ELBOW DISLOCATIONS: EPIDEMIOLOGY AND BIOMECHANICS
The elbow is the second most common major joint dislocated in the adult population, superseded only by the glenohumeral joint. Approximately 20% of these dislocations are complex, presenting with concomitant fractures of the radial head, coronoid process, or olecranon. The inherent stability of the elbow relies on a highly congruent osseous articulation (the ulnohumeral joint) and a robust soft-tissue envelope, primarily the medial ulnar collateral ligament (MUCL) and the lateral collateral ligament (LCL) complex.
Acute simple dislocations of the elbow are almost universally reducible via closed methods. Following reduction, the majority of these joints demonstrate adequate stability through a functional arc of motion. Late elbow instability and chronic stiffness are exceedingly rare following simple dislocations, provided that appropriate rehabilitation protocols are instituted.
Principles of Management in Simple Dislocations
The foundational treatment principles for simple elbow dislocations dictate concentric reduction of the joint followed by early, protected motion. Prolonged immobilization is historically associated with severe, recalcitrant arthrofibrosis.
Clinical Pearl: Immobilization of a simple elbow dislocation should rarely exceed 2 to 3 weeks. The primary complication of simple dislocations is stiffness, not recurrent instability.
Josefsson et al. conducted landmark comparative studies evaluating the operative versus nonoperative treatment of ligamentous injuries occurring in the setting of simple elbow dislocations. Their findings demonstrated that although all patients exhibited gross instability under anesthesia post-reduction, those treated nonoperatively ultimately reported fewer symptoms and achieved superior functional outcomes compared to those subjected to primary ligamentous repair.
Immobilization typically ranges from 2 to 4 weeks, strictly dictated by the degree of residual instability. Mehlhoff et al., in a comprehensive review of 52 patients treated nonoperatively, strongly recommended that unprotected flexion and extension exercises be initiated within 2 weeks of the dislocation to optimize outcomes. Conversely, in high-demand throwing athletes, where valgus stability is paramount, Burra and Andrews have advocated for acute operative repair of the MUCL to restore elite-level kinematics.
DISLOCATION OF THE RADIAL HEAD
Isolated dislocations of the radial head—occurring without simultaneous dislocation of the humeroulnar joint—are relatively uncommon but biomechanically significant. When this occurs, the radial head is almost exclusively displaced anteriorly. While closed reduction is often easily achieved manually, maintaining this reduction can be challenging.
The pathoanatomy involves the rupture or severe displacement of the annular ligament. Consequently, the unopposed pull of the biceps brachii muscle acts as a potent deforming force, frequently causing the dislocation to recur. If the radial head remains subluxated or dislocated, it creates a mechanical block, severely limiting terminal flexion of the elbow joint.
Indications for Operative Intervention
Open reduction and primary repair, or formal reconstruction of the annular ligament, are strictly indicated under the following clinical scenarios:
1. Recurrent Instability: When the dislocation recurs despite closed reduction and immobilization of the elbow in greater than 90 degrees of flexion.
2. Delayed Presentation: When the injury has gone unrecognized or untreated for 2 to 4 weeks.
3. Irreducibility: When closed reduction is blocked, most commonly due to the interposition of the torn annular ligament or anterior capsule into the radiocapitellar joint.
Surgical Warning: If an isolated radial head dislocation has gone untreated for more than 4 to 5 weeks in an adult, the articular cartilage is often irreparably damaged, and the soft tissues are severely contracted. In these delayed cases, radial head excision or prosthetic arthroplasty is indicated rather than attempted ligamentous reconstruction.
(Note: The treatment of a radial head dislocation associated with a fracture of the proximal third of the ulna—the classic Monteggia fracture-dislocation—requires rigid internal fixation of the ulna to restore length and alignment, which typically reduces the radial head indirectly.)
SURGICAL TECHNIQUE: OPEN REDUCTION AND ANNULAR LIGAMENT RECONSTRUCTION
When operative intervention is mandated for an irreducible or highly unstable radial head, a direct approach to the radiocapitellar joint is required.
Step-by-Step Operative Approach
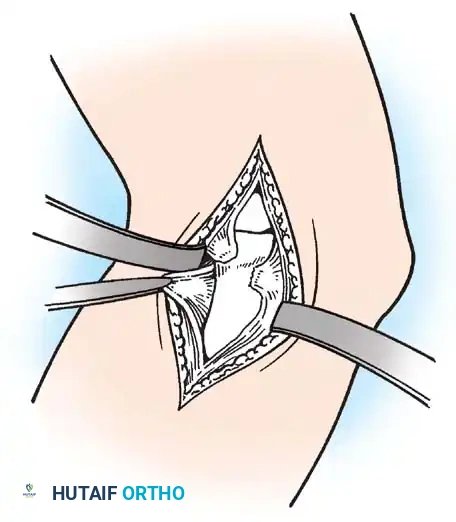
- Incision and Exposure: Make a longitudinal incision over the posterolateral aspect of the elbow, centered over the radial head (Kocher interval between the anconeus and extensor carpi ulnaris).
- Deep Dissection: Carefully expose the radial head and identify the remnants of the ruptured annular ligament.
- Joint Clearance and Reduction: Debride any interposed capsular tissue or hematoma blocking the joint. Anatomically reduce the radial head into the radial notch of the ulna.
- Primary Repair: If the tissue quality permits, repair the annular ligament and the disrupted lateral capsule using fine, non-absorbable interrupted sutures.
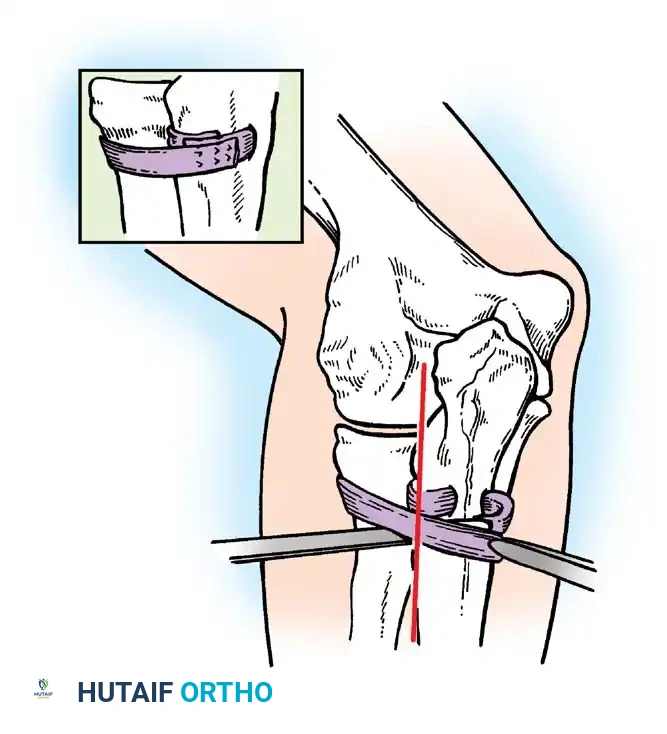
- Ligament Reconstruction (If Primary Repair Fails): If the native ligament is irreparable or deficient, harvest a fascial graft (1.3 cm wide × 10 cm long) from the ipsilateral fascia lata of the thigh (or alternatively, from the deep dorsal fascia of the forearm).
- Ulnar Tunnel Preparation: Expose the posterior surface of the proximal ulna through a secondary 5 cm incision. Drill a transverse osseous tunnel through the ulnar metaphysis, precisely 1.3 cm distal to the articular level of the radial head.
- Graft Passage and Fixation: Pass the strip of fascia lata through this ulnar tunnel, loop it circumferentially around the radial neck, and suture its ends together under appropriate tension to create a robust, neo-annular ligament. Ensure the forearm can fully pronate and supinate without impingement.
Postoperative Protocol
Following annular ligament reconstruction, the arm is placed in a well-padded posterior splint or cast. The elbow is immobilized at 90 degrees of flexion with the forearm in neutral rotation for 2 to 3 weeks.
Following this period, gentle active motion and muscle rehabilitation are initiated.
Pitfall: The elbow must never be forcefully manipulated, and passive stretching must be strictly avoided. Forcing motion increases the risk of heterotopic ossification (myositis ossificans) and recurrent instability.
Slight asymptomatic subluxation of the radial head may occur after motion and strength are restored; however, this rarely interferes significantly with long-term functional outcomes.
COMPLEX FRACTURE-DISLOCATIONS OF THE ELBOW
Complex elbow dislocations characterized by severe soft-tissue disruption and associated periarticular fractures demand aggressive surgical intervention to restore joint congruity and stability. Pheasant and other modern authors strongly recommend that fracture-dislocations with severe soft-tissue compromise should not be managed closed. Instead, they require meticulous debridement, rigid internal fixation of fractures, and primary repair of capsuloligamentous structures.
Pathoanatomy of Complex Instability
Large periarticular fractures adversely affect functional results if left unreduced. A fracture of the coronoid process is a critical sentinel sign; it strongly suggests that the elbow had sustained at least a partial dislocation (subluxation) at the moment of impact.
During surgical exploration of a severe fracture-dislocation, the surgeon will typically encounter:
* Complete avulsion or tearing of the brachialis muscle from its ulnar insertion.
* Extensive avulsion of the anterior joint capsule.
* Complete rupture of the LCL complex and frequently the MUCL.
If these profound soft-tissue injuries are repaired concurrently with the osseous injuries, the return of function is significantly hastened, the final arc of motion is improved, and the potential for devastating myositis ossificans is minimized. In every severe fracture-dislocation of the elbow, the surgeon must also maintain a high index of suspicion for concomitant longitudinal radioulnar dissociation (Essex-Lopresti injury) and meticulously assess the integrity of the distal radioulnar joint (DRUJ).
THE DISTAL RADIOULNAR JOINT (DRUJ)
Injuries to the DRUJ can occur in isolation or in association with almost any fracture of the forearm (e.g., Galeazzi fractures). The primary biomechanical function of the DRUJ is to stabilize the forearm during the complex arc of pronation and supination, acting as the pivot point where the radius rotates around the fixed distal ulna.
Stabilizing Structures of the DRUJ
The distal ulna is covered by articular cartilage and interfaces with the ulnar notch of the radius. The DRUJ is dynamically and statically stabilized by a complex network of structures:
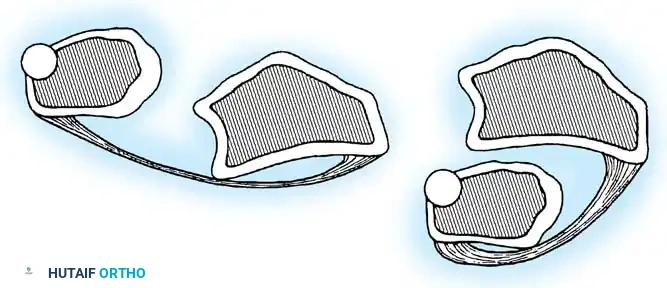
* The Triangular Fibrocartilage Complex (TFCC): The primary stabilizer, including the articular disc attached to the base of the ulnar styloid and the margin of the ulnar notch.
* Radioulnar Ligaments: The volar (anterior) and dorsal (posterior) radioulnar ligaments, which are robust thickenings of the joint capsule.
* Ulnar Collateral Ligament (UCL): Extending from the ulnar styloid to the pisiform and triquetrum.
* Pronator Quadratus: Spans the volar surface of the distal radius and ulna, providing dynamic stabilization.
For a complete DRUJ dislocation to occur, a catastrophic failure of several or all of these structures must take place.
Classification and Closed Management
Dameron emphasized that DRUJ dislocations are classified based on the position of the ulna relative to the radius: dorsal or volar.
- Dorsal Dislocation (Ulna Dorsal): The most common variant. Reduction is typically achieved by firm supination of the forearm combined with direct volar pressure over the distal ulna.
- Volar Dislocation (Ulna Volar): Less common. Reduction is usually successful via forced pronation of the forearm.
If reduced acutely, the forearm is immobilized in a long-arm cast (in supination for dorsal dislocations, or pronation for volar dislocations) for 4 weeks, generally yielding excellent functional results.
Indications for Open Reduction of the DRUJ
Failure to recognize a simple DRUJ dislocation associated with a forearm fracture leads to inadequate immobilization, failure of TFCC healing, and chronic, symptomatic instability.
Open reduction is indicated in the following scenarios:
1. Irreducible Acute Dislocations: Cetti, Jenkins et al., and Hanel and Scheid have extensively described irreducible DRUJ dislocations. In the vast majority of these cases, the Extensor Carpi Ulnaris (ECU) tendon or its subsheath becomes entrapped within the sigmoid notch, physically blocking closed reduction. A dorsal surgical approach is required to extricate the ECU, followed by TFCC repair or transosseous radioulnar pinning.
2. Subacute Dislocations (< 2 months old): If the dislocation cannot be reduced closed, Dameron advises open reduction with direct exposure and anatomic repair of the TFCC.
3. Chronic Dislocations (> 2 months old): Late surgical reduction is fraught with complications due to cartilage necrosis and severe contractures. In these chronic cases, salvage procedures such as excision of the distal ulna (Darrach procedure) or pseudoarthrosis (Sauvé-Kapandji procedure) combined with distal ligamentous reconstruction are indicated.
Diagnostic Pearl: According to Milch, rupture of the distal radioulnar ligaments frequently causes visible diastasis of the DRUJ on standard PA radiographs. This widening is a pathognomonic sign of complete ligamentous rupture necessitating operative repair.
Chronic Instability and Reconstruction Techniques
Rupture of the DRUJ ligaments without an associated fracture is frequently misdiagnosed as a simple wrist sprain. Because the joint is rarely immobilized correctly, the ligaments heal in an elongated position. This damage is often not discovered until 6 to 8 weeks post-injury, by which time secondary osteoarthrosis of the sigmoid notch may have already commenced.
In cases of chronic instability where the articular surfaces remain pristine, complex soft-tissue reconstructions may be attempted. The Bunnell technique is a classic historical method used to tether the distal ulna and prevent dorsal subluxation.
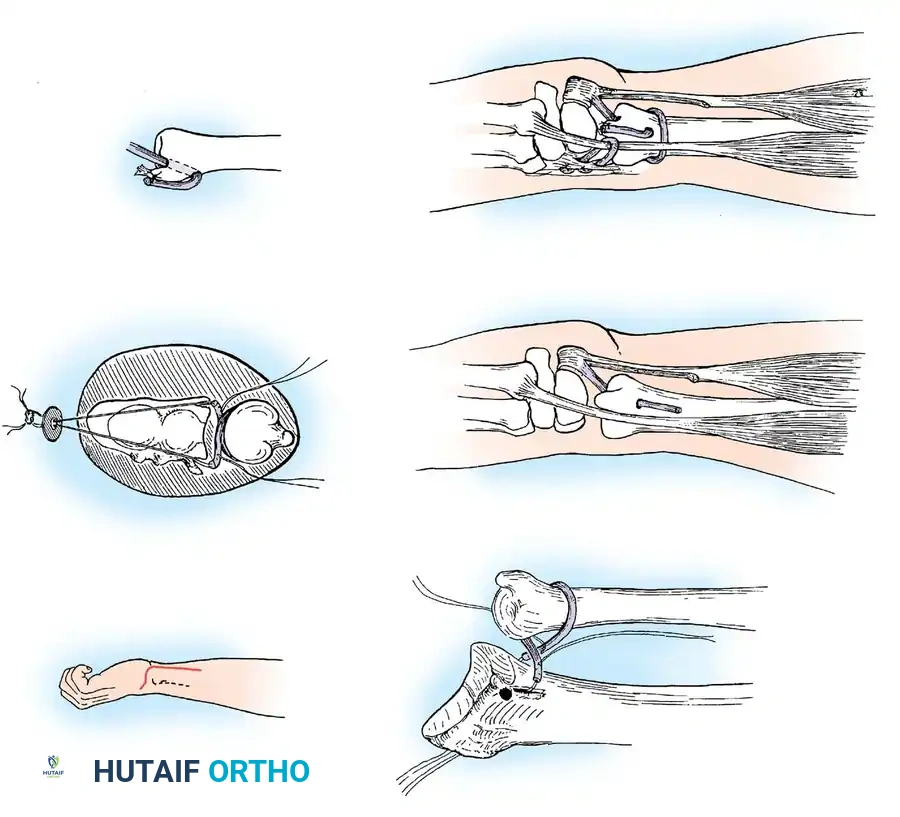
The Bunnell Stabilization Technique:
As illustrated, this procedure involves creating a dynamic and static tether to stabilize the distal ulna:
* A small tendon graft (often palmaris longus) is looped circumferentially around the neck of the ulna and anchored securely into the distal radius to recreate the radioulnar ligaments.
* A tenodesis of the distal ulna is performed using a split portion of the flexor carpi ulnaris (FCU) tendon.
* The extensor carpi ulnaris (ECU) tendon is anchored dorsally via a separate tendon loop to prevent volar subluxation of the tendon during active flexion and pronation of the wrist.
While technically demanding, such reconstructive operations cannot be successful unless the osseous anatomy of the radius and ulna is completely undeformed. If angular deformity exists, corrective osteotomy must precede or accompany any soft-tissue reconstruction of the DRUJ.
