Elbow Replacement for Acute Trauma
DEFINITION
Most comminuted elbow fractures have associated soft tissue injuries, which are often of equal or greater importance to the bony injury.The goal when treating acute elbow fractures is that of anatomic open reduction and internal fixation (ORIF) with management of any soft tissue injuries.An acute elbow arthroplasty should be considered only if ORIF is unlikely to achieve a predictably good functional outcome in the older age groups.In the majority of cases, elbow replacements for the treatment of acute fractures should be limited to the physiologically elderly patient with low functional demands.
ANATOMY
The bony anatomy of the elbow consists of the distal humerus, proximal ulna, and proximal radius.Important soft tissue stabilizers include the medial and lateral ligamentous complexes and surrounding musculature, especially the brachialis, common flexor and common extensor masses, and triceps.The ulnar nerve is tethered to the medial condylar-epicondylar fragment by the cubital tunnel retinaculum distally and the arcade of Struthers proximally.
PATHOGENESIS
Elbow injuries are often the result of direct impact—for example, a direct blow on the elbow during a fall. Knowing the energy of the fracture is important to gauge the likelihood of associated injuries.Less energy is required to create a comminuted fracture in elderly and osteoporotic individuals, but muscular injuries of the triceps and brachialis are common, with a subsequent influence on the functional outcome.The ulnar nerve displaces with the medial fragment. As a consequence, the nerve may kink, leading to a local nerve injury. Nerve lacerations are an uncommon consequence of comminuted distal humeral fractures.
NATURAL HISTORY
Most distal humeral fractures are treatable with either nonoperative management or ORIF. Challenging fracture subgroups include fractures that involve articular surfaces and are highly comminuted, although younger patients (younger than 65 years old) are generally not considered candidates for total joint replacements, partialjoint replacements are an emerging solution. 22Many direct and indirect soft tissue complications may ensue, including neurovascular entrapment, 8,12 muscle tears leading to myositis ossificans,12,18,23 and soft tissue contracture with joint stiffness.There is some evidence to suggest that congruently reducing and fixing a comminuted intra-articular distalhumeral fracture does not eliminate the risk of posttraumatic arthritis, 13 although, where possible, ORIF with anatomic congruity should remain the primary goal.
PATIENT HISTORY AND PHYSICAL FINDINGS

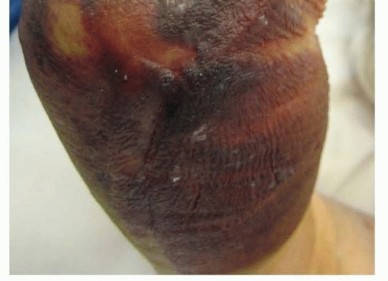
FIG 1 • Typical appearance of an elbow with an underlying fracture with extensive swelling and bruising. Distal radioulnar joint disruption: Ballottement of the ulnar head should be done in the volar and dorsal directions, in pronation and supination. A disrupted joint is often painful with such ballottement, and the ulnarhead may be prominent with the forearm in pronation.Fracture extension beyond the elbow: The examiner should palpate the ulnar shaft, along its subcutaneous border, from the wrist to the olecranon.Interosseous membrane injury: Palpating the interval between the bones of the forearm is not a sensitive examination but can raise suspicion for an Essex-Lopresti injury, leading to further imaging. If an interosseous membrane disruption is present, this will influence the type of implant used for elbow replacement (one with a radial head replacement), but the pathology is not commonly described.
IMAGING AND DIAGNOSTIC STUDIES
Plain radiographs, including anteroposterior (AP) and lateral views ( FIG 2) of the elbow and both wrists, should be obtained. The elbow view may have to be taken in a protective splint or plaster backslab for patient comfort.Elbow radiographs will allow initial assessment of the degree of comminution and may indicate the presence of decreased bone mineral density.Bilateral wrist views will indicate the presence of an axial (interosseous membrane) injury if the ulnar head is in positive variance compared to the contralateral uninjured wrist.Plain tomograms are of use in improving the understanding of the fracture configuration, but an alternative would be a computed tomography (CT) scan. With the latter, the surgeon can view a three-dimensional reconstruction, which is a useful surgical planning tool for ORIF.If there is evidence on physical examination of a neurologic injury, it is prudent to document its extent with a carefully performed neurologic examination.
DIFFERENTIAL DIAGNOSIS

FIG 2 • Standard AP (A) and lateral (B) plain radiographs.
NONOPERATIVE MANAGEMENT
The “bag-of-bones” technique is a nonoperative method of treatment described by Eastwood 7 that encourages the compressive molding of the comminuted distal humeral fracture fragments.Subsequent rehabilitation with collar and cuff support achieves substandard but acceptable results only in the elderly and debilitated group of patients who have almost no demand on elbow function.This type of treatment does not achieve acceptable results with respect to stability and strength in younger patients.
SURGICAL MANAGEMENT
OPEN REDUCTION AND INTERNAL FIXATION
ORIF has been widely documented for comminuted fractures of the distal humerus.Some reported series demonstrate good results with fixation of such challenging fractures, with better results predominantly in the younger age groups. 19,24 Rarely are good results achieved in the elderly, osteoporotic group.13Many series report less than satisfactory outcomes in the elderly treated by operative fixation. 19A direct comparison of internal fixation to primary total elbow replacement in the elderly osteoporotic group revealed that replacement produced no poor results and no need for revision surgery at 2 years of follow-up.The internal fixation group produced three poor results requiring revision to a total elbow replacement. 10
ELBOW ARTHROPLASTY



FIG 3 • A. Patient positioned in a supine position. The elbow is isolated and placed on a roll of towel placed on the patient's chest and stabilized by an assistant. The surgeon must take care to avoid the neck and anesthetic equipment. B. Patient positioned in a lateral decubitus position with the elbow draped over an arm support. P.153Surgical ApproachTwo main surgical approaches are useful for acute total elbow arthroplasty:“Triceps on” (eg, Alonso-Llames, paratricipetal) “Triceps off” (eg, Bryan-Morrey)The triceps should be carefully managed in either approach, and it often has a thin tendon, especially in older patients and those with rheumatoid arthritis. The triceps tendon should be dissected from the olecranon with a small curved scalpel blade, maintained perpendicular to the interface between the tendon and bone.
TECHNIQUES
INCISION AND DISSECTION




TRICEPS ON (TRICEPS PRESERVING)




TECH FIG 2 • A. A periosteal elevator is introduced between the triceps and the humeral shaft, and the two structures are separated by sliding the elevator proximally and then distally to the level of the triceps insertion. B. The lateral corridor is defined, and lateral fragments are removed. From the lateral margin of the humeral shaft, raise the brachialis from 2 to 3 cm of the anterior surface.An alternative approach when considering a hemiarthroplasty is ulnar osteotomy and triceps reflection. This is relatively a simple exposure, but the osteotomy will need to be fixed with a plate and screw construct.
MODIFIED BRYAN-MORREY APPROACH


TECH FIG 3 • A. The triceps is split through its central tendon in line with the fibers. The tendinous portion is dissected from the olecranon to gain access to the ulna. B,C. To dissect the Sharpey fibers off the ulna, the surgeon uses the scalpel parallel to the ulna surface and maintains the release directly adjacent to the bone.(continued)
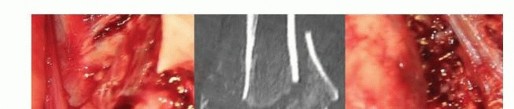
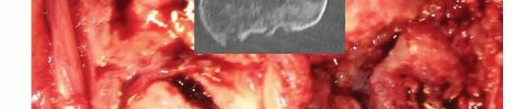

TECH FIG 3 •(continued)D. Comminuted distal humeral fracture in an osteoporotic elderly woman, with CT imaging confirming significant articular comminution. This is the view through the triceps split.

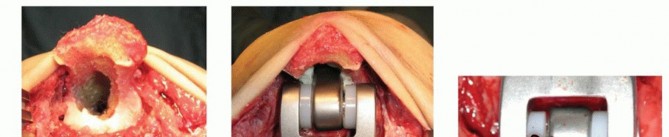
TECH FIG 4 • A. The humeral component entry point, the apex of the olecranon fossa, is identified, and humeral canal preparation is commenced by opening the canal with a bone nibbler or burr.(continued)
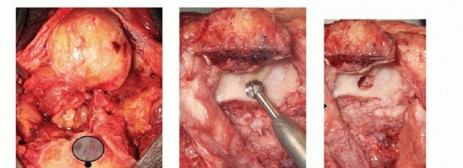
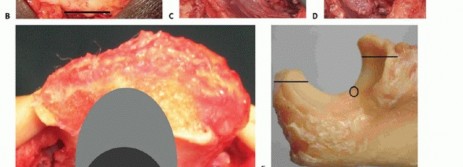

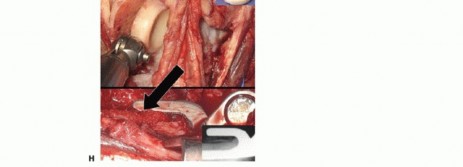



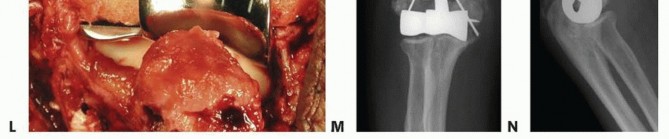
TECH FIG 4 •(continued)I-K. Latitude DHH. I. Intact medial and lateral humeral columns, with a red vessel loop loosely around the ulna nerve. J. AP radiograph demonstrating the trochlea and capitellum correctly sized for the host, greater sigmoid notch of the ulna, and the radial head. K. Lateral radiograph demonstrating a well-aligned radio capitellar joint and osseous integration of the anterior flange. L-N. Sorbie DHH. L. Fractured medial and lateral columns were reconstructed with K-wires, prior to implant insertion. M. AP radiograph demonstrating a well-seated Sorbie implant with healed medial and lateral columns. N. Lateral radiograph demonstrating a well-aligned radiocapitellar joint with posterior heterotopic ossification in the traumatically injured triceps muscle.
Implant Insertion and Soft Tissue Tensioning

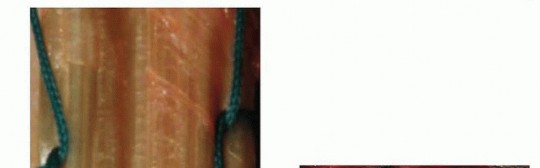

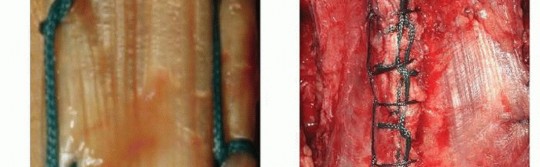
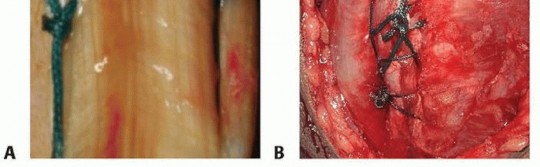
TECH FIG 6 • A,B. A running locking stitch is used to improve triceps purchase when reattaching the muscle to the ulna. A. An example of a running locking stitch on either side of the split tendon. B. A locking stitch that locks both sides of the split together with one continuous locking suture. It is then reinforced with a reversed across-split locking suture.(continued)
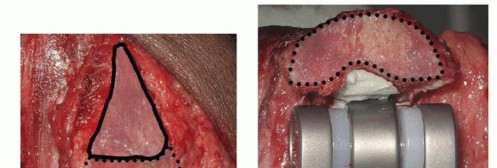
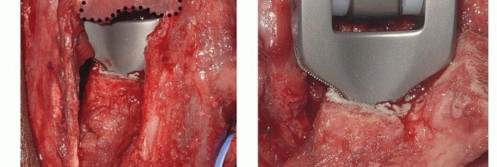
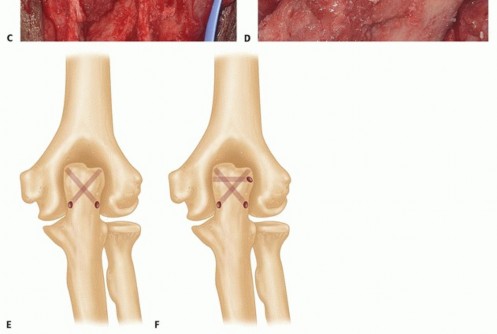
TECH FIG 6 •(continued)C,D. The triceps footprint to which reattachment should be attempted is predominantly on the flat part of the ulna or olecranon process, and not the tip, which is resected to prevent posterior abutment. E. Drill holes (1.5 to 2 mm) are oriented in a crossing fashion to secure the triceps to the footprint area. F. A separate cinch suture is used to increase the security and the area of contact between the triceps and the ulna, thereby improving healing potential.
Wound Closure
The ulnar nerve is transposed into an anterior subcutaneous location.
Reapproximate the flexor-pronator and common extensor masses to the triceps with absorbable suture. Do not overtighten this repair, as it will restrict motion.
The use of a subcutaneous drain is a matter of surgeon preference. However, there is no literature demonstrating the efficacy of a postoperative drain in preventing hematoma.
P.160
WOUND CLOSURE
PEARLS AND PITFALLS
Indications ▪ A complete history and physical examination should be performed, with specific questions about any bone mineral density problems and healing tendency.1.Care must be taken to address associated pathology at the elbow, wrist, and shoulder.Planning ▪ The surgeon should consider fracture osteosynthesis when the patient has adequate bone stock and places high demand on the elbow.2.Arthroplasty should be available in the physiologically older and lower demand patient, with a view to converting to an acute arthroplasty if osteosynthesis is not possible intraoperatively.Exposure ▪ Initial definition and protection of the ulnar nerve are important. Careful dissection of the nerve from the cubital tunnel restraints will allow freedom to move the nerve without risking traction injury during the remainder of the procedure.3.If the exposure involves removing the triceps from its ulnar attachment (Bryan-Morrey approach), the site of Sharpey fiber attachment should be marked and reattached anatomically.4.During a triceps sparing approach, the tendon attachment to the olecranon must be carefully preserved.Inspection ▪ A thorough inspection of the ulna and radial articular surface should be performed to investigate the possibility of a hemiarthroplasty replacement in the appropriately selected younger patient.5.The surgeon should observe the state of the ulnar nerve and muscles around the elbow (especially triceps and brachialis); this will help to explain altered nerve function in the former and weakness and possible myositis ossificans and stiffness in the latter.Bone preparation1.If the humeral columns are intact, then an attempt at preservation should be made, with their extensor and flexor mass attachments, during a total elbow replacement.Implantation ▪ When planning length and implantation, the surgeon should pay careful attention to the tension of the brachialis and triceps. These muscles need appropriate tension to function well, but if overtensioned, the elbow will be stiff, and if undertensioned, the elbow will be weak.1.Hemiarthroplasty—plan to use an implant that is appropriate for the patient, for example, if younger and more active, may need to convert to a total replacement in the future, hence a “convertible” implant is an option.2.Hemiarthroplasty—avoid over- or understuffing or over- or undersizing the joint, with fluoroscopic examination after trial implantation.3.When an ulna osteotomy approach is chosen for DHH, prior to performing the osteotomy, place the plate onto the ulna, and predrill the screws. This saves time at the end of the case.|Wound ▪ Drains should be used at the discretion of the surgeon. If a drain is not used, the closure surgeon should pay close attention to hemostasis, and for the first 12 hours, amoderately tight bandage should be used to avoid hematoma formation. The dressing is removed on postoperative day 2.Rehabilitation ▪ With triceps reattachment, the surgeon should be cautious to avoid overzealous rehabilitation for fear of compromising triceps healing, with subsequent avulsions or extension weakness.|------
POSTOPERATIVE CARE
A volar plaster or thermoplastic splint is used to maintain the elbow in full extension for the first 24 to 48 hours. This avoids tension on the incision and on the triceps reattachment.The arm is elevated on pillows or with a Bradford sling overnight to prevent edema.Nonsteroidal anti-inflammatories are avoided because of their detrimental effects on tissue healing (bone to tendon and bone to bone). This is especially important when relying on ligamentous healing for a hemiarthroplasty.On the second day after surgery, the dressing is removed and the compliant patient should commence gentle active antigravity flexion, with passive gravity-assisted extension.A resting molded orthoplast splint with the elbow placed at 90 degrees of flexion is made to protect the triceps repair and wound.Graduated and targeted motion is prescribed, with greater than 90 degrees of elbow flexion attempted after 5 weeks. This allows sufficient time for the triceps to adhere and heal to the ulna. Aggressive flexion too early may result in triceps avulsion or pull-out. Triceps antigravity exercises can commence after 5 weeks.Always, at each patient interaction, the surgeon should reiterate the restrictions of use with an elbow arthroplasty: limited internal (varus) and external (valgus) rotatory torques, 2-pound repetitive and 10-pound single-event lifting.Postoperative care for a hemiarthroplasty varies from a total replacement. In stable constructs, active-assisted motion is begun immediately, and passive motion is avoided. Individuals with operative columnar fixation require additional immobilization for 2 weeks in a splint at night and intermittently during the day with the arm flexed at 90 degrees. At 6 weeks, patients are instructed to begin light elbow strengthening exercises.
COMPLICATIONS
Triceps avulsion StiffnessOverlengthened implantation Overtensioned triceps reattachmentOverzealous closure of triceps to flexor-extensor compartments Inadequate soft tissue releaseP.161ImpingementRadial head on humeral component (distal yolk) Coronoid on humeral component (anterior yolk) Olecranon process on posterior humerusDeep venous thrombosis InfectionPeriprosthetic fracture Osteoporotic boneStem-canal mismatched sizesStem-canal mismatched curvatureInadequate opening for ulnar component at coronoid base Ulnar nerve neuropathy or injury
OUTCOMES
TOTAL ELBOW ARTHROPLASTY
Cobb and Morrey 6 reported 15 excellent and 5 good results, with one patient with inadequate data, in a cohort of patients with acute distal humeral fractures (average age of 72 years) at 3.3 years of follow-up.Ray et al 21 reported 5 excellent and 2 good functional results in a group of patients with an average age of 81 years at 2 to 4 years of follow-up.Gambirasio et al 11 reported excellent functional results in a cohort of 10 elderly patients with osteoporotic intraarticular fractures.Frankle et al 10 compared the outcomes of patients older than age 65 years with comminuted intra-articular distal humeral fractures treated with ORIF versus acute total elbow replacements. The ORIF group had 8 excellent results, 12 good results, 1 fair result, and 3 poor results, with 3 patients requiring conversion to elbow replacement. All 12 acute primary elbow replacements achieved excellent (n = 11) or good (n = 1) results.Kamineni and Morrey 15 reported an average Mayo Elbow Performance Score (MEPS) of 93/100 in a series of 49 acute distal humeral fractures (average patient age of 67 years) at 7 years of follow-up. The average arc of motion was 107 degrees.Lee et al 17 reported seven acute elbow replacements for distal humeral fractures in patients with an average age of 73 years. The average arc of motion was 89 degrees and the average MEPS was 94/100 at an average follow-up of 25 months.Abbas et al 1 reported 23 elbow replacements for complex and intra-articular fractures in patients with an average age of 75 years. MEPS was 93/100 with an average flexion arc of 93 degrees, at an average follow-up of 6 years.
DISTAL HUMERAL HEMIARTHROPLASTY
Smith and Hughes 22 have reported a large series of 26 patients (mean age of 62 years; range 29 to 92 years). Four patients required conversion to total joint replacement.Hughes et al 14 reviewed the early results and proposed a treatment algorithm incorporating the use of this technique in the overall management of distal humeral fractures.DHH was performed on 30 patients (mean age of 65 years; range 29 to 91 years) for unreconstructable fractures of the distal humerus or salvage of failed internal fixation.A triceps on approach was used in 6 patients and an olecranon osteotomy in 24 patients. A Sorbie Questor prosthesis (Wright Medical Technology, Arlington, TN) was used in 14 patients and a Latitude (Tornier Inc., Minneapolis, MN) in 16 patients.Clinical review at a mean of 25 months (range 3 to 88 months) included the American Shoulder and Elbow Surgeons (ASES) elbow outcomes instrument, Mayo Elbow Performance Index (MEPI), and radiologic assessment.At follow-up of 28 patients, mean flexion deformity was 25 degrees, flexion 128 degrees, range of prosupination 165 degrees, mean ASES 83, MEPI 77, and satisfaction 8/10. Acute cases scored better than salvage cases. Reoperation was required in 16 patients (53%); two revisions to a linked prosthesis for periprosthetic fracture and aseptic loosening at 16 and 53 months, 12 metalwork removals and four ulnar nerve procedures.This is the largest reported experience of DHH. Early results of DHH show good outcomes after complex DHH, despite a technically demanding procedure. This series had metalware removal in 40%, symptomatic laxity in 12%, and column nonunion in 8%. Better results are obtained for treatment in the acute setting and with use of an olecranon osteotomy.Burkhart et al 5 reported on 9 good or excellent results and 1 “fair” result in a cohort of 10 females (average age of 75 years; acute hemiarthroplasty, n = 8; and hemiarthroplasty after failed osteosynthesis, n = 2), with a 12-month follow-up. The average range of motion was 17 degrees of extension deficit to 124 degrees of flexion, with 80 degrees of prosupination. No complications requiring revision surgery were reported.Adolfsson and Nestorson 3 reported eight excellent or good results, according to the Mayo elbow performance score, in eight females, average age of 79 years. The mean follow-up was 4 years, arc of motion was 31 degrees extension deficit to 126 degrees of flexion. Radiographic attrition of the ulna was observed, and one periprosthetic fracture at 3 years was reported.Argintar et al 4 reviewed the Tornier Latitude elbow hemiarthroplasty retrospectively in a small series of 10 patients and reported good to excellent results in short-term clinical outcomes. Unlike other hemiarthroplasty systems, the Latitude system is versatile with several stem lengths, a flange, and, perhaps most importantly, is convertible to a linked or unlinked total elbow arthroplasty.The Kudo prosthesis has shown good short-term clinical success. Adolfsson and Hammer 2 retrospectively reviewed four distal humerus hemiarthroplasties; with an average follow-up of 10 months, average extension was 20 degrees, flexion was 126 degrees, and pronation and supination were each 78 degrees. Three patients were deemed to have an excellent outcome and one patient had a good outcome, with theMayo score. A longer term study by Adolfsson and Nestorson, 3 4.5-year follow-up, eight patients who underwent distal humerus hemiarthroplasty demonstrated mean elbow motion arcs from 31 to 126 degrees. Of this group, five patients had an excellent outcome and three patients had a good outcome.
CONCLUSIONS
Total elbow arthroplasty, in the setting of an acute unreconstructable distal humeral fracture, is a reliable option that provides pain relief and function compatible with a low-demand individual. The DHH has a potential niche in the younger, more active patient, but with limited experience, its use should be carefullyconsidered.
REFERENCES
P.1621.Abbas GA, Chutter GSJ, Williams JR. Retrospective review of primary total elbow replacement (TER) for osteoporotic fractures of distal humerus in the elderly over 10-year period. Injury Extra 2010;41:160.2.Adolfsson L, Hammer R. Elbow hemiarthroplasty for acute reconstruction of intraarticular distal humerus fractures: a preliminary report involving 4 patients. Acta Orthop 2006;77:785-787.3.Adolfsson L, Nestorson J. The Kudo humeral component as primary hemiarthroplasty in distal humeral fractures. J Shoulder Elbow Surg 2012;21:451-455.4.Argintar E, Berry M, Narvy SJ, et al. Hemiarthroplasty for the treatment of distal humerus fractures: short-term clinical results. Orthopedics 2012;35:1042-1045.5.Burkhart KJ, Nijs S, Mattyasovszky SG, et al. Distal humerus hemiarthroplasty of the elbow for comminuted distal humeral fractures in the elderly patient. J Trauma 2011;71:635-642.6.Cobb TK, Morrey BF. Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.7.Eastwood WJ. The T-shaped fracture of the lower end of the humerus. J Bone Joint Surg 1937;19:364-3698.Faierman E, Wang J, Jupiter JB. Secondary ulnar nerve palsy in adults after elbow trauma: a report of two cases. J Hand Surg Am 2001;26:675-678.9.Frankle MA, Herscovici D Jr, DiPasquale TG, et al. A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular fractures of the distal humerus in women older than 65 years. J Shoulder Elbow Surg 1999;9:455.10.Frankle MA, Herscovici D Jr, DiPasquale TG, et al. A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than age 65. J Orthop Trauma 2003;17:473-480.11.Gambirasio R, Riand N, Stern R, et al. Total elbow replacement for complex fractures of the distal humerus. An option for the elderly patient. J Bone Joint Surg Br 2001;83:974-978.12.Holmes JC, Skolnick MD, Hall JE. Untreated median-nerve entrapment in bone after fracture of the distal end of the humerus: post-mortem findings after forty-seven years. J Bone Joint Surg Am 1979;61:309-310.13.Huang TL, Chiu FY, Chuang TY, et al. The results of open reduction and internal fixation in elderly patients with severe fractures of the distal humerus: a critical analysis of the results. J Trauma 2005;58: 62-69.14.Hughes J, Malone AA, Zarkadas P, et al. Distal humeral hemiarthroplasty (DHH) for intra-articular distal humeral fractures. J Bone Joint Surg Br 2012;94-B:162.15.Kamineni S, Morrey BF. Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86-A(5):940-947.16.Kamineni S, Morrey BF. Distal humeral fractures treated with noncustom total elbow replacement. Surgical technique. J Bone Joint Surg Am 2005;87(suppl 1):41-50.17.Lee KT, Lai CH, Singh S. Results of total elbow arthroplasty in the treatment of distal humerus fractures in elderly Asian patients. J Trauma 2006;61:889-892.18.Mohan K. Myositis ossificans traumatica of the elbow. Int Surg 1972;57:475-478.19.Pajarinen J, Bjorkenheim JM. Operative treatment of type C intercondylar fractures of the distal humerus: results after a mean follow-up of 2 years in a series of 18 patients. J Shoulder Elbow Surg 2002;11: 48-52.20.Parsons M, O'Brien R, Hughes J. Elbow hemiarthroplasty for acute and salvage reconstruction of intraarticular distal humerus fractures. Tech Shoulder Elbow Surg 2005;6:87-97.21.Ray PS, Kakarlapudi K, Rajsekhar C, et al. Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. Injury 2000;31:687-692.22.Smith GC, Hughes JS. Unreconstructable acute distal humeral fractures and their sequelae treated with distal humeral hemiarthroplasty: a two-year to eleven-year. J Shoulder Elbow Surg 2013;22:1710-1723.23.Thompson HC III, Garcia A. Myositis ossificans: aftermath of elbow injuries. Clin Orthop Relat Res 1967;50:129-134.24.Zhao J, Wang X, Zhang Q. Surgical treatment of comminuted intraarticular fractures of the distal humerus with double tension band osteosynthesis. Orthopedics 2000;23:449-452.
