Mastering the Dorsolateral Approach for Bunion Surgery
Introduction & Epidemiology
Hallux valgus, a complex deformity characterized by lateral deviation of the great toe and medial deviation of the first metatarsal, represents one of the most common forefoot pathologies encountered by orthopedic surgeons. Its prevalence is estimated to be as high as 23-35% in the adult population, with a notable increase with age and female predilection. The etiology is multifactorial, encompassing genetic predisposition, footwear choices, and underlying biomechanical imbalances.
Surgical intervention for hallux valgus aims to correct the structural deformity, alleviate pain, and restore functional mechanics of the first metatarsophalangeal (MTP) joint. While over 150 distinct surgical procedures have been described for hallux valgus, the majority involve a combination of soft tissue releases and bony osteotomies. The dorsolateral approach, specifically, provides crucial access to the lateral structures of the first MTP joint, primarily for soft tissue releases that are essential components of a comprehensive correction strategy. Historically, isolated soft tissue procedures were attempted for hallux valgus, often with suboptimal long-term outcomes and high recurrence rates. Current surgical paradigms almost universally incorporate a dorsolateral soft tissue release in conjunction with a medial capsulorrhaphy and a corrective first metatarsal osteotomy to achieve a stable, congruent, and anatomically aligned MTP joint. Understanding the precise indications, detailed surgical technique, and potential complications associated with the dorsolateral approach is paramount for residents and practicing orthopedic surgeons.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the first MTP joint is fundamental to executing a successful dorsolateral approach and achieving a stable correction of hallux valgus.
Anatomical Considerations
The first MTP joint is a condyloid synovial joint, critical for propulsion during gait. Key structures relevant to the dorsolateral approach include:
- Joint Capsule: The fibrous capsule surrounds the MTP joint, reinforced by collateral ligaments. In hallux valgus, the lateral aspect of the capsule becomes contracted and thickened, contributing significantly to the deformity, while the medial capsule is attenuated.
-
Adductor Hallucis Muscle:
This muscle has two heads:
- Oblique head: Originates from the bases of the 2nd, 3rd, and 4th metatarsals and the fibular collateral ligament of the 3rd MTP joint.
-
Transverse head:
Originates from the plantar ligaments of the 3rd, 4th, and 5th MTP joints.
Both heads insert, via a conjoined tendon, into the lateral aspect of the base of the proximal phalanx of the great toe and the lateral sesamoid. The adductor hallucis exerts a strong deforming force, pulling the hallux laterally and the first metatarsal head medially, exacerbating the valgus deformity and lateral sesamoid subluxation.
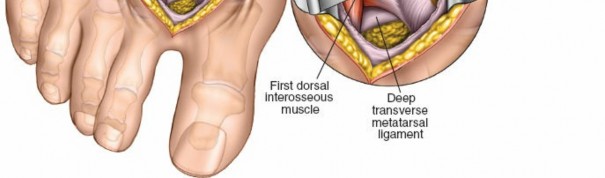
- Transverse Metatarsal Ligament (TML): This strong fibrous band connects the plantar plates of the metatarsal heads, particularly between the first and second. In hallux valgus, it becomes taut and contributes to the lateral displacement of the first metatarsal head relative to the second, impeding metatarsal head reduction.
- Lateral Sesamoid Complex: The lateral (fibular) sesamoid bone is embedded within the plantar plate, articulating with the facet on the plantar aspect of the first metatarsal head. In hallux valgus, the lateral sesamoid typically subluxates laterally, losing its normal articulation with the first metatarsal head, contributing to the "round-about" effect of the deformity and impacting the mechanics of the flexor hallucis brevis tendon.
-
Neurovascular Structures:
Meticulous dissection is required to protect vital structures.
- Dorsal Cutaneous Nerves: Branches of the superficial peroneal nerve often cross the dorsolateral aspect of the first MTP joint. Care must be taken to identify and retract these to prevent iatrogenic neuromas or paresthesias.
- Dorsal Digital Nerves: The common dorsal digital nerve to the first interspace typically divides into proper dorsal digital nerves. These are superficial and vulnerable during skin incision and capsular exposure.
- Dorsal Digital Artery: Situated dorsally and often adjacent to the nerves.
- Plantar Digital Nerves/Arteries: While generally protected by the metatarsal heads, aggressive deep dissection during TML division can risk injury.
Biomechanical Implications of Hallux Valgus
The hallmark of hallux valgus is the progressive instability and malalignment of the first ray.
1.
Metatarsus Primus Varus:
The first metatarsal deviates medially, increasing the intermetatarsal angle (IMA).
2.
Hallux Valgus:
The proximal phalanx deviates laterally relative to the first metatarsal.
3.
Lateral Sesamoid Subluxation:
The fibular sesamoid displaces laterally relative to the first metatarsal head, often remaining with the proximal phalanx, contributing to the "bowstringing" effect of the flexor hallucis brevis.
4.
Adductor Contracture:
The adductor hallucis tendon becomes pathologically contracted, pulling the hallux into valgus and exacerbating lateral sesamoid subluxation. This deforming force is a primary target of the dorsolateral release.
5.
Lateral Capsular Tightness:
The lateral joint capsule and collateral ligaments become adaptively shortened, restricting reduction of the MTP joint.
6.
Medial Capsular Attenuation:
The medial capsule becomes stretched and incompetent, failing to stabilize the joint medially.
The dorsolateral approach directly addresses the contracted lateral soft tissue structures, allowing for correction of the lateral deviation of the hallux and repositioning of the sesamoid complex under the first metatarsal head. This release is a critical prerequisite for successful bony realignment and medial capsular plication.
Indications & Contraindications
The dorsolateral approach for bunion surgery is almost exclusively used for soft tissue corrective procedures in cases of hallux valgus. It is rarely, if ever, performed in isolation, but rather as an integral component of a multi-planar correction strategy.
Indications (Operative)
The primary indication for the dorsolateral approach is to release contracted lateral soft tissues, specifically the adductor hallucis tendon, lateral capsule, and transverse metatarsal ligament, which are essential for correcting hallux valgus deformity.
- Adjuvant to First Metatarsal Osteotomies: Most commonly, the dorsolateral approach is combined with a first metatarsal osteotomy (e.g., Chevron, Scarf, Lapidus) to facilitate reduction of the valgus deformity and allow proper realignment of the MTP joint. The soft tissue release permits easier translation and stabilization of the metatarsal head and reduction of the proximal phalanx.
- Mild-to-Moderate Hallux Valgus: In deformities with an Intermetatarsal Angle (IMA) typically less than 15-18 degrees and Hallux Valgus Angle (HVA) less than 30-35 degrees, the soft tissue component is critical for achieving comprehensive correction.
- Flexible Deformity: The presence of a reducible deformity on clinical examination is a strong indicator that soft tissue release will contribute to correction.
- Lateral Sesamoid Subluxation: When the fibular sesamoid is significantly subluxated laterally (e.g., grade 2 or 3 on Hardy and Clapham classification), its release is essential for restoring proper MTP joint mechanics.
- Recurrent Deformity with Soft Tissue Contracture: In revision cases, addressing residual lateral soft tissue contracture via a dorsolateral approach may be necessary.
Contraindications
Isolated soft tissue procedures utilizing the dorsolateral approach are generally contraindicated. When combined with osteotomies, specific conditions may contraindicate the entire surgical strategy or necessitate modifications.
- Advanced Arthrosis of the MTP Joint: Grade 3-4 degenerative changes of the first MTP joint are an absolute contraindication for joint-preserving procedures like soft tissue release and osteotomy. Fusion (arthrodesis) or arthroplasty would be more appropriate.
- Neuromuscular Disorders with Spasticity: Conditions like cerebral palsy or stroke, causing spasticity, can lead to recurrence if the underlying neuromuscular imbalance is not addressed. Soft tissue releases alone are insufficient and carry a high risk of recurrence.
- Significant Hypermobility of the First Ray: If hypermobility or instability of the first TMT joint is present, a proximal stabilization procedure (e.g., Lapidus arthrodesis) should be prioritized, often in conjunction with a dorsolateral release. Isolated distal procedures will likely fail.
- Excessive Distal Metatarsal Proximal Phalangeal Angle (DMPPA): While controversial, an isolated soft tissue release for a DMPPA (also known as distal articular set angle or DASA) greater than 15 degrees is unlikely to fully correct the deformity and may predispose to hallux varus if combined with an aggressive medial capsular plication without addressing the articular congruency via an Akin osteotomy or similar.
- Severe Vascular Insufficiency: As with all forefoot surgery, a mandatory preoperative assessment of pedal vascularity is crucial. Peripheral artery disease contraindicates elective forefoot surgery due to high risks of wound healing complications and amputation.
- Active Infection: Absolute contraindication for elective surgery.
- Poor Patient Compliance: Lack of adherence to post-operative protocols can jeopardize outcomes.
Table: Operative vs. Non-Operative Indications for Hallux Valgus
| Feature | Non-Operative Management | Operative Management (including Dorsolateral Release) |
|---|---|---|
| Pain | Mild, intermittent, well-controlled with conservative measures. | Moderate to severe, persistent, interfering with activities of daily living. |
| Deformity | Mild, non-progressive, no significant functional limitation. | Progressive, symptomatic, cosmetic concern. |
| Footwear | Accommodated by wider toe-box shoes, orthotics. | Unable to fit into standard footwear due to pain/deformity. |
| Radiographic | Mild angles (HVA < 20°, IMA < 12°), congruent joint, no arthrosis. | Moderate-to-severe angles (HVA > 20°, IMA > 12°), lateral sesamoid subluxation, failed non-operative management. |
| Joint Status | Flexible, no significant arthrosis. | Flexible deformity, or rigid deformity requiring comprehensive correction. |
| Patient Expectation | Realistic about symptom modulation, not structural correction. | Realistic about potential for structural correction and recovery. |
| Associated Pathology | No significant MTPJ arthrosis or other forefoot pathology requiring intervention. | Often associated with MTPJ arthrosis (mild-moderate), metatarsalgia, hammer toes. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical for optimizing surgical efficiency and minimizing complications.
Pre-Operative Planning
-
History and Physical Examination:
- History: Pain location, duration, aggravating/alleviating factors, impact on activity, footwear intolerance, past medical history (diabetes, smoking, neuropathies, vascular disease), medications, allergies.
- Physical Exam: Assess foot morphology (pes planus/cavus), skin integrity, neurovascular status (pulses, sensation), flexibility of the deformity (reducible vs. rigid hallux valgus), MTPJ range of motion, and assessment for associated deformities (hammer toes, metatarsalgia, first ray hypermobility). Evaluate for ankle equinus.
-
Radiographic Evaluation:
-
Weight-bearing Anteroposterior (AP), Lateral, and Oblique Views:
These are essential for comprehensive assessment.
- AP View: Measure Hallux Valgus Angle (HVA), Intermetatarsal Angle (IMA), Distal Metatarsal Articular Angle (DMAA or DASA), assess MTPJ congruence, and classify sesamoid position (Hardy and Clapham grades 0-7, or similar classifications). Evaluate for bone spurs.
- Lateral View: Assess first metatarsal elevation or depression, presence of degenerative changes, and alignment of the entire foot.
- Oblique View: Better visualization of the MTP joint and sesamoids, especially if there's overlap on AP views.
- Consider Stress Radiographs: May be useful to assess first TMT joint hypermobility.
- Advanced Imaging (MRI/CT): Rarely indicated for routine hallux valgus. May be considered for evaluation of avascular necrosis of the metatarsal head, stress fractures, or complex arthrosis if MTPJ fusion is contemplated.
-
Weight-bearing Anteroposterior (AP), Lateral, and Oblique Views:
These are essential for comprehensive assessment.
- Surgical Strategy Discussion: Based on clinical and radiographic findings, determine the specific combination of procedures required (e.g., dorsolateral release + medial capsular plication + Chevron osteotomy + Akin osteotomy). Anticipate the sequence of steps and potential challenges.
Anesthesia and Tourniquet Application
- Anesthesia: General anesthesia is common, but regional blocks (e.g., ankle block, popliteal block) can provide excellent post-operative analgesia and reduce systemic anesthetic exposure. A combination of general anesthesia with a regional block is often preferred.
-
Tourniquet:
- Thigh Tourniquet: Placed on the mid-thigh after padding. The leg is exsanguinated either by elevation for 3-5 minutes or by using an Esmarch bandage from distal to proximal. This provides a bloodless field, which is critical for precise soft tissue dissection and neurovascular protection.
- Ankle Tourniquet: A soft rubber bandage (e.g., Esmarch bandage or specifically designed ankle tourniquet) can be wrapped tightly just proximal to the malleoli for ankle block cases. This provides a localized bloodless field with lower pressure, but its duration is more limited and the field may not be as completely exsanguinated. Ensure proper padding beneath the tourniquet to prevent skin or nerve injury.
-
Exsanguination:
Regardless of tourniquet placement, thorough exsanguination is essential.
 - Image caption: Patient positioned supine on the operating table with a padded thigh tourniquet in place, prepared for exsanguination.
Patient Positioning
- Supine Position: The patient is placed supine on the operating table.
- Leg Positioning: The affected foot is typically positioned at the end of the table or draped off to allow full range of motion of the ankle and MTP joints during the procedure. A sterile drape may be placed under the foot for support.
-
Prep and Drape:
Standard sterile prep and drape are performed, ensuring adequate exposure of the entire foot and ankle to allow for manipulation and potential extension of the surgical field if necessary.
- Image caption: The foot is prepped and draped in a sterile fashion, with the tourniquet inflated, providing a clear surgical field.
Detailed Surgical Approach / Technique
The dorsolateral approach facilitates critical lateral soft tissue releases for hallux valgus correction. The technique described here focuses on a standard approach, which is often performed prior to a medial approach for osteotomy and capsular plication.
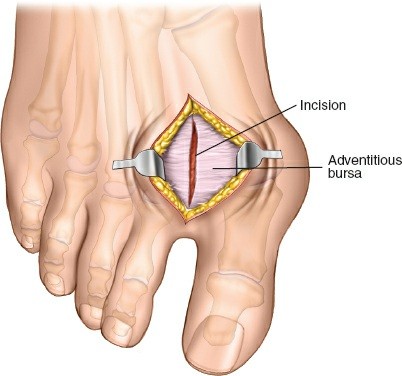
1. Incision
- Localization: A longitudinal skin incision is typically made along the dorsolateral aspect of the first MTP joint, starting approximately 1-2 cm proximal to the joint line over the first metatarsal head and extending distally for 3-4 cm over the proximal phalanx. The incision should be carefully planned to avoid dorsal digital nerves and branches of the superficial peroneal nerve. A curvilinear or slightly oblique incision may also be utilized, following natural skin lines.
- Skin Incision: The incision is carried through the skin with a No. 15 blade.
-
Subcutaneous Dissection:
Blunt and sharp dissection proceeds through the subcutaneous tissue. Identify and protect any visible neurovascular structures. The dorsal digital nerve to the great toe is often found dorsomedial to the incision and must be carefully retracted. Adherence to a layer-by-layer dissection is crucial to prevent iatrogenic nerve injury.
- Image caption: A longitudinal skin incision is made over the dorsolateral aspect of the first MTP joint, extending proximally over the metatarsal head.
2. Capsular Exposure
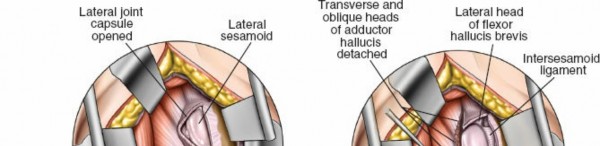
- Capsular Incision: Once the subcutaneous tissues are divided and nerves are protected, the underlying dorsolateral joint capsule of the first MTP joint is exposed. The extensor hallucis longus (EHL) tendon is identified dorsally and typically retracted medially, or kept within the incision to protect it. An L-shaped or longitudinal incision is made in the dorsolateral capsule. The L-shaped incision typically begins dorsally, parallel to the EHL, and extends distally before turning plantarly along the lateral aspect of the proximal phalanx. This allows for excellent exposure of the lateral sesamoid and adductor hallucis insertion.
-
Subperiosteal Dissection:
Elevate the capsule and periosteum from the lateral aspect of the first metatarsal head and proximal phalanx to expose the underlying bone and the lateral sesamoid.
- Image caption: The dorsolateral joint capsule of the first MTP joint has been exposed, and an L-shaped capsular incision is being made, allowing access to the underlying joint and lateral structures.
3. Adductor Hallucis Tendon Tenotomy
- Identification: The adductor hallucis tendon insertion is identified on the lateral aspect of the base of the proximal phalanx and the lateral sesamoid. It can be differentiated from the lateral collateral ligament by its more tendinous, muscle-like appearance.
-
Tenotomy:
Using a fine blade (e.g., No. 15 or 11), the adductor hallucis tendon is sharply divided at its insertion site. Ensure a complete release to allow full correction of the valgus deformity. This can be performed from superior to inferior or inferior to superior. Care must be taken to avoid violating the plantar plate or damaging the lateral collateral ligament inadvertently, though a complete release usually involves some degree of lateral collateral ligament relaxation or partial division.
- Image caption: The adductor hallucis tendon is identified inserting onto the lateral aspect of the proximal phalanx and lateral sesamoid, and is being sharply tenotomized at its insertion.
4. Lateral Sesamoid Release / Excision
- Release: After adductor tenotomy, the lateral (fibular) sesamoid bone is typically still held by its capsular and ligamentous attachments to the proximal phalanx and metatarsal head. These attachments are carefully released using a fine elevator or blade, allowing the sesamoid to be mobilized and centralized beneath the first metatarsal head. The goal is to free the sesamoid completely to allow it to articulate properly post-correction.
-
Excision (Rare):
Excision of the lateral sesamoid bone is rarely performed due to potential complications such as hallux varus, transfer metatarsalgia, or MTP joint instability. Indications for excision might include severe degenerative arthritis of the sesamoid, osteonecrosis, or a non-union of a fractured sesamoid that is persistently symptomatic. If excised, meticulous care must be taken to preserve the flexor hallucis brevis tendon integrity and to close any resultant capsular defect.
- Image caption: After adductor tenotomy, the lateral sesamoid is further mobilized by releasing its remaining capsular and ligamentous attachments to allow for centralization.
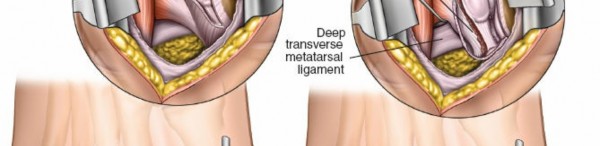
5. Division of the Transverse Metatarsal Ligament (TML)
- Identification: The TML is a strong fibrous band connecting the plantar plates of the first and second metatarsal heads. To access it, the lateral aspect of the first metatarsal head must be further exposed. This step is crucial for allowing medial translation of the first metatarsal head during osteotomy and facilitating correction of the intermetatarsal angle.
-
Division:
With the MTP joint distracted or abducted to create tension on the TML, it is carefully divided using a fine blade or scissors. This must be done with extreme caution to avoid injury to the plantar neurovascular structures running immediately deep to the ligament, particularly the plantar digital nerve to the first interspace. Blunt dissection can be used to palpate these structures prior to division. A narrow Hohmann retractor or lamina spreader can be used to protect the deeper structures.
- Image caption: The transverse metatarsal ligament is carefully identified between the first and second metatarsal heads and divided, ensuring protection of underlying plantar neurovascular structures.
6. Assessment of Correction and Associated Procedures
- Intraoperative Assessment: After the dorsolateral releases are complete, assess the flexibility and reducibility of the hallux valgus deformity. The hallux should now be easily reducible into a corrected position. The lateral sesamoid should be free and mobile.
-
Associated Procedures:
This approach is almost always combined with other procedures:
- First Metatarsal Osteotomy: Classically, first metatarsal osteotomies (e.g., Chevron, Scarf, Lapidus) are performed to address the metatarsus primus varus. These are typically accessed via a dorsomedial incision.
- Medial Capsulorrhaphy/Capsular Plication: Performed through the dorsomedial incision, the medial capsule is imbricated and tightened to stabilize the MTP joint in the corrected position.
- Akin Osteotomy: A medial closing wedge osteotomy of the proximal phalanx may be performed to correct any residual hallux valgus interphalangeus.
-
The sequence is usually dorsolateral release, then metatarsal osteotomy, then medial capsular plication and Akin osteotomy.
- Image caption: Following soft tissue releases and bony correction, the first MTP joint is manipulated to assess for full deformity correction and stability prior to closure.
7. Closure
-
Layered Closure:
- The dorsolateral capsule, if excessively redundant, may be imbricated or reapproximated, but typically, an open capsulotomy is left.
- Subcutaneous tissues are reapproximated with absorbable sutures (e.g., 3-0 or 4-0 Vicryl).
- Skin closure is performed with non-absorbable sutures (e.g., 4-0 nylon) or absorbable subcuticular sutures (e.g., 4-0 Monocryl) for optimal cosmesis.
-
Dressing:
A sterile, multi-layered compression dressing is applied to maintain the corrected position and minimize swelling. This typically includes a non-adherent primary dressing, gauze, cotton padding, and an elastic bandage. A bunion splint or post-operative shoe is often applied to protect the correction.
- Image caption: The wound is meticulously closed in layers, and a sterile, multi-layered dressing is applied, often with a splint, to maintain the corrected alignment.
Complications & Management
While the dorsolateral approach itself is generally safe, it is an integral part of a larger bunion correction, and potential complications often relate to the overall procedure. Understanding and anticipating these is crucial for effective management.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (approx.) | Management / Salvage Strategies |
|---|---|---|
| Recurrence of Deformity | 10-25% (overall bunion surgery), higher for isolated soft tissue release. |
Prevention:
Thorough pre-op planning, complete soft tissue releases, accurate osteotomy, stable fixation, appropriate post-op rehab.
Management: Depends on etiology (inadequate release, unstable fixation, hypermobility, patient factors). May require revision surgery (further osteotomy, fusion, soft tissue balancing), exostectomy for painful medial prominence. |
| Hallux Varus (Overcorrection) | 2-5% (overall bunion surgery) |
Prevention:
Judicious lateral release, avoiding excessive medial capsular tightening, appropriate osteotomy correction.
Management: Early recognition allows non-operative management (taping, splinting). If rigid, may require revision (lateral soft tissue plication, medial release, potential MTPJ fusion or arthroplasty, IP fusion if flexible). |
| MTP Joint Stiffness / Limited ROM | 5-15% |
Prevention:
Early, controlled range of motion exercises, meticulous soft tissue handling, avoiding excessive soft tissue scarring.
Management: Physical therapy (mobilization, stretching), anti-inflammatory measures. If persistent, MTPJ manipulation under anesthesia, cheilectomy for dorsal impingement, or rarely, arthrolysis. |
| Nerve Injury | 1-10% (dorsal cutaneous/digital nerve) |
Prevention:
Careful skin incision, meticulous layer-by-layer dissection, identifying and protecting neural structures.
Management: Most neurapraxias resolve spontaneously. Neuropathic pain may be treated with medications (gabapentin, tricyclics). Persistent painful neuroma may require surgical excision or transposition. |
| Infection | 1-3% (superficial), <1% (deep) |
Prevention:
Strict aseptic technique, appropriate perioperative antibiotics, good wound care.
Management: Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, IV antibiotics, hardware removal if present and infected, culture-directed therapy. |
| Delayed Wound Healing / Dehiscence | <5% |
Prevention:
Meticulous surgical technique, avoiding excessive tension on skin edges, careful patient selection (e.g., diabetics, smokers).
Management: Local wound care, débridement, offloading. May require secondary closure or skin grafting in severe cases. |
| Transfer Metatarsalgia | 5-15% (related to metatarsal shortening/elevation) |
Prevention:
Careful attention to metatarsal length and plantar inclination during osteotomy.
Management: Custom orthotics, metatarsal pads, shoe modifications. If severe and recalcitrant, may require lesser metatarsal osteotomy. |
| Avascular Necrosis (AVN) of 1st Metatarsal Head | <1-5% (primarily with distal osteotomies, e.g., Chevron) |
Prevention:
Preservation of vascular supply to the metatarsal head (e.g., maintaining medial periosteal hinge with Chevron).
Management: Non-operative (offloading, anti-inflammatories) for mild cases. If symptomatic collapse, may require MTPJ fusion or arthroplasty. |
| Complex Regional Pain Syndrome (CRPS) | <1% |
Prevention:
Careful patient handling, adequate pain control, early mobilization.
Management: Multidisciplinary approach: physical therapy, pain management (nerve blocks, medications), psychological support. Early diagnosis is key. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes, preventing complications, and facilitating a timely return to function. Protocols vary slightly based on the specific procedures performed (e.g., soft tissue only vs. osteotomy) and surgeon preference. The following outlines a typical protocol for a combined dorsolateral release and first metatarsal osteotomy.
Phase I: Immediate Post-Operative (Weeks 0-2)
- Goals: Protect surgical repair, minimize swelling and pain, prevent wound complications.
- Weight-Bearing: Non-weight bearing or partial weight-bearing in a post-operative shoe (hard-soled shoe with stiff shank) or controlled ankle motion (CAM) boot, emphasizing heel-weight bearing if tolerated. Full non-weight bearing with crutches is often prescribed if a significant osteotomy or instability is present.
-
Immobilization:
- A soft compression dressing is applied immediately post-op to maintain alignment and reduce swelling.
- Often, a bunion splint (e.g., velcro toe strap) is used to maintain hallux alignment.
- Pain Management: Opioids initially, transitioning to NSAIDs and acetaminophen. Regional nerve blocks can provide excellent immediate post-operative analgesia.
- Edema Control: Strict elevation above heart level (especially for the first 48-72 hours), regular ice application.
- Wound Care: Keep dressing clean and dry. First dressing change typically occurs at 1-2 weeks. Monitor for signs of infection or wound healing issues.
- Activity: Minimal activity, focusing on rest and elevation.
Phase II: Early Mobilization (Weeks 2-6)
- Goals: Restore controlled range of motion (ROM), protect bony healing, gradually increase weight-bearing.
-
Weight-Bearing:
- Gradual progression to partial weight-bearing, then full weight-bearing in a post-operative shoe or CAM boot, depending on osteotomy stability and radiographic evidence of healing.
- If stable osteotomy, may progress to flat-soled, stiff-soled shoe around week 4.
-
Exercises:
- Initiate gentle, active and passive range of motion (ROM) exercises for the first MTP joint. Focus on dorsiflexion and plantarflexion. Avoid aggressive passive ROM to prevent overcorrection or disruption of healing tissues.
- Gentle toe curls, toe spreads.
- Intrinsic foot muscle activation exercises.
- Physical Therapy: May begin formal physical therapy to guide ROM and strengthening.
- Edema Control: Continue elevation and ice as needed. Compression stockings may be introduced.
- Wound Care: Suture removal at 2-3 weeks. Continue monitoring wound. Scar massage once wound is fully closed.
Phase III: Intermediate Rehabilitation (Weeks 6-12)
- Goals: Restore full MTP joint ROM, improve strength, regain normal gait mechanics.
- Weight-Bearing: Transition out of post-operative shoe into supportive athletic shoes. Avoid high heels or restrictive footwear.
-
Exercises:
- Progressive ROM and strengthening exercises for the foot and ankle musculature.
- Balance and proprioception exercises (e.g., single-leg stance).
- Gait training to normalize walking pattern.
- Stretching for the Achilles tendon if ankle equinus is present.
- Activity: Gradually increase activity levels. Low-impact activities (swimming, cycling) can be introduced. Avoid high-impact activities (running, jumping sports) until 3-4 months post-op.
- Shoe Wear: Recommend spacious, supportive footwear. Custom orthotics may be prescribed if underlying biomechanical issues persist.
Phase IV: Advanced Rehabilitation & Return to Activity (Weeks 12+)
- Goals: Return to full activity, optimize long-term function and strength.
- Activity: Progressive return to sport-specific activities, ensuring adequate strength, balance, and pain-free motion.
- Long-Term Care: Continue foot and ankle strengthening. Regular follow-up appointments with the surgeon, typically at 3, 6, and 12 months, with radiographs to monitor alignment and healing.
Summary of Key Literature / Guidelines
The evolution of hallux valgus surgery has consistently reinforced the principle that successful and durable correction requires addressing both the soft tissue and bony components of the deformity. The dorsolateral soft tissue release, targeting the adductor hallucis tendon, lateral capsule, and transverse metatarsal ligament, is a cornerstone of this comprehensive approach.
- Historical Context: Early attempts at isolated soft tissue correction, such as the McBride procedure (McBride, 1928), often yielded high recurrence rates (up to 40-50%) when performed without concomitant bony correction, especially in moderate to severe deformities. This led to a consensus that soft tissue release must be coupled with osteotomy.
- Combined Procedures: Modern literature overwhelmingly supports the use of the dorsolateral release in conjunction with first metatarsal osteotomies (e.g., distal Chevron, proximal crescentic or closing wedge, Lapidus arthrodesis). Studies by Trnka et al. (1999) and Coughlin and Shurnas (2003) have demonstrated superior long-term outcomes and lower recurrence rates when addressing both bony and soft tissue components.
- Adductor Tenotomy: The complete release of the adductor hallucis tendon is considered essential by most surgeons. Sarrafian (1983) and others have detailed the biomechanical implications of its contracture and the necessity of its division to allow proper repositioning of the hallux.
- Lateral Capsular Release: Contraction of the lateral capsule is a primary deforming force. Its release, in conjunction with adductor tenotomy, facilitates relocation of the MTP joint. However, excessive lateral release without adequate medial soft tissue balancing can predispose to hallux varus.
- Transverse Metatarsal Ligament Division: While some debate its routine necessity, many authors, including Maestro et al. (2000), advocate for TML division, particularly in cases with increased intermetatarsal angles, as it facilitates reduction of the first metatarsal and normalizes forefoot width. Care must be taken to avoid neurovascular injury.
- Sesamoid Realignment: The goal of lateral release is to allow the fibular sesamoid to be centralized under the first metatarsal head. This re-establishes the normal mechanical advantage of the flexor hallucis brevis and contributes to stability. Excision of the lateral sesamoid is now rarely performed due to the significant risk of hallux varus and other complications (Hattrup et al., 2000).
- Outcomes and Complications: While overall patient satisfaction rates for bunion surgery are high (85-95%), complications like recurrence, stiffness, and nerve injury remain concerns. The incidence of complications is influenced by surgical technique, patient factors, and the severity of the initial deformity. Long-term studies emphasize the importance of achieving and maintaining MTP joint congruence and adequate correction of radiographic angles (HVA, IMA) for sustained success.
- Current Guidelines: Professional organizations generally recommend a staged, patient-specific approach to hallux valgus surgery, integrating appropriate soft tissue balancing with bony correction based on the degree of deformity, joint congruency, and patient comorbidities. The dorsolateral approach is a vital part of the armamentarium for successful hallux valgus correction.
In conclusion, the dorsolateral approach for bunion surgery, targeting the adductor hallucis tendon, lateral capsule, and transverse metatarsal ligament, is a technically demanding yet critical component of a comprehensive hallux valgus correction. Mastery of this approach requires a profound understanding of forefoot anatomy, biomechanics, indications, meticulous surgical technique, and astute management of potential complications. It is rarely a standalone procedure, but rather a synergistic element that permits successful bony realignment and medial soft tissue stabilization, ultimately leading to improved patient outcomes.
Clinical & Radiographic Imaging