or ulnar angulation.
* Corrective osteotomies for congenital deformities (e.g., Madelung's deformity).
4.
Treatment of chronic osteomyelitis of the ulna:
Involves extensive debridement of infected and necrotic bone, often followed by antibiotic therapy and potentially reconstructive procedures (e.g., bone grafting, vascularized flaps).
5.
Treatment of the fibrous anlage of the ulna in cases of ulnar clubhand (radial longitudinal deficiency):
Excision of the tethering fibrous band to improve forearm growth and alignment, often combined with osteotomies or other reconstructive procedures.
6.
Ulnar lengthening:
Indicated in cases of ulnar-sided deficiency or negative ulnar variance causing wrist pathology. Common applications include:
* Ulnar clubhand reconstruction.
* Cases of Kienböck's disease (stage II or III) with negative ulnar variance, to offload the lunate.
* Correction of Madelung's deformity.
7.
Ulnar shortening:
Indicated for conditions causing positive ulnar variance or ulnar impaction syndrome. Common applications include:
* Ulnar impaction syndrome.
* Distal radial malunion that results in relative ulnar length excess.
* DRUJ incongruity due to length mismatch.
8.
Biopsy or excision of benign or malignant tumors of the ulnar shaft.
9.
Removal of symptomatic or broken hardware
from previous ulnar fixation.
| Indication Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Traumatic |
- Displaced or unstable isolated ulnar shaft fractures (e.g., >10-15 degrees angulation, >50% displacement, significant rotational deformity in adults)
- Both-bone forearm fractures (ulna and radius) requiring anatomical reduction and stable fixation - Monteggia fracture-dislocations (unstable ulnar fracture often requires ORIF to reduce radial head) - Open ulnar fractures (Gustilo-Anderson Type II or greater) - Compartment syndrome requiring fasciotomy (rare as primary indication for this approach, but can be part of extensive trauma management) |
- Minimally displaced or non-displaced isolated ulnar shaft fractures (nightstick fractures)
- Stable, closed ulnar shaft fractures in children (often managed with casting) - Stable avulsion fractures of the olecranon or ulnar styloid (if not involving joint stability) - Stress fractures of the ulna (typically managed with activity modification and immobilization) |
| Degenerative |
- Ulnar impaction syndrome refractory to conservative management, requiring ulnar shortening osteotomy
- Kienböck's disease with negative ulnar variance, requiring ulnar lengthening osteotomy - Distal radial malunion causing positive ulnar variance and DRUJ symptoms, requiring ulnar shortening osteotomy |
- Mild to moderate ulnar impaction syndrome responsive to activity modification, NSAIDs, and corticosteroid injections
- Early Kienböck's disease stages (e.g., Stage I) - Asymptomatic ulnar variance |
| Infectious |
- Acute or chronic osteomyelitis of the ulna requiring debridement, sequestrectomy, and/or bone grafting
- Infected nonunion of ulnar fractures |
- Superficial soft tissue infections not involving bone (managed with antibiotics)
- Early, localized cellulitis without systemic signs (managed with antibiotics and monitoring) |
| Neoplastic |
- Biopsy of suspicious ulnar lesions
- Excision of benign tumors (e.g., osteochondroma, fibrous dysplasia, enchondroma) causing pain, deformity, or impending fracture - Resection of malignant tumors (often requiring reconstruction) |
- Asymptomatic, stable benign lesions with characteristic radiographic features (e.g., non-ossifying fibroma) requiring surveillance
- Small, clinically insignificant lesions identified incidentally |
| Developmental |
- Ulnar clubhand (radial longitudinal deficiency) with a fibrous anlage or bony deformity requiring excision, osteotomy, or lengthening
- Madelung's deformity causing pain or functional limitation, requiring corrective osteotomy (e.g., ulnar lengthening or radial osteotomy combined with distal ulnar epiphysiodesis) |
- Asymptomatic mild ulnar clubhand or Madelung's deformity
- Developmental conditions not causing functional deficits or pain, managed with observation |
| Revision Surgery |
- Symptomatic hardware requiring removal
- Nonunion or malunion requiring revision fixation, bone grafting, or osteotomy |
- Asymptomatic, well-fixed hardware
- Stable, asymptomatic malunions not causing functional deficit |
Contraindications
Absolute contraindications for the ulnar approach are few and generally apply to any surgical procedure:
* Uncontrolled systemic infection or sepsis.
* Patient factors precluding safe anesthesia or surgical tolerance.
* Insufficient soft tissue coverage or viability over the proposed surgical site (e.g., severe burns, extensive crush injury with questionable tissue viability), which may necessitate alternative approaches or staged reconstruction.
Relative contraindications include:
* Pre-existing severe scarring or contracture from previous surgeries or trauma, which may complicate dissection and increase risk of neurovascular injury.
* Active local infection (for elective procedures like osteotomy), though it becomes an indication for infected nonunion or osteomyelitis.
* Severe peripheral vascular disease compromising wound healing.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing surgical outcomes and minimizing complications.
Pre-Operative Imaging
- Standard Radiographs: Anteroposterior (AP) and lateral views of the forearm, including the elbow and wrist joints, are fundamental. These provide essential information on fracture morphology, displacement, angulation, and rotational deformity; extent of nonunion or malunion; presence of osteomyelitis (sclerosis, lucency, sequestrum); or tumor characteristics.
- Computed Tomography (CT) Scan: Indispensable for complex fractures, comminuted nonunions, osteomyelitis (especially with cortical involvement and medullary extension), or tumor assessment (defining extent and involvement of surrounding structures). CT with 3D reconstructions can precisely delineate fracture patterns, rotational deformities, and guide osteotomy planning.
- Magnetic Resonance Imaging (MRI): Useful for evaluating soft tissue involvement, assessing tumor extension into muscle or neurovascular bundles, differentiating osteomyelitis from other bone pathologies, or visualizing the fibrous anlage in ulnar clubhand.
- Ultrasound: Can be used to assess the integrity of the TFCC or to identify superficial neurovascular structures (e.g., dorsal ulnar cutaneous nerve) pre-operatively in revision cases.
Patient Counseling
A comprehensive discussion with the patient regarding the diagnosis, proposed surgical plan, potential benefits, risks (including infection, nonunion, nerve injury, hardware issues), expected recovery timeline, and realistic functional outcomes is paramount for informed consent.
Equipment
- Standard orthopedic instrument tray.
- Small fragment and/or large fragment plating sets (e.g., 3.5 mm LC-DCP, LCP, 2.7 mm LCP for smaller osteotomies).
- Standard bone reduction clamps (Verbrugge, point-to-point, broad fragment).
- Periosteal elevators (e.g., Langenbeck, Freer, Key).
- Bone rongeurs, curettes, osteotomes (for debridement, osteotomy).
- High-speed burr for precise osteotomies or debridement.
- Bone grafting instruments if autograft harvesting is anticipated (e.g., iliac crest or distal radius).
- Surgical loupes for magnified vision during critical dissections.
- Fluoroscopy (C-arm) for intra-operative assessment of reduction, hardware placement, and osteotomy accuracy.
Patient Positioning
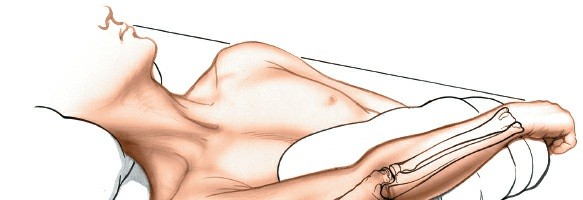
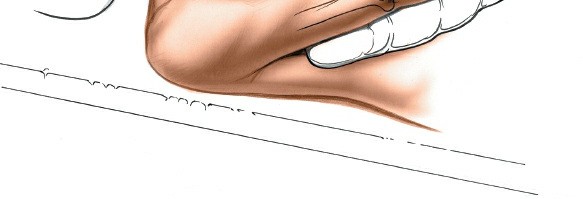
Place the patient supine on the operating table. The preferred method for forearm access involves placing the arm on a hand table , allowing for full circumferential access and precise control of pronation and supination. This is particularly crucial for fracture fixation or osteotomies where rotational alignment is critical.
A common positioning technique is to abduct the arm to 90 degrees at the shoulder with the elbow flexed to 90 degrees. This provides optimal exposure for the entire length of the ulna. Alternatively, as suggested in the seed content, the arm can be placed across the chest to expose the subcutaneous border of the ulna, which is suitable for more localized lesions or when less manipulation of the elbow/forearm is required.
Regardless of the precise arm position, the limb must be thoroughly prepared and draped in a sterile fashion from the axilla to the fingertips.
(Figure 4-17 from seed content, likely showing patient positioning with the arm across the chest).
Tourniquet Application: Exsanguinate the limb either by elevating it for 3 to 5 minutes or by applying a soft rubber bandage (Esmarch) from distal to proximal. Inflate a pneumatic tourniquet (either high on the arm or a mid-forearm tourniquet, depending on the extent of the pathology and surgeon preference) to a pressure sufficient to achieve a bloodless field (typically 250-300 mmHg, or 100 mmHg above systolic blood pressure). A bloodless field is essential for clear identification of anatomical structures and meticulous dissection.
Detailed Surgical Approach / Technique
The direct posterior approach to the ulnar shaft is a reliable and safe method for comprehensive exposure. The key is to identify the subcutaneous border and work in the well-defined internervous plane.
1. Skin Incision
The incision is made longitudinally along the subcutaneous border of the ulna. The length of the incision should be tailored to the extent of the pathology, ensuring adequate visualization proximal and distal to the area of interest.
* For midshaft fractures, a direct incision over the palpable ulnar border is made.
* For proximal lesions, the incision can extend towards the olecranon.
* For distal lesions, it can extend towards the ulnar styloid.
* When planning the incision, consider the natural lines of tension (Langer's lines) to optimize scar cosmesis, although functional access takes precedence.

(Demonstrates the initial skin incision along the ulnar shaft.)

(Likely showing the skin incision or initial subcutaneous dissection.)
2. Subcutaneous Dissection
Incise the skin and subcutaneous tissues. Identify and protect any superficial veins that can be ligated or cauterized if necessary. In the distal forearm, exercise caution to identify and retract the
dorsal ulnar cutaneous nerve
. This sensory nerve crosses the operative field dorsally in the distal aspect and is highly vulnerable to injury, which can result in a painful neuroma or numbness. Gentle blunt dissection and retraction are preferred over sharp dissection in this region.
(Illustrates the layers after skin incision, showing subcutaneous fat and underlying fascia before muscle identification.)
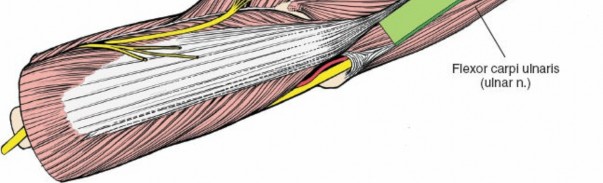
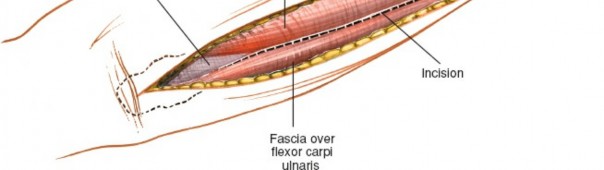
3. Identifying the Internervous Plane
The deep fascia overlying the forearm musculature is incised. The subcutaneous border of the ulna is now visible beneath the fascia. This border serves as the common origin for the shared aponeurosis of the FCU (medial/anterior) and ECU (lateral/posterior).
As detailed in the original seed content, the plane between the FCU and ECU muscles can be challenging to define directly due to their shared aponeurotic attachment to the subcutaneous border of the ulna.
To access the bone:
* Incise the common aponeurosis longitudinally, precisely along the subcutaneous border of the ulna. This incision should be carried down to the periosteum.
* The fibers of the extensor carpi ulnaris usually have to be detached from this aponeurosis, as mentioned. This effectively separates the muscle mass from its attachment to the ulna.
(Depicts the dissection through the aponeurosis, separating the ECU from its attachment along the ulnar border.)
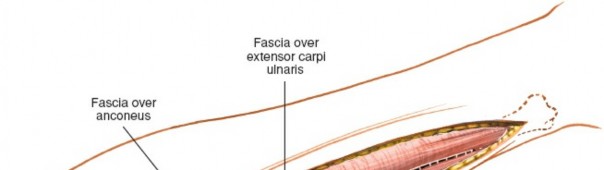
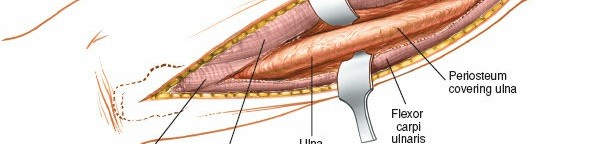
4. Exposure of the Ulna
Once the common aponeurosis is incised, subperiosteal elevation can commence.
* Using a sharp periosteal elevator (e.g., Key or Langenbeck), meticulously elevate the periosteum and the attached muscle masses off the ulnar shaft.
*
Anteriorly/Medially:
Elevate the FCU and the underlying Flexor Digitorum Profundus (FDP) from the anterior and medial surfaces of the ulna. These muscles are retracted anteriorly. Care should be taken to stay subperiosteal to protect the ulnar neurovascular bundle, which lies deep to the FCU.
*
Posteriorly/Laterally:
Elevate the ECU and the other extensor muscles (Extensor Digitorum, Extensor Indicis) from the posterior and lateral surfaces of the ulna. These muscles are retracted posteriorly.

(Shows subperiosteal elevation of the musculature, exposing the raw ulnar cortex.)
The entire length of the ulnar shaft can be exposed by extending the subperiosteal elevation as needed. Minimize soft tissue stripping to preserve periosteal blood supply, especially in cases of fracture or nonunion.
(The ulna is now fully exposed, with a fracture clearly visible mid-shaft.)
5. Management of Pathology (Fracture Fixation Example)
With the ulnar shaft exposed, the specific surgical procedure can be performed. For a ulnar shaft fracture:
*
Reduction:
The fracture fragments are meticulously reduced anatomically. This may involve traction, rotation, and direct manipulation using bone-holding clamps. Assess both length and rotational alignment. Fluoroscopy can be invaluable here.

(Depicts the fracture being reduced, likely with manual manipulation or reduction clamps.)
*
Fixation:
Stable internal fixation is achieved, typically with a contoured locking compression plate (LCP) or dynamic compression plate (DCP). Principles of AO surgery are applied:
*
Absolute stability (compression plating):
For simple, transverse, or short oblique fractures. Lag screws can be used across the fracture for interfragmentary compression.
*
Relative stability (bridging plating):
For comminuted fractures, maintaining length, alignment, and rotation without directly compressing small fragments.
* Plate selection depends on bone quality, fracture pattern, and patient factors. Generally, a minimum of three bicortical screws per fragment proximal and distal to the fracture is recommended for adequate stability.
(A plate is being applied to the reduced ulnar fracture.)
(The plate is secured with screws, demonstrating initial fixation.)
(The final plate and screw construct providing stable internal fixation of the ulna.)
For other indications:
*
Osteotomy:
Precise bone cuts are made using oscillating saws, guided by pre-operative planning. Bone graft may be applied, and rigid fixation with a plate is essential.
*
Osteomyelitis:
Debridement involves removal of all necrotic and infected bone until punctate bleeding is observed from healthy bone. Cultures are taken, and the wound may be left open or closed over antibiotic beads.
*
Tumor Excision:
Resection is performed with appropriate margins, followed by reconstruction if needed.
6. Wound Closure
Once the primary procedure is complete:
*
Irrigation:
Thoroughly irrigate the wound with sterile saline to remove bone debris and blood.
*
Hemostasis:
Ensure meticulous hemostasis.
*
Periosteum:
Reapproximate the periosteum with absorbable sutures if possible, although this is not always feasible or necessary.
*
Deep Fascia:
Reapproximate the deep fascia and the aponeurotic layer with absorbable sutures, restoring the muscle envelope around the ulna.
*
Subcutaneous Tissue:
Close the subcutaneous layer with interrupted absorbable sutures to obliterate dead space and reduce tension on the skin.
*
Skin:
Close the skin with non-absorbable sutures or staples.

(Shows closure of the deep fascial or subcutaneous layers.)

(Illustrates the final skin closure with sutures or staples.)
7. Post-Operative Dressing and Immobilization
Apply a sterile dressing to the wound. Depending on the stability of the fixation and the specific pathology addressed, a splint or cast may be applied for initial immobilization and comfort. For stable fixation of acute fractures, a bulky soft dressing may suffice, allowing early motion.

(Application of a sterile dressing to the closed wound.)
(Final post-operative immobilization with a splint or cast.)
Complications & Management
Despite its relative safety, the posterior ulnar approach, like any surgical intervention, carries potential risks. Understanding these complications and having strategies for their management is crucial.
General Surgical Complications
- Infection: Superficial wound infection or deep osteomyelitis.
- Hematoma/Seroma: Accumulation of blood or fluid, potentially requiring drainage.
- Anesthetic Complications: Standard risks associated with general or regional anesthesia.
- Thromboembolic Events: Deep vein thrombosis (DVT) or pulmonary embolism (PE), though rare in upper extremity surgery.
- Complex Regional Pain Syndrome (CRPS): A rare but debilitating post-operative pain syndrome.
Specific Complications of Ulnar Approach
| Complication | Incidence | Etiology | Salvage Strategies & Management |
|---|---|---|---|
| Nerve Injury: | |||
| Dorsal Ulnar Cutaneous Nerve | Common (5-15% sensory deficit) | Direct trauma during skin incision or subcutaneous dissection; excessive traction or entrapment during closure. |
-
Prevention:
Meticulous subcutaneous dissection; identify and protect nerve distally.
- Management: - Neuropraxia/Axonotmesis: Observation, pain management, nerve gliding exercises, reassuring patient that recovery often occurs. - Neuroma in continuity/Transection: Surgical exploration, neurolysis, or resection of neuroma with transposition or graft if symptomatic and persistent after 6-12 months. |
| Ulnar Nerve | Rare (<1%) | Accidental injury during deep anterior retraction (proximal exposure) or aggressive dissection around the FCU muscle. |
-
Prevention:
Maintain strict subperiosteal dissection anteriorly; avoid excessive anterior retraction.
- Management: Immediate post-operative neurological assessment. - Neuropraxia: Observation, supportive care. - Significant Deficit/Transection: Urgent surgical exploration, nerve repair (direct suture or graft) within 72 hours. Post-operatively, physical therapy for muscle re-education. |
| Posterior Interosseous Nerve (PIN) | Extremely Rare (<0.1%) | Excessive lateral retraction/stripping of the extensor muscle mass, particularly proximally near the supinator. |
-
Prevention:
Limit lateral dissection; avoid aggressive proximal lateral stripping.
- Management: As per ulnar nerve injury; urgent exploration for significant deficit. |
| Vascular Injury: | Rare (<0.1%) | Injury to ulnar artery or its perforators during deep dissection or enthusiastic screw placement. |
-
Prevention:
Meticulous hemostasis, careful drilling, avoid plunging drill bits.
- Management: Intraoperative repair of vessel if identified. Post-operative monitoring for signs of ischemia; angiogram if suspicion of occult injury. Exploration and repair by vascular surgeon if needed. |
| Nonunion / Delayed Union: | Varies (3-10% for fractures) | Inadequate reduction, unstable fixation, extensive soft tissue stripping, infection, poor bone biology, patient non-compliance (smoking, NSAID use). Higher risk in open fractures or re-operations. |
-
Management:
- Delayed Union: Conservative management, bone stimulators, activity modification. - Nonunion: Revision surgery with debridement of fibrous tissue, stable internal fixation (larger/stiffer plate), autologous bone grafting (iliac crest, distal radius), biological adjuncts (BMPs, PRP). Infection must be ruled out/treated. |
| Malunion: | Varies (2-5%) | Inaccurate reduction (angular, rotational, length), premature weight-bearing, implant failure. Affects forearm rotation and DRUJ function. |
-
Management:
- Asymptomatic/Mild: Observation. - Symptomatic/Functional Impairment: Corrective osteotomy (opening/closing wedge) with stable internal fixation. Pre-operative CT with 3D reconstruction is essential for planning. |
| Hardware-Related: | Common (10-20% for removal) | Prominent hardware causing soft tissue irritation, breakage, loosening, infection around hardware. |
-
Management:
- Irritation/Prominence: Elective hardware removal after bony union (typically 12-18 months). - Breakage/Loosening: Suggests nonunion; requires revision surgery, often with larger plate and bone grafting. - Infection: Debridement, targeted antibiotics; hardware removal once union achieved or if acute infection. |
| Post-operative Infection: | 1-5% | Contamination during surgery, hematoma formation, patient co-morbidities (diabetes, immunosuppression). |
-
Management:
- Superficial: Oral antibiotics, local wound care. - Deep (Osteomyelitis): Surgical debridement, tissue/bone cultures, prolonged intravenous antibiotics, potentially hardware removal if infection persists or union is established. Negative pressure wound therapy. |
| Refracture after Hardware Removal: | 2-5% | Premature hardware removal before bone remodeling is complete; inadequate rehabilitation; repeat trauma. |
-
Prevention:
Ensure complete radiographic union and cortical remodeling before removal (minimum 12-18 months for adults). Gradual return to activity.
- Management: Re-fixation of the refracture, often with a longer plate and potentially bone grafting. |
| Compartment Syndrome: | Rare (<1%) | Untreated severe trauma, reperfusion injury after prolonged ischemia, significant post-operative hematoma. |
-
Prevention:
Close monitoring of limb (pain, pallor, pulselessness, paresthesia, paralysis).
- Management: Emergent fasciotomy. |
| Scarring/Adhesions: | Varies | Extensive soft tissue stripping, poor wound healing, prolonged immobilization. May limit forearm rotation. |
-
Prevention:
Meticulous soft tissue handling, minimal stripping, early controlled range of motion.
- Management: Aggressive physical therapy, scar massage. Surgical adhesiolysis in refractory cases, although often with guarded prognosis. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional outcomes following ulnar shaft surgery. Protocols are tailored to the specific pathology addressed, the stability of fixation, and the individual patient's healing capacity.
Immediate Post-Operative Phase (Days 0-14)
- Immobilization: A well-padded long arm splint or brace is typically applied for comfort and initial protection, especially after fracture fixation or osteotomy. For stable constructs, gentle motion may be initiated sooner.
- Pain Management: Multimodal analgesia including NSAIDs, acetaminophen, and opioid analgesics as needed.
- Edema Control: Elevation of the limb above heart level, gentle active range of motion (AROM) of the digits and shoulder, and intermittent cold therapy.
- Wound Care: Daily dressing changes as per institutional protocol, monitoring for signs of infection or skin complications. Suture removal typically at 10-14 days.
Early Mobilization Phase (Weeks 2-6/8)
-
Initiation of Range of Motion (ROM):
Once adequate pain control is achieved and wound healing is satisfactory, controlled AROM of the elbow and wrist is initiated.
- Forearm Rotation: Gentle active pronation and supination may begin, carefully progressing based on fracture stability (fluoroscopic confirmation of union if concerned). Avoid passive stretching that could disrupt early healing or irritate soft tissues.
- Elbow and Wrist Flexion/Extension: AROM within pain-free limits.
- Strengthening (Isometric): Isometric exercises for wrist and hand muscles can be started.
- Scar Management: Gentle scar massage once the wound is completely closed to prevent adhesions.
- Protection: Continue to avoid heavy lifting, pushing, or pulling. The splint may be transitioned to a removable brace or discontinued based on radiographic evidence of early union and clinical stability.
Intermediate Strengthening Phase (Weeks 8-16)
- Progressive ROM: Progress to full AROM of the elbow, wrist, and forearm as tolerated. Gentle passive ROM may be introduced by a therapist if active motion is limited.
- Strengthening: Gradually introduce progressive resistance exercises for the forearm flexors, extensors, pronators, and supinators. Hand grip strengthening.
- Proprioception: Exercises to improve proprioception and neuromuscular control.
- Return to Activity: Gradually return to light daily activities. Avoid impact activities or heavy lifting. Radiographic evidence of cortical bridging and callus formation should be present.
Advanced Functional Phase (Weeks 16+)
- Advanced Strengthening: Progressive loading and strengthening exercises tailored to patient's occupational or athletic demands. This includes eccentric loading and higher-resistance activities.
- Sport/Work-Specific Training: For athletes or individuals with physically demanding jobs, sport or work-specific drills and simulations are incorporated.
- Monitoring: Continued monitoring for pain, swelling, and functional limitations. Radiographic assessment for complete bony union.
Hardware Removal
- Timing: Elective hardware removal is generally considered after complete bony union and cortical remodeling, typically 12-18 months post-operatively in adults. In children, removal may be indicated earlier to prevent growth disturbance or once bone healing is confirmed. For complex cases or osteotomies, removal may be deferred longer.
- Indications: Symptomatic hardware (e.g., pain, soft tissue irritation, prominence), infection, or patient request (e.g., young, active individuals wishing to reduce risk of refracture upon re-injury).
- Post-Removal: Short period of protection (e.g., 2-4 weeks in a brace) followed by progressive activity return to minimize refracture risk.
Summary of Key Literature / Guidelines
The surgical management of ulnar shaft pathology is guided by established orthopedic principles and evolving evidence-based practices.
- AO Principles: The Arbeitsgemeinschaft für Osteosynthesefragen (AO Foundation) principles remain fundamental to fracture fixation. These emphasize anatomical reduction, stable internal fixation, preservation of blood supply, and early, pain-free mobilization. For ulnar shaft fractures, both absolute stability (compression plating for simple patterns) and relative stability (bridging plating for comminuted patterns) are employed depending on the fracture morphology. The application of locking plates has provided improved stability, particularly in osteopenic bone or complex fracture patterns.
- Forearm Fracture Management: Current guidelines, such as those from the American Academy of Orthopaedic Surgeons (AAOS), advocate for anatomical reduction and stable internal fixation for displaced adult forearm fractures to restore length, rotation, and alignment, thereby minimizing the risk of malunion, nonunion, and post-traumatic stiffness. For Monteggia fractures, stable ulnar fixation is critical for indirect reduction of the radial head.
- Nonunion and Malunion: The management of ulnar nonunions often requires revision surgery with robust fixation and autogenous bone grafting to enhance biological healing. Treatment of malunions frequently involves corrective osteotomies to restore forearm rotation and length, emphasizing meticulous pre-operative planning with 3D imaging to define the deformity.
- Ulnar Shortening/Lengthening: For conditions like ulnar impaction syndrome or Kienböck's disease, ulnar shortening or lengthening osteotomies have well-documented techniques and indications. The success of these procedures relies on precise osteotomy execution and rigid internal fixation to allow for early motion and predictable union.
- Infectious Conditions: Management of ulnar osteomyelitis follows established infectious disease and orthopedic surgery guidelines, emphasizing thorough surgical debridement of necrotic and infected tissue, culture-directed antimicrobial therapy, and reconstruction of bone defects.
- Textbook References: Classic orthopedic texts such as Campbell's Operative Orthopaedics, Rockwood and Green's Fractures in Adults, and Hoppenfeld's Surgical Exposures in Orthopaedics provide comprehensive descriptions of the ulnar approach and its applications, serving as foundational references for trainees and practicing surgeons. Recent literature continues to refine techniques, evaluate implant performance, and optimize rehabilitation protocols, further enhancing patient outcomes in ulnar shaft surgery. Continuous engagement with contemporary literature and surgical education is essential for staying abreast of best practices.
Clinical & Radiographic Imaging