Mastering Great Toe Dorsal Approaches for MTP Joint Surgery
Introduction & Epidemiology
The first metatarsophalangeal (MTP) joint is a critical structure for ambulation, balance, and propulsion during gait. Pathologies affecting this joint, such as hallux valgus and hallux rigidus, represent a significant proportion of forefoot surgical interventions. The dorsal approach to the great toe MTP joint is a versatile and widely utilized surgical corridor, providing excellent exposure for a myriad of reconstructive and ablative procedures. Its inherent advantages include direct access to the joint capsule, dorsal exostoses, and the extensor mechanism, making it suitable for addressing both osseous and soft tissue deformities.
Hallux valgus, characterized by lateral deviation of the great toe and medial prominence of the first metatarsal head, affects a substantial portion of the adult population, with reported prevalence rates ranging from 23% to 35% across various demographics. Symptomatic hallux valgus often necessitates surgical correction to alleviate pain, improve footwear tolerance, and restore biomechanical function. Hallux rigidus, a degenerative arthritic condition of the first MTP joint, progresses through stages of cartilage loss and osteophyte formation, leading to pain and restricted motion. Its prevalence is estimated to be around 1 in 45 individuals over the age of 50, making it one of the most common arthritic conditions of the foot. Other conditions like trauma, inflammatory arthropathy, and tumors may also necessitate surgical intervention via a dorsal approach.
The evolution of surgical techniques, coupled with a deeper understanding of the biomechanics and anatomy of the first ray, has led to improved outcomes. The dorsal approach remains a cornerstone of forefoot surgery, enabling surgeons to precisely address complex deformities while minimizing collateral tissue damage.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the first MTP joint and its surrounding structures is paramount for successful outcomes and complication avoidance.
Bony Anatomy
The first MTP joint is formed by the articulation of the convex head of the first metatarsal and the concave base of the proximal phalanx. The first metatarsal head is typically wider medially than laterally, contributing to the medial eminence often seen in hallux valgus. The sesamoid bones, embedded within the flexor hallucis brevis tendons, articulate with two distinct facets on the plantar aspect of the first metatarsal head, forming the sesamoid-metatarsal articulation. These sesamoids act as a fulcrum for the flexor hallucis brevis, increasing its mechanical advantage, and protecting the plantar plate and flexor hallucis longus tendon. The proximal phalanx base provides the articular surface for the metatarsal head.
Ligamentous Structures
The joint capsule surrounds the MTP joint, reinforced by a complex network of ligaments:
*
Collateral Ligaments:
Strong medial and lateral collateral ligaments originate from the metatarsal head and insert onto the proximal phalanx base. They provide primary stability, preventing varus/valgus deviation.
*
Plantar Plate:
A fibrocartilaginous structure on the plantar aspect of the joint, continuous with the joint capsule, serving as a critical stabilizer against dorsal subluxation and hyperextension. It anchors the sesamoids to the proximal phalanx.
*
Deep Transverse Metatarsal Ligament (DTML):
Connects the plantar plates of adjacent MTP joints, providing transverse stability to the forefoot. The connection between the first and second MTP joints is often implicated in hallux valgus deformity.
Tendinous Structures
- Extensor Hallucis Longus (EHL): Lies dorsally, responsible for great toe dorsiflexion. Its tendon runs over the MTP joint and inserts onto the distal phalanx. It often contributes to the dorsal contracture in hallux rigidus.
- Flexor Hallucis Longus (FHL): Passes plantar to the sesamoids and inserts onto the distal phalanx, primarily responsible for great toe plantarflexion.
- Flexor Hallucis Brevis (FHB): Divides into medial and lateral heads, inserting into the medial and lateral sesamoids, respectively, before continuing to the proximal phalanx.
- Abductor Hallucis: Originates from the medial calcaneal tuberosity and inserts onto the medial aspect of the proximal phalanx and medial sesamoid, contributing to toe abduction and arch support.
- Adductor Hallucis: Composed of oblique and transverse heads, inserting onto the lateral aspect of the proximal phalanx and lateral sesamoid. It is a major deforming force in hallux valgus.
Neurovascular Structures
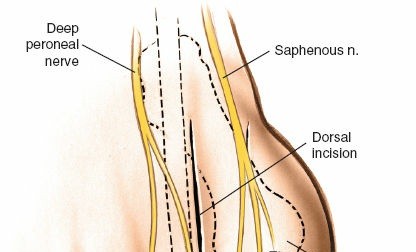
- Dorsal Cutaneous Nerves: Branches of the superficial fibular nerve (intermediate dorsal cutaneous) and medial dorsal cutaneous nerve (from the saphenous nerve) supply sensation to the dorsum of the foot and toes. The medial dorsal cutaneous nerve and its branches are particularly vulnerable during dorsal approaches, especially when extending medially.
- Dorsal Digital Nerves: The proper dorsal digital nerve to the great toe (a branch of the medial dorsal cutaneous nerve) and the common digital nerve between the first and second toes (a branch of the deep fibular nerve) are at risk.
- Dorsal Metatarsal Arteries: The first dorsal metatarsal artery and its digital branches run dorsally, providing blood supply. Meticulous dissection is required to protect these vessels.
Biomechanics
The first MTP joint is integral to the "windlass mechanism" described by Hicks, where dorsiflexion of the toes during propulsion tightens the plantar aponeurosis, elevating the arch and converting the foot into a rigid lever for push-off.
*
Hallux Valgus:
In hallux valgus, the lateral deviation of the great toe leads to malalignment, abnormal load transfer, and disruption of the windlass mechanism. The adductor hallucis and EHL often become deforming forces, and the medial collateral ligament becomes attenuated.
*
Hallux Rigidus:
Progressive cartilage degeneration and osteophyte formation restrict motion, particularly dorsiflexion, impairing the push-off phase of gait and causing compensatory changes in adjacent joints. Dorsal osteophytes are common and directly restrict dorsiflexion.
Indications & Contraindications
The dorsal approach is highly versatile for a broad range of MTP joint pathologies.
Indications for Operative Intervention
The dorsal approach is employed for most surgeries of the great toe MTP joint, primarily addressing bunions (hallux valgus) and hallux rigidus, but also encompassing other conditions.
- Excision of Metatarsal Exostosis (Bunionectomy): Resection of the prominent medial eminence of the first metatarsal head in hallux valgus.
- Distal Metatarsal Osteotomy: Corrective osteotomies of the first metatarsal (e.g., Chevron, Reverdin, Scarf, Weil, Mau) to realign the metatarsal head, correct the intermetatarsal angle, and improve metatarsal length.
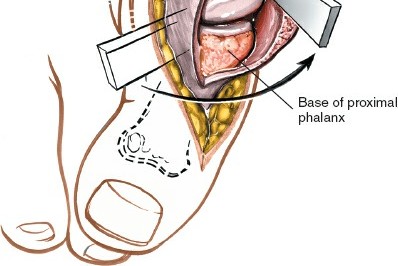
- Excision of the Proximal Part of the Proximal Phalanx: A component of resectional arthroplasty (e.g., Keller arthroplasty) for severe hallux rigidus or revision surgery.
-
Soft Tissue Correction of Hallux Valgus:
This includes:
- Lateral Release: Tenotomy of the adductor hallucis tendon, release of the lateral joint capsule, and release of the fibular sesamoid ligament to balance soft tissue tension.
- Medial Capsular Reefing: Tightening of the medial joint capsule to correct valgus deformity.
- EHL Lengthening/Tenotomy: Rarely performed but can address significant EHL contracture.
- Arthrodesis of the Metatarsophalangeal Joint: Fusion of the MTP joint, primarily for severe hallux rigidus, failed arthroplasty, severe hallux valgus with arthritis, or neuropathic joints, aiming for a stable, pain-free joint.
- Insertion of Total Joint Replacements: Arthroplasty (hemi or total) for advanced hallux rigidus, offering motion preservation.
- Dorsal Wedge Osteotomy of the Proximal Phalanx (e.g., Akin osteotomy): A medial closing wedge osteotomy of the proximal phalanx, often an adjunctive procedure in hallux valgus correction, or a dorsal closing wedge osteotomy for hallux rigidus (Moberg osteotomy) to increase dorsiflexion.
- Cheilectomy: Debridement of dorsal osteophytes from the metatarsal head and proximal phalanx base for early to moderate hallux rigidus to improve dorsiflexion.
- Trauma: Open reduction and internal fixation of intra-articular fractures or complex dislocations of the first MTP joint.
Contraindications
Absolute contraindications are few but critical:
* Active local infection (cellulitis, osteomyelitis).
* Severe peripheral vascular disease with compromised tissue perfusion (risk of non-healing, necrosis).
* Uncontrolled systemic diseases (e.g., diabetes, rheumatoid arthritis) with high operative risk or poor healing potential.
* Severe neuropathy (e.g., Charcot arthropathy) unless specific management protocols are in place.
* Severely attenuated or compromised skin envelope over the surgical site (e.g., frank ulceration, deep infection, extreme thinning as noted in the seed content).
* Patient unwillingness or inability to comply with post-operative rehabilitation protocols.
Relative contraindications include poor nutritional status, smoking, and psychological conditions impacting compliance.
Operative vs. Non-Operative Indications
| Indication Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Hallux Valgus | Symptomatic deformity (pain, footwear difficulty, callosities), failed extensive non-operative management (shoe modifications, orthoses), significant radiographic deformity (HVA > 20°, IMA > 10°, symptomatic DMAA > 10°). Presence of bunion pain, MTP joint arthritis, or hammer toe deformities secondary to HV. | Asymptomatic deformity, mild pain managed with conservative measures. Patient preference against surgery. Mild radiographic deformity (HVA < 20°, IMA < 10°). Contraindications to surgery. |
| Hallux Rigidus | Symptomatic, progressive MTP joint pain, limited dorsiflexion (<50% normal ROM), and radiographic evidence of degenerative changes (Grade II-IV classification), failed conservative treatment (NSAIDs, injections, shoe modifications, orthoses). Persistent pain at end-range motion. | Mild symptoms, early radiographic changes (Grade 0-I), pain controlled with conservative measures. Adequate functional range of motion for daily activities. Patient preference against surgery. Contraindications to surgery. |
| MTP Joint Arthritis | Significant pain and functional impairment, radiographic evidence of advanced arthritis (loss of joint space, osteophytes, subchondral sclerosis/cysts), failed conservative management. | Mild or intermittent pain, managed with conservative measures, early radiographic changes without severe functional limitation. |
| Trauma | Displaced intra-articular fractures, irreducible dislocations, unstable ligamentous injuries, non-unions or malunions causing pain/dysfunction. | Stable, non-displaced fractures, stable ligamentous injuries without significant functional deficit, successfully reduced closed dislocations. |
| Tumor/Mass | Symptomatic lesions, suspicious for malignancy, rapidly growing masses, or masses causing compression/erosion of adjacent structures. | Asymptomatic benign lesions (e.g., ganglion cysts) confirmed by imaging or biopsy, or lesions with low suspicion for malignancy that are stable in size and not causing functional impairment. |
| Failed Surgery | Persistent pain, recurrence of deformity, hardware complications (prominence, loosening), nonunion/malunion, infection requiring revision. | Asymptomatic hardware, minor radiographic residual deformity not causing symptoms, patient content with initial outcome. |
Pre-Operative Planning & Patient Positioning
Pre-Operative Planning
-
Clinical Assessment:
- History: Detailed symptom analysis including pain location, intensity, aggravating/alleviating factors, duration, footwear difficulties, activity limitations, and prior treatments. Medical comorbidities, allergies, and medication review are essential.
-
Physical Examination:
- Vascular Status: Palpation of dorsal pedis and posterior tibial pulses, capillary refill time. In cases of concern, ankle-brachial index (ABI) should be measured. As noted in the seed content, a careful assessment of the skin and vascular state of the foot is mandatory, especially with red, thin, or inflamed skin, and certainly with frank ulceration.
- Skin Condition: Assess for callosities, ulceration, inflammation, and integrity, especially over the medial eminence in bunions.
- Neurological Exam: Sensation (light touch, sharp/dull, two-point discrimination), motor strength.
- MTP Joint Assessment: Range of motion (dorsiflexion, plantarflexion, abduction, adduction), stability (collateral ligaments), joint line tenderness, presence of crepitus. Assess for lesser toe deformities and hypermobility of the first ray.
- Gait Analysis: Observe the patient's gait pattern for compensatory mechanisms.
-
Radiographic Evaluation:
-
Weight-Bearing Anteroposterior (AP), Lateral, and Oblique Views:
These are the standard.
- AP View: Assess Hallux Valgus Angle (HVA), Intermetatarsal Angle (IMA), Distal Metatarsal Articular Angle (DMAA), and sesamoid position (Hardy and Clapham classification). Evaluate joint space narrowing, osteophytes, and subluxation.
- Lateral View: Assess MTP joint congruity, presence of dorsal osteophytes (hallux rigidus), Meary's angle (alignment of talus, navicular, cuneiforms, and first metatarsal). Evaluate for metatarsus primus elevatus.
- Oblique View: Better visualization of the lateral sesamoid and second MTP joint.
- Advanced Imaging (as needed): CT scan for complex intra-articular fractures or revision surgery to delineate bony architecture. MRI for soft tissue pathology, osteomyelitis, or pre-operative planning for tumor resection.
-
Weight-Bearing Anteroposterior (AP), Lateral, and Oblique Views:
These are the standard.
- Anesthetic Consultation: Discuss regional anesthesia (e.g., ankle block, popliteal block) vs. general anesthesia.
- Informed Consent: Detailed discussion of the procedure, expected outcomes, potential complications, and post-operative course.
- Tourniquet Considerations: Midthigh tourniquet for procedures requiring prolonged ischemia (e.g., arthrodesis, complex osteotomies) or an ankle tourniquet for shorter procedures with less extensive dissection. An ankle tourniquet can be applied using a soft rubber bandage to exsanguinate the foot and then wrap the leg tightly just above the ankle. Ensure adequate padding and appropriate inflation pressures.
Patient Positioning
Place the patient supine on the operating table. The affected foot should be positioned at the end of the table or over a bump to allow for unrestricted manipulation of the MTP joint during the procedure. A sterile tourniquet, placed midthigh or supramalleolar, is applied but not inflated until the foot is fully prepped and draped. Exsanguination of the limb is performed prior to tourniquet inflation. The limb is then sterilely prepared with an antiseptic solution (e.g., povidone-iodine or chlorhexidine) and draped in a standard fashion, ensuring ample sterile field for instrument placement and limb manipulation.
Detailed Surgical Approach / Technique
The dorsal approach offers direct access to the MTP joint, facilitating precise osseous and soft tissue modifications. The specific incision and deep dissection strategy may vary slightly based on the pathology and chosen reconstructive procedure.
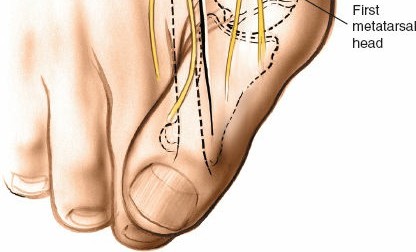
Landmarks and Incision
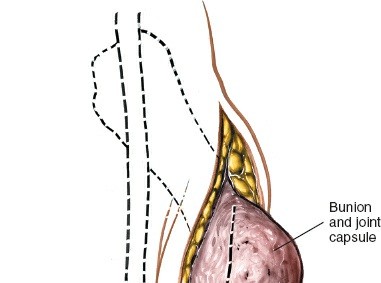
Palpate the head of the first metatarsal bone and the metatarsophalangeal joint , which are readily identifiable on the ball of the foot and its medial border. The MTP joint line is typically palpable approximately 1 cm distal to the prominent medial eminence of the metatarsal head.
A common approach involves a dorsomedial longitudinal incision approximately 4-6 cm in length, centered over the first MTP joint. It typically extends from the mid-diaphysis of the first metatarsal distally to the mid-diaphysis of the proximal phalanx. The incision should be slightly curved, following the natural skin creases where possible, or straight. For procedures focused on the medial eminence, a more medially placed incision is advantageous. For procedures requiring significant dorsal access (e.g., cheilectomy, dorsal wedge osteotomy), a more dorsally centered incision, parallel to the EHL tendon, is appropriate. Careful planning of the incision is critical to avoid tension on closure, especially in the presence of thin, inflamed skin overlying a bunion.
A typical dorsomedial longitudinal incision for access to the first MTP joint.
Layered Dissection
-
Skin and Subcutaneous Tissue:
- Incise the skin with a No. 15 blade.
- Undermine the skin and subcutaneous tissues cautiously using sharp and blunt dissection. Identify and protect the medial dorsal cutaneous nerve and its branches, which typically run within the subcutaneous fat dorsomedially. These nerves are highly vulnerable to injury, and their preservation is crucial to avoid post-operative numbness or painful neuromas. Retract them carefully. Similarly, identify and protect superficial veins.
-
Deep Fascia:
- The deep fascia overlying the extensor hallucis longus (EHL) tendon is incised longitudinally. The EHL tendon is now visible.
- The EHL tendon is typically retracted laterally to expose the underlying joint capsule. In some dorsal approaches, especially for cheilectomy, the EHL may be tenotomized in a Z-lengthening fashion if significant contracture is present, or a longitudinal incision is made directly adjacent to it.
-
Capsular Incision:
-
The choice of capsular incision depends on the specific procedure and desired exposure.
- T-Capsulotomy: A longitudinal incision centered over the joint, with a transverse limb along the joint line. This provides excellent exposure for arthrodesis, arthroplasty, and severe hallux rigidus. The flaps can be used for later reefing.
- H-Capsulotomy: Similar to T-capsulotomy but with two longitudinal limbs, providing wide exposure.
- Inverted L-Capsulotomy (medial approach): A longitudinal incision along the medial aspect of the joint with a transverse limb along the plantar base of the proximal phalanx. This allows for lateral soft tissue release and medial capsular reefing.
- Dorsal Longitudinal Capsulotomy: A simple longitudinal incision over the dorsum of the joint, often used for cheilectomy or dorsal wedge osteotomy.
- After incising the capsule, the MTP joint is exposed. Synovium may be debrided if inflamed or hypertrophic.
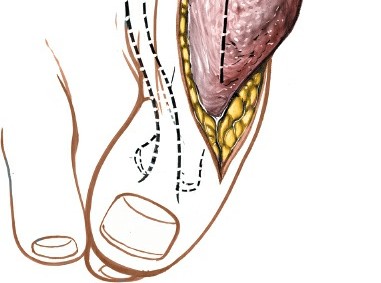
-
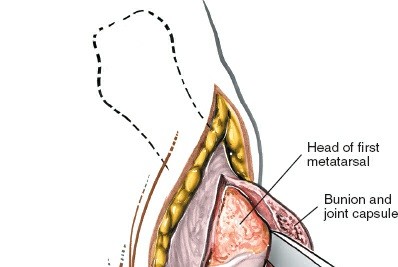
 - Exposure of the MTP joint capsule following initial dissection. Note the protection of neurovascular structures.
-
The choice of capsular incision depends on the specific procedure and desired exposure.
Operative Procedures (Integration within the Approach)
Once the MTP joint is exposed, the specific pathology is addressed.
1. Excision of Metatarsal Exostosis (Bunionectomy)
- The medial capsule is incised, and a periosteal elevator is used to raise the periosteum and capsule off the medial eminence of the first metatarsal head. Care is taken to stay subperiosteal to protect the medial collateral ligament.
- The medial eminence is resected using an oscillating saw or osteotome, typically parallel to the medial shaft of the first metatarsal, ensuring sufficient bone is removed to eliminate the prominence without compromising the integrity of the metatarsal head or articular surface. Avoid over-resection, which can lead to hallux varus.
-
Bone edges are rasped smooth.
-
 - Resection of the medial metatarsal eminence using an oscillating saw.
-
2. Soft Tissue Correction (Hallux Valgus)
- Lateral Release: Following exposure, the MTP joint is distracted. Using a small blade (e.g., #64 Beaver blade) or a fine electrocautery tip, the tight lateral capsule, the fibular sesamoid ligament, and the adductor hallucis tendon insertion on the lateral base of the proximal phalanx are sequentially released. This release facilitates correction of the valgus deformity and lateral shift of the sesamoids. The amount of release is guided by intraoperative correction.
- Medial Capsular Reefing: After bony correction, the medial capsule, which has been stretched in hallux valgus, is imbricated or reefed to maintain correction and provide medial stability. This can be performed with non-absorbable sutures, advancing the distal flap proximally.
3. Distal Metatarsal Osteotomy
- For common osteotomies like the Chevron (Austin) or Reverdin-Laird, a V-shaped cut is made in the metatarsal head. For a Chevron osteotomy, the apex is placed at the metatarsal head.
- The capital fragment is translated laterally to reduce the intermetatarsal angle.
- Fixation is typically achieved with a single or two small diameter screws (e.g., 2.0 mm, 2.4 mm, or 2.7 mm cortical screws). K-wires can also be used, especially in younger patients or for less stable constructs.
-
Other osteotomies, such as the Weil osteotomy (shortening osteotomy for lesser metatarsalgia), may also be performed via a dorsal approach, often in conjunction with great toe surgery.
-
 - Example of distal metatarsal osteotomy with subsequent fixation using small cortical screws.
-
4. Proximal Phalanx Osteotomy (Akin or Moberg)
- An Akin osteotomy is a medial closing wedge osteotomy of the proximal phalanx performed for residual hallux valgus interphalangeus. A medially based wedge of bone is resected from the proximal phalanx, and the fragments are compressed and fixed with a K-wire or small screw.
-
A
Moberg osteotomy
is a dorsal closing wedge osteotomy of the proximal phalanx, used for hallux rigidus to increase dorsiflexion. A dorsal wedge is removed from the proximal phalanx, and the fragments are compressed and fixed.
-
 - Illustration of a proximal phalanx osteotomy, demonstrating bone resection and subsequent fixation.
-
5. Cheilectomy
- For hallux rigidus, osteophytes are meticulously removed from the dorsal aspect of the metatarsal head and the base of the proximal phalanx using an osteotome, rongeurs, or a high-speed burr.
- The aim is to remove sufficient bone to allow at least 60-70 degrees of pain-free dorsiflexion.
- Any synovitis or inflamed soft tissue is debrided.
6. Arthrodesis of the MTP Joint
- For severe arthritis, instability, or failed previous surgery, arthrodesis provides a pain-free, stable joint.
- The articular cartilage from both the metatarsal head and proximal phalanx base is completely resected using a sagittal saw, osteotome, or burr until bleeding subchondral bone is exposed.
-
The bone ends are then prepared to ensure maximal apposition and stability. Common techniques include:
- Flat Cut: Resect flat surfaces perpendicular to the desired fusion angle.
- Concave-Convex: Create a concave surface on one bone and a convex surface on the other to enhance stability.
- Peg-in-Hole: Create a peg on one bone and a corresponding hole in the other.
- The joint is positioned in optimal functional alignment: typically 5-10 degrees of valgus and 10-15 degrees of dorsiflexion. The ideal position allows comfortable shoe wear and facilitates the push-off phase of gait.
-
Fixation can be achieved with two or more cancellous screws, a dorsal plate, or a combination. The goal is rigid internal fixation to promote fusion.
-
 - Preparation of bone surfaces for MTP joint arthrodesis, demonstrating precise bone resection.
-
7. Total Joint Replacements
- Following capsular and soft tissue release, the MTP joint is disarticulated.
- The metatarsal head and proximal phalanx base are resected to accommodate the selected implant components. Resection guides are used to ensure precise bone cuts.
- Trial components are inserted to assess fit, alignment, and range of motion.
- The definitive components (often metal for the metatarsal and polyethylene for the phalanx, or ceramic/pyrocarbon implants) are then inserted, either press-fit or cemented, according to manufacturer specifications.
Closure
- Copious irrigation of the surgical site.
- Hemostasis is achieved.
- The joint capsule is closed where feasible and desired (e.g., medial capsular reefing), typically with absorbable sutures.
- The deep fascia is closed.
- The subcutaneous tissue is closed with absorbable sutures, taking care to evert skin edges.
- The skin is closed with non-absorbable sutures or staples.
- A sterile dressing is applied, often with a soft compressive bandage to maintain correction and control edema.
Complications & Management
Despite meticulous surgical technique, complications can arise. Recognition and appropriate management are crucial for salvage.
Common Complications and Management Strategies
| Complication | Incidence | Risk Factors `
Metatarsal and Phalangeal Osteotomies:
* **Distal Metatarsal Osteotomy:**
* **Chevron Osteotomy:** For hallux valgus correction. A V-shaped cut (angle 60 degrees) is made in the distal metatarsal, with the apex at the metatarsal head. The capital fragment is translated laterally to reduce the intermetatarsal angle (IMA). Dorsal or plantar tilt may be introduced to correct an elevated or depressed first metatarsal.
* ``
* *Demonstrates a distal metatarsal osteotomy (e.g., Chevron), with the capital fragment translated and fixed with a small screw. Note the precision of the saw cuts.*
* **Reverdin-Laird Osteotomy:** A similar osteotomy to Chevron but with a plantar hinge, allowing for correction of an increased DMAA and removal of a medial wedge for HV correction.
* **Weil Osteotomy:** A dorsal-to-plantar oblique osteotomy used to shorten the metatarsal. While most commonly performed on lesser metatarsals, it can be utilized on the first metatarsal to address forefoot load transfer issues.
* **Proximal Phalanx Osteotomies:**
* **Akin Osteotomy:** A medially based closing wedge osteotomy of the proximal phalanx, approximately 5-7mm distal to the joint, used to correct hallux valgus interphalangeus. A small wedge of bone is removed from the medial cortex, allowing for the phalanx to be closed and fixed.
* **Moberg Osteotomy (Dorsal Wedge Osteotomy):** A dorsal closing wedge osteotomy of the proximal phalanx (often 20-30 degrees) to increase dorsiflexion in hallux rigidus. This shifts the articulation dorsally, allowing more motion.
* ``
* *Illustrates a dorsal closing wedge osteotomy of the proximal phalanx (Moberg), showing the bone wedge removed and anticipated fragment compression. This image could also represent an Akin osteotomy if the wedge was removed medially.*
Fixation:
- For osteotomies and fusions, rigid internal fixation is crucial.
- Screws: Small diameter cortical or cancellous screws (e.g., 2.0-3.5mm) are commonly used for osteotomies and arthrodesis. Lag screw technique provides compression.
- K-wires: Used for temporary stabilization or definitive fixation in selected cases (e.g., Akin osteotomy, pediatric osteotomies).
- Plates: Low-profile dorsal plates (e.g., mini-fragment plates, locking plates) are increasingly used for MTP arthrodesis, providing robust fixation and allowing earlier weight-bearing.
Soft Tissue Balancing & Closure:
- Following bony procedures, the MTP joint is tested for stability and range of motion.
- Medial Capsular Reefing: If performed, the medial capsule is imbricated using non-absorbable sutures to stabilize the corrected hallux valgus deformity.
- EHL Lengthening: Rarely indicated but can be performed with a Z-plasty if significant EHL contracture persists, especially in hallux rigidus.
- The deep fascia is closed with absorbable sutures.
- Subcutaneous fat is approximated to eliminate dead space and minimize tension on the skin.
- Skin closure is performed with non-absorbable sutures or staples.
- A sterile dressing is applied, often with a splint or surgical shoe that maintains the toe in a corrected position.
Post-Operative Rehabilitation Protocols
Rehabilitation protocols vary significantly based on the specific surgical procedure (e.g., arthrodesis vs. osteotomy) and surgeon preference. The general principles focus on pain management, edema control, protection of the repair, and gradual return to function.
General Principles
- Pain Management: Multimodal approach (NSAIDs, acetaminophen, opioids as needed). Regional blocks can provide initial prolonged analgesia.
- Edema Control: Strict elevation above heart level for the first 1-2 weeks, ice application, and compression dressings.
- Weight-Bearing: Determined by the stability of fixation and bone healing.
- Wound Care: Keep incision dry and clean. Monitor for signs of infection.
Protocol Examples
1. Hallux Valgus Correction (Osteotomy with Soft Tissue Repair)
-
0-2 Weeks (Protection Phase):
- Weight-Bearing: Partial weight-bearing (PWB) in a post-operative shoe or boot, or full weight-bearing (FWB) in a surgical shoe if stable fixation is achieved. Crutches or a walker may be used.
- Immobilization: Soft dressing with toe splinting to maintain correction.
- Activity: Strict elevation. Gentle ankle ROM.
- Goal: Protect repair, minimize swelling, pain control.
-
2-6 Weeks (Early Mobilization):
- Weight-Bearing: Progress to FWB in surgical shoe or stiff-soled shoe.
- Mobilization: Initiate gentle active and passive MTP joint range of motion (ROM) exercises, focusing on plantarflexion and dorsiflexion. Scar massage once wound is healed.
- Activity: Gradual increase in ambulation. Stationary cycling may begin.
- Goal: Restore MTP joint motion, reduce stiffness.
-
6-12 Weeks (Progressive Strengthening):
- Weight-Bearing: Transition to comfortable athletic shoes. Orthotics may be prescribed.
- Strengthening: Initiate toe curls, toe raises, intrinsic foot muscle exercises. Balance exercises.
- Activity: Return to low-impact activities.
- Goal: Restore strength, balance, normal gait mechanics.
-
3-6 Months+ (Return to Activity):
- Activity: Gradual return to higher impact activities and sports as tolerated. Continue with strengthening and flexibility exercises.
- Goal: Full recovery of function.
2. Hallux Rigidus (Cheilectomy)
-
0-2 Weeks (Protection & Early Motion):
- Weight-Bearing: FWB in a stiff-soled post-operative shoe.
- Mobilization: Immediate active and passive MTP joint ROM exercises, particularly dorsiflexion, to prevent recurrence of stiffness and osteophyte formation. Physical therapy initiated early.
- Goal: Maintain gains in dorsiflexion, minimize pain and swelling.
-
2-6 Weeks (Progressive Motion & Strengthening):
- Weight-Bearing: Transition to comfortable shoes.
- Mobilization: Continue aggressive ROM exercises.
- Strengthening: Intrinsic foot muscle strengthening.
-
6-12 Weeks (Return to Activity):
- Activity: Gradual return to activities. Emphasis on footwear modification and supportive inserts.
- Goal: Maximize functional ROM, pain reduction.
3. MTP Joint Arthrodesis
-
0-6 Weeks (Immobilization & Protection):
- Weight-Bearing: Non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) in a CAM boot or cast.
- Immobilization: Strict immobilization of the MTP joint to promote fusion.
- Activity: Crutch ambulation. Elevation and ice.
- Goal: Achieve solid fusion, prevent hardware failure.
-
6-12 Weeks (Gradual Weight-Bearing):
- Weight-Bearing: Transition to PWB, then FWB in CAM boot, based on radiographic evidence of healing and clinical assessment of tenderness.
- Activity: Continue elevation.
- Goal: Protect healing fusion, gradual return to protected ambulation.
-
3-6 Months+ (Consolidation & Return to Activity):
- Weight-Bearing: Transition to comfortable, stiff-soled shoes.
- Activity: Gradual increase in activities as bone consolidation progresses.
- Goal: Full fusion, pain-free ambulation.
Summary of Key Literature / Guidelines
The literature on dorsal approaches to the first MTP joint is extensive, reflecting decades of evolving understanding and surgical refinement. Key themes include:
- Hallux Valgus Correction: Numerous studies compare various osteotomies (e.g., Chevron vs. Scarf vs. proximal osteotomies) and soft tissue balancing techniques. Outcomes generally show good to excellent results with high patient satisfaction, but recurrence rates vary. Long-term studies emphasize the importance of addressing all components of the deformity, including IMA, HVA, DMAA, and sesamoid position. Recent literature explores minimally invasive techniques as an alternative, but open dorsal approaches remain the gold standard for many complex corrections.
-
Hallux Rigidus Management:
- Cheilectomy: Widely supported for Grade I and II hallux rigidus, offering excellent pain relief and improved dorsiflexion in the short to medium term. Success depends on adequate bone resection and early post-operative mobilization.
- Moberg Osteotomy: Often combined with cheilectomy for Grade II and III hallux rigidus to improve dorsiflexion, particularly in younger patients.
- Arthrodesis: Considered the gold standard for Grade III and IV hallux rigidus, failed cheilectomy, or revision surgery, offering reliable pain relief and predictable outcomes with high fusion rates (often >90%) when stable fixation is achieved. Functional outcomes are generally good despite the loss of motion.
- Arthroplasty (Hemi-/Total): Offers the advantage of motion preservation. Outcomes are less predictable than arthrodesis, with concerns regarding component wear, loosening, and osteolysis. Contemporary implants show improved results, but arthroplasty is generally reserved for older, less active patients or those with specific demands for motion.
- Complication Rates: Studies consistently report low rates of serious complications, with superficial infection, nerve irritation, and recurrence of deformity being the most common. Avascular necrosis of the metatarsal head (particularly with aggressive capital osteotomies) is a rare but debilitating complication, emphasizing careful surgical technique and vascular preservation.
- Patient-Reported Outcomes (PROs): Increasing emphasis on PRO measures (e.g., AOFAS score, SF-36, FAAM) demonstrates good functional improvement and patient satisfaction across a range of dorsal MTP procedures.
- Rehabilitation: Evidence supports early mobilization protocols where appropriate, particularly for cheilectomy and some osteotomies, to mitigate stiffness and optimize functional recovery. Strict non-weight-bearing or protected weight-bearing is crucial for arthrodesis and unstable osteotomies until radiographic signs of healing are present.
The dorsal approach to the first MTP joint remains a cornerstone of forefoot surgical practice. Mastery of its anatomical nuances, technical steps, and management of potential complications is essential for all orthopedic surgeons addressing pathologies of the great toe. Continuous review of the evolving literature ensures the application of evidence-based practices and optimal patient outcomes.
Clinical & Radiographic Imaging