INTRODUCTION TO BENIGN BONE TUMORS OF THE HAND
The management of primary bone tumors in the hand skeleton presents a unique orthopedic challenge. The intricate anatomy, minimal soft-tissue envelope, and high biomechanical demands of the digits require a delicate balance between aggressive oncologic clearance and the preservation of maximal hand function. While malignant primary bone tumors of the hand are exceedingly rare, benign lesions—such as enchondromas, benign osteoblastomas, aneurysmal bone cysts (ABCs), and giant cell tumors (GCTs)—are encountered with relative frequency in clinical practice.
This comprehensive guide details the pathophysiology, clinical presentation, biomechanical implications, and step-by-step surgical management of these destructive, yet benign, osseous lesions.
ENCHONDROMA
Enchondromas are the most common and destructive primary bone tumors of the hand skeleton. Originating from displaced rests of physeal cartilage that fail to undergo normal endochondral ossification, these benign hyaline cartilage neoplasms typically manifest in the tubular bones of the hand.
Clinical Presentation and Pathophysiology
The most frequent anatomical location for an enchondroma is the proximal metaphysis of the proximal phalanx. In this region, the tumor characteristically presents as an eccentric and expansile lytic lesion. Because the hand possesses a thin cortical shell and minimal overlying soft tissue, the loculated medullary tumor often expands the bony cortex, leading to visible, asymmetrical enlargement of the affected finger.
Clinical Pearl: Pathological fracture is the most common presenting complication of a hand enchondroma. The expansile nature of the tumor thins the cortex, creating a significant biomechanical stress riser. Routine torsional forces generated during simple grip or pinch can precipitate an acute fracture through the weakened metaphyseal bone.
While most enchondromas are solitary, surgeons must maintain a high index of suspicion for syndromic presentations:
* Ollier Disease: A non-hereditary dysplasia characterized by multiple enchondromatosis. Patients present with extensive, asymmetric cartilaginous lesions that can cause severe angular deformities and limb-length discrepancies.
* Maffucci Syndrome: A rare congenital disorder characterized by multiple enchondromatosis associated with symmetrical, superficial, and deep soft-tissue hemangiomas, typically visible on the hands and legs. This syndrome carries a significantly higher risk of malignant transformation to chondrosarcoma compared to solitary lesions.
Diagnostic Evaluation
Diagnosis is primarily established through a combination of physical examination and orthogonal radiography. Radiographs typically reveal a well-circumscribed, radiolucent, expansile lesion with central calcifications (the classic "rings and arcs" or "popcorn" calcification pattern of chondroid matrix).
Differential diagnoses for destructive lytic lesions in the hand include:
* Epidermal inclusion cysts (typically in the distal phalanx following penetrating trauma)
* Giant cell tumors of bone
* Aneurysmal bone cysts
* Osteoid osteoma
Surgical Management: Curettage and Bone Grafting
The gold standard of treatment for symptomatic or structurally compromising solitary enchondromas is meticulous intralesional curettage followed by bone grafting. Digits rendered completely dysfunctional from severe, multiple enchondromas or massive hemangiomas (as seen in advanced Maffucci syndrome) are often best managed with ray amputation to restore overall hand mechanics.

Preoperative radiograph demonstrating an eccentric, expansile enchondroma of the proximal phalanx.
Step-by-Step Surgical Technique
- Patient Positioning and Anesthesia: The patient is placed supine with the operative arm extended on a radiolucent hand table. Regional anesthesia (brachial plexus block) or general anesthesia is utilized. A well-padded pneumatic upper arm tourniquet is applied to ensure a bloodless surgical field.
- Surgical Approach: A midaxial or dorsal approach is selected based on the eccentricity of the lesion.
- Midaxial Approach: Incision is made along the neutral line of the digit (connecting the apices of the flexion creases). The neurovascular bundle is identified and protected volarly. The extensor mechanism is retracted dorsally.
- Dorsal Approach: A longitudinal incision is made over the phalanx. The extensor tendon is either split longitudinally or retracted laterally to expose the periosteum.
- Cortical Windowing: The periosteum is incised and elevated. A high-speed burr or a small osteotome is used to create an oval cortical window over the thinnest portion of the expanded cortex. The window must be large enough to allow complete visualization of the medullary canal.
- Intralesional Curettage: Using a series of small, angled curettes, the gross cartilaginous tumor (which often appears as bluish-white, lobulated, avascular tissue) is meticulously excavated.
- Adjuvant Treatment: To minimize recurrence, the cavity is expanded using a high-speed burr to remove microscopic disease residing in the cortical ridges. Chemical adjuvants, such as 88% phenol followed by absolute alcohol neutralization, or cryotherapy with liquid nitrogen, may be applied to the cavity walls.
- Bone Grafting: The resultant void is tightly packed with cancellous bone graft. Autograft (harvested from the distal radius or iliac crest) provides optimal osteoconductive, osteoinductive, and osteogenic properties. Alternatively, allograft chips or synthetic bone substitutes (e.g., calcium phosphate cement) can be used to avoid donor-site morbidity.
- Closure and Rehabilitation: The periosteal window (if preserved) is laid back, and the soft tissues are closed in layers. The digit is splinted in an intrinsic-plus position. Early active range of motion (ROM) is initiated within 3 to 5 days to prevent extensor tendon adhesions.

Postoperative radiograph following thorough intralesional curettage and dense packing with cancellous bone graft.
BENIGN OSTEOBLASTOMA
Benign osteoblastomas are rare, bone-forming neoplasms. When they do arise, they exhibit a predilection for the axial skeleton, but in the appendicular skeleton, they commonly occur in the small tubular bones of the hands and feet.
Clinical and Radiographic Characteristics
Clinically and histologically, osteoblastomas share significant similarities with osteoid osteomas. Both lesions produce woven bone and osteoid lined by plump osteoblasts. However, critical distinctions dictate their management:
* Size: Osteoblastomas are generally larger than osteoid osteomas (typically >2.0 cm in diameter).
* Symptomatology: Unlike the classic nocturnal, prostaglandin-mediated pain of osteoid osteoma that is dramatically relieved by NSAIDs, osteoblastomas cause a duller, less localized ache that is less responsive to salicylates.
* Radiographic Appearance: Osteoblastomas are highly expansile. They produce gross metacarpal or phalangeal deformities. Radiographically, they exhibit a characteristic "ground-glass" appearance due to the varying degrees of matrix ossification. Despite tremendous expansion, the cortical shell typically remains intact, though it may become paper-thin and cause pressure deformities on adjacent bones.

Expanding intraosseous tumor of the fifth metacarpal exhibiting a ground-glass appearance. Note the intact cortical shell causing pressure deformity on the adjacent fourth metacarpal.
Surgical Management
The biological behavior of osteoblastomas in the hand dictates a more aggressive surgical approach than that used for simple enchondromas.
- Standard Treatment: For well-contained lesions, aggressive intralesional curettage combined with high-speed burring and bone grafting is the standard of care.
- Aggressive/Recurrent Lesions: Osteoblastomas can be locally aggressive. If the lesion has destroyed significant cortical bone or recurred following primary curettage, en bloc excision is required.
- Interpositional Grafting: Following en bloc resection of a metacarpal or phalanx, structural integrity must be restored. A partial-thickness or full-thickness structural autograft (such as a fibular strut graft or iliac crest graft) is interposed.
Surgical Warning: When performing en bloc resection of a metacarpal, meticulous care must be taken to preserve the epiphyseal growth plate (in pediatric patients) and the subchondral cortex of the carpometacarpal joint to maintain longitudinal growth and joint kinematics.

Intraoperative/Postoperative imaging demonstrating a partial-thickness fibular graft interposed after the complete excision of the osteoblastoma. The epiphyseal plate and subchondral cortex have been meticulously preserved.

Long-term follow-up (15 months post-operation) showing complete remodeling of the graft. There is no evidence of tumor recurrence, and the growth plate and carpometacarpal joint have been successfully maintained.
ANEURYSMAL BONE CYST (ABC)
Aneurysmal bone cysts are highly destructive, blood-filled, reactive bone lesions. While they can occur as primary lesions, they frequently arise secondary to other osseous pathologies, including giant cell tumors, chondroblastomas, or osteoblastomas.
Pathology and Presentation
ABCs typically begin as eccentric, ballooning lesions located in the metaphysis of tubular bones (distinct from the epiphyseal location of giant cell tumors). As the lesion progresses, it enlarges to become centrally located, causing severe pain, swelling, and mechanical limitation of motion.
Histologically, ABCs are characterized by cavernous, blood-filled spaces separated by fibrous septa containing osteoclast-like giant cells and reactive woven bone. Crucially, these blood-filled spaces lack an endothelial lining, differentiating them from true vascular neoplasms.
Radiographically, ABCs are almost indistinguishable from giant cell tumors or highly expansile enchondromas. They present as radiolucent, multiloculated ("soap bubble") lesions that cause tremendous cortical expansion, often reducing the cortex to a microscopic, eggshell-thin rim.

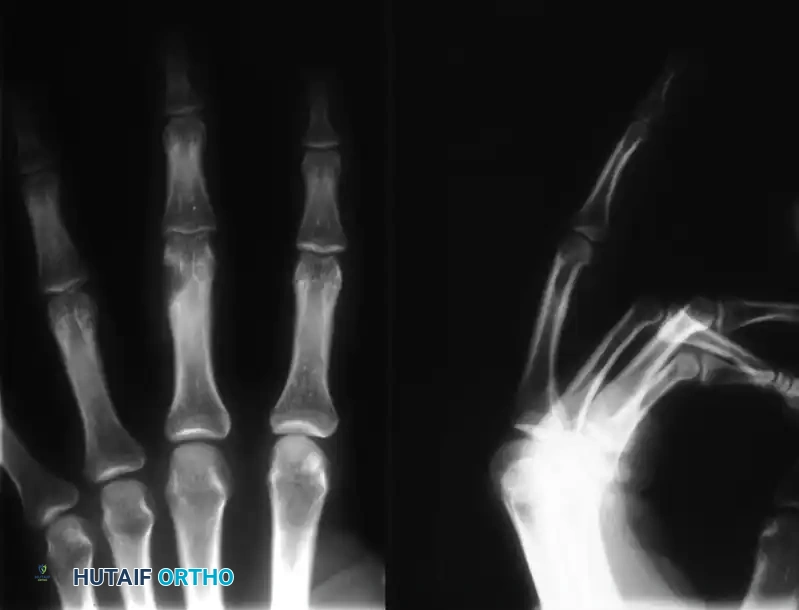
Radiographic presentation of an eccentric, ballooning lytic lesion characteristic of an aneurysmal bone cyst or aggressive osteoid osteoma variant in the proximal phalanx.
Surgical Management
The tremendous cortical expansion and subsequent loss of mechanical stability make the management of ABCs in the hand particularly challenging.
- Inadequacy of Curettage: Simple curettage of an ABC in a small tubular bone carries an unacceptably high recurrence rate and often fails to restore the structural integrity of the severely expanded and thinned bone.
- En Bloc Resection: For tubular bone involvement in the hand, en bloc resection of the affected segment followed by structural autogenous bone grafting is the treatment of choice. This ensures complete eradication of the reactive tissue and provides immediate mechanical stability, allowing for early rehabilitation.
GIANT CELL TUMORS OF BONE (GCT)
Giant cell tumors of bone are uncommon in the hand. When they do occur in the upper extremity, they are most frequently reported in the distal radius. Within the hand itself, the carpal bones (with the hamate being the most common) and the phalanges are the primary sites of involvement.
Biological Behavior and Grading
Despite being classified as histologically benign, GCTs are locally aggressive neoplasms with a high propensity for recurrence and a capacity for massive bone destruction. In the hand, GCTs behave even more aggressively than their counterparts in the long bones.
GCTs are typically graded based on their radiographic appearance and biological activity (Campanacci grading):
* Grade I (Latent): Lesions are well-marginated with an intact cortex.
* Grade II (Active): Cortical margins are thinned and the cortex is expanded, but containment is maintained.
* Grade III (Aggressive): Cortical containment has been lost, resulting in cortical destruction and soft tissue invasion.
Surgical Management and Reconstruction
The aggressive nature of GCTs in the hand necessitates a radical approach to surgical management.
Surgical Pitfall: Generally, simple intralesional curettage and bone grafting are entirely insufficient for the treatment of GCTs in the hand. The recurrence rate following simple curettage approaches 80-90% in tubular bones.
- Resection and Reconstruction: If the cortex is thinned but not completely eroded (Grade II), wide resection of the involved bone segment combined with reconstructive surgery (using structural autograft or allograft) is indicated.
- En Bloc Excision and Ablation: For Grade III lesions demonstrating cortical invasion, destruction, and soft tissue extension—or in cases of aggressive recurrence—en bloc excision with massive allograft reconstruction is required. In severe cases where the neurovascular bundles or flexor/extensor mechanisms are irreparably compromised, ray amputation (ablation of the part) is the most definitive and functional treatment.
- Adjuvant Therapies:
- Cryosurgery: The use of liquid nitrogen as an adjunctive treatment during extended curettage can be highly useful. The extreme cold induces intracellular ice crystal formation and thermal necrosis, extending the oncologic margin by several millimeters into the surrounding bone.
- Radiation Therapy: Radiation therapy is strictly contraindicated for giant cell tumors of bone in the hand. It has proven oncologically ineffective for local control and carries a catastrophic 20% risk of inducing secondary radiation-induced sarcomas (e.g., osteosarcoma or fibrosarcoma) in the irradiated field.
Postoperative Protocol
Following the resection of aggressive benign tumors (osteoblastomas, ABCs, GCTs) and structural grafting, the hand must be immobilized in a thermoplastic splint or cast to protect the graft-host junction. Pin fixation (K-wires) or mini-fragment plates are often utilized to stabilize the reconstruction.
Once radiographic union is evident at the graft interfaces (typically 6 to 8 weeks), aggressive occupational therapy is initiated. The focus shifts to scar desensitization, restoration of the intrinsic muscle balance, and progressive passive and active range of motion to overcome the inevitable stiffness associated with complex hand reconstruction. Regular radiographic surveillance is mandatory for a minimum of 2 to 5 years to monitor for local recurrence.
