ARTHROSCOPIC MANAGEMENT OF ELBOW LOOSE BODIES
The removal of intra-articular loose bodies remains the most common and highly successful indication for elbow arthroscopy. Patients typically present with a constellation of mechanical symptoms, including persistent pain, catching, locking, and a mechanically blocked or limited range of motion (ROM). When these symptoms are recalcitrant to conservative management, a thorough diagnostic and therapeutic arthroscopic examination is strictly indicated.
Pathoanatomy and Etiology
Understanding the origin of loose bodies is critical for comprehensive joint management. In addition to locating and extracting the loose body, the operating surgeon must identify and address the site of origin to prevent recurrence and mitigate progressive joint degeneration.
Osteocartilaginous loose bodies most frequently arise from:
* Osteochondritic Lesions: Particularly osteochondritis dissecans (OCD) of the capitellum.
* Osteochondral Fractures: Often resulting from acute lateral compression injuries or shear forces.
* Synovial Pathologies: Such as primary or secondary synovial chondromatosis, which can generate dozens of cartilaginous nodules.
Loose bodies exhibit a propensity to migrate and embed within the capsular recesses. They are frequently sequestered in the fibrous tissue of the coronoid, radial, or olecranon fossae. Furthermore, small loose bodies may hide within the tight confines of the olecranon-trochlear articulation or the radiocapitellar articulation. Failure to systematically probe these hidden recesses during arthroscopy will result in retained fragments and persistent postoperative symptoms.
Diagnostic Imaging
Standard radiographic evaluation is the first line of diagnosis but possesses significant limitations regarding sensitivity. According to seminal data by Andrews and Carson, only approximately 38% of loose bodies are obvious on standard plain radiographs.

Figure 52-64 A: Lateral radiograph of the elbow demonstrating a large anterior loose body and an associated defect of the radial head.

Figure 52-64 B: Anteroposterior (AP) radiograph revealing a large loose body lodged within the coronoid fossa.
To enhance diagnostic accuracy, Computed Tomography (CT) arthrography is highly recommended, as it detects up to 72% of loose bodies, providing precise localization and characterizing the size of the fragments. Magnetic Resonance Imaging (MRI) is also invaluable, particularly for identifying purely cartilaginous bodies and evaluating the integrity of the articular surfaces.
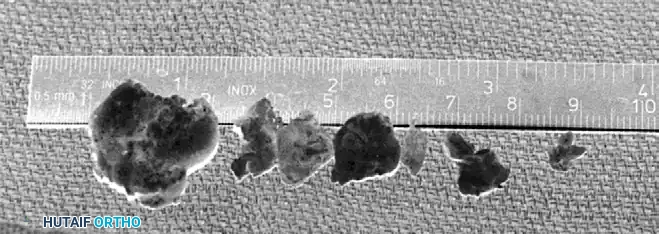
Figure 52-64 C: Postoperative radiograph following the successful removal of loose bodies and resection of the radial head defect.

Figure 52-64 D: Additional postoperative imaging confirming complete clearance of the anterior and posterior compartments.
Surgical Technique: Step-by-Step Retrieval
Elbow arthroscopy for loose body removal demands meticulous portal placement and fluid management to avoid neurovascular compromise.
Surgical Warning: The elbow capsule has a limited volume (typically 15-25 mL). Excessive fluid extravasation can lead to compartment syndrome or neuropraxia. Maintain low pump pressures and utilize gravity flow when possible.
- Diagnostic Round: Begin with a standard proximal anteromedial portal to view the anterior compartment, followed by an anterolateral portal for instrumentation.
- Soft Tissue Release: Loose bodies embedded in the coronoid or radial fossae often require the release of overlying fibrous tissue. Utilize an arthroscopic shaver or arthroscopic scissors to carefully free these bodies from the synovium.
- Fragment Manipulation: When large bodies are located in difficult-to-reach sites, they must be mobilized to a more accessible area.
- The Uncoupling Technique: Uncouple the arthroscope from its sheath, retract the scope a few millimeters, and use the blunt edge of the sheath to physically push the loose body into a favorable position.
- Fluid Management: If fluid turbulence causes the loose body to float away from the grasper (the "snow globe effect"), reduce or completely turn off the inflow to allow the fragment to settle.
- Extraction Strategies:
- Small Fragments: Removed via standard arthroscopic graspers through the working cannula.
- Large Fragments: Occasionally, loose bodies are too large to be extracted through a standard arthroscopic portal. These can be fragmented using an arthroscopic burr and removed piecemeal.
- Kocher Clamp Technique: Alternatively, large bodies can be left in place until the conclusion of the intra-articular work. They are then removed by longitudinally extending the capsular incision and extracting the intact fragment with a Kocher clamp. This delayed extraction prevents premature fluid extravasation into the anterior soft tissues, thereby decreasing the risk of neurovascular compromise during the remainder of the procedure.

Figure 52-65 A: Arthroscopic view of a large, obstructing loose body situated in the anterior elbow compartment.

Figure 52-65 B: The anterior compartment visualized after successful extraction, demonstrating a decompressed and clear joint space.
If a second operative portal is required for the posterior compartment, establish a straight posterior or posterolateral portal under direct arthroscopic visualization to clear the olecranon fossa.
Postoperative Care and Rehabilitation
Rehabilitation must begin immediately to prevent arthrofibrosis, a common complication following elbow trauma and surgery.
* Immediate Phase (Days 1-7): The patient is encouraged to move the elbow within the confines of the postoperative bulky dressing as soon as pain and swelling permit.
* Intermediate Phase (Weeks 2-6): Formal physical therapy focuses on active and active-assisted ROM. Flexibility and progressive strengthening exercises are initiated once joint effusion and acute pain are sufficiently diminished.
PANNER DISEASE AND OSTEOCHONDRITIS DISSECANS
While both Panner disease and Osteochondritis Dissecans (OCD) affect the capitellum, they are distinct clinical entities separated by patient age, pathophysiology, and long-term prognosis.
Panner Disease
Panner disease is an idiopathic osteochondrosis characterized by diffuse involvement of the capitellum.
* Demographics: It almost exclusively occurs in pediatric patients aged 6 to 8 years.
* Pathophysiology: It involves a temporary disruption of the blood supply to the growing capitellum, leading to necrosis and subsequent regeneration.
* Management: The disease is entirely self-limiting. With conservative treatment—consisting of rest, activity modification, and symptomatic management—the capitellum remodels completely, and residual joint problems are exceedingly rare.
Osteochondritis Dissecans (OCD) of the Capitellum
In contrast to Panner disease, OCD develops in a more localized area of the capitellum in preadolescents or adolescents (typically 10 to 17 years old). At this age, the capitellum is closer to skeletal maturity, possesses a diminishing blood supply, and has significantly less potential for spontaneous healing and remodeling.
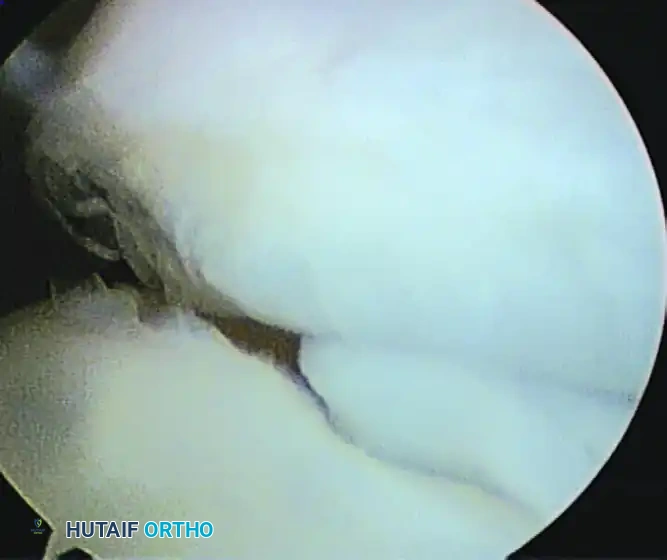
Figure 52-66: Arthroscopic visualization of a partially detached osteochondritis dissecans (OCD) lesion of the capitellum, demonstrating articular cartilage fissuring and instability.
Biomechanics and Etiology
OCD is heavily correlated with activities that subject the radiocapitellar joint to repetitive compression and shear forces. It is a hallmark injury of "valgus extension overload" seen in overhead athletes.
* High-Risk Activities: Baseball pitching, gymnastics, racquet sports, and heavy weightlifting.
* Mechanism: During the late cocking and early acceleration phases of throwing, immense valgus torque is placed on the elbow. This causes medial tension (stressing the ulnar collateral ligament) and lateral compression, driving the radial head forcefully into the capitellum. Over time, this repetitive microtrauma leads to focal subchondral bone ischemia, fragmentation, and eventual cartilage detachment.
Clinical Evaluation
Patients typically present with insidious onset, lateral-sided elbow pain that is exacerbated by repetitive loading activities.
* Physical Examination: Point tenderness is usually elicited directly over the radiocapitellar joint and the capitellum.
* Provocative Testing:
* Active Compression Test: Performed by resisting elbow extension while the patient actively pronates and supinates with a clenched fist.
* Radial Shear Test (O’Driscoll): Valgus stress is applied during passive flexion and extension of the elbow, producing lateral-sided pain or a mechanical grinding sensation.
* Moving Valgus Stress Test: Essential to evaluate for concomitant Ulnar Collateral Ligament (UCL) insufficiency, which often coexists with lateral compressive pathology.
* Prognostic Indicators: According to Takahara et al., the presence of a persistent joint effusion and a loss of elbow extension greater than 20 degrees are poor prognostic signs indicating advanced disease.
Advanced Imaging and MRI Criteria
Radiographic examination of the adolescent elbow must include an AP view, a lateral view, and an AP view with the elbow in 45 degrees of flexion to profile the posterior aspect of the capitellum. Comparison views of the contralateral elbow are highly recommended to evaluate subtle articular surface changes.
MRI is the definitive imaging modality of choice to determine the treatment course, assess cartilage viability, and evaluate persistent pain unexplained by plain radiographs.
Clinical Pearl: MRI Signs of Instability
Kijowski and DeSmet outlined four critical MRI findings that dictate an unstable OCD lesion requiring surgical intervention:
1. A line of high-signal intensity deep to the fragment on T2-weighted images (indicating fluid interposition).
2. An articular fracture indicated by high-signal intensity passing through the subchondral bone plate.
3. A focal osteochondral defect (empty crater).
4. A fluid-filled cyst measuring 5 mm or greater deep to the lesion.
Classification and Grading Systems
Surgical decision-making relies heavily on accurate grading of the lesion.
Arthroscopic Grading (Baumgarten, Andrews, and Satterwhite):
* Grade 1: Articular cartilage softening (chondromalacia).
* Grade 2: Fraying or fissuring, but the cartilage cap remains intact.
* Grade 3: Disruption of the articular cartilage with a definable fragment.
* Grade 4: A detached fragment that remains within the crater.
* Grade 5: A completely displaced lesion (loose body).
International Cartilage Repair Society (ICRS) Grading:
* Grade 1: Intact, stable cartilage.
* Grade 2: Partially detached lesion.
* Grade 3: Completely detached lesion, but remaining within the crater.
* Grade 4: Displaced fragment from the crater.
Surgical Decision Making: Stable vs. Unstable Lesions
When determining the algorithm for conservative versus surgical intervention, lesions are broadly divided into stable and unstable categories, as validated by Takahara et al. in a comprehensive study of 106 patients.
- Stable Lesions (Conservative Management): These lesions have a high propensity for complete healing. They present with an open capitellar growth plate, localized flattening or radiolucency of the subchondral bone without fluid interposition on MRI, and well-preserved elbow motion. Treatment involves strict cessation of the offending activity for 3 to 6 months.
- Unstable Lesions (Surgical Management): Surgery provides superior outcomes for lesions exhibiting any of the following: a closed capitellar growth plate, radiographic fragmentation, MRI signs of instability, or restricted elbow motion of 20 degrees or more.
Arthroscopic Interventions and Prognostic Factors
During arthroscopic evaluation, the size, containment, and radial head engagement of the lesion are the most critical prognostic factors dictating the specific surgical technique.
According to Ahmad et al., poor prognostic factors include:
1. Capitellar defects encompassing more than 50% of the articular surface.
2. Loss of lateral buttress containment exceeding 6 to 7 mm.
3. Engagement of the radial head into the defect.
Evaluating Engagement: To assess radial head engagement, the surgeon places the elbow in extension, pronates and supinates the forearm, and then ranges the elbow through a full arc of motion under direct arthroscopic visualization. If the radial head drops into the capitellar defect after initial debridement, the biomechanics of the joint are severely compromised.
Surgical Options:
1. Debridement and Microfracture: For smaller, contained lesions (<50% involvement) without radial head engagement. The unstable fragment is excised, the sclerotic base is debrided to bleeding subchondral bone, and microfracture awls are used to penetrate the subchondral plate, stimulating a marrow-stimulating healing response (fibrocartilage formation).
2. Fragment Fixation: Attempted if the fragment is large, acute, and possesses sufficient attached subchondral bone to allow for healing. However, follow-up studies show variable success, as most fragments exhibit advanced chondral degeneration or lack adequate bone stock for secure screw or dart fixation.
3. Osteochondral Autograft Transfer System (OATS): Strictly indicated for large lesions (>50% involvement), lesions with a loss of lateral containment, or those demonstrating radial head engagement. Transferring a cylindrical osteochondral plug (typically harvested from the non-weight-bearing periphery of the ipsilateral knee) restores the articular congruity and lateral buttress, preventing progressive degenerative joint changes and allowing the athlete to return to high-demand activities.
