Dorsal Approach for Morton: Optimal Neuroma Treatment
Introduction & Epidemiology
Morton's neuroma, or interdigital neuroma, is a common compressive neuropathy of the foot, characterized by perineural fibrosis and nerve degeneration, typically affecting the common digital nerve. While historically termed a "neuroma," it is pathologically not a true tumor but rather a reactive hyperplasia of the nerve sheath and surrounding tissues, involving demyelination, endoneurial edema, and vascular proliferation. The condition primarily manifests as forefoot pain, often described as burning, tingling, or electric shock-like sensations, exacerbated by weight-bearing activities and constrictive footwear. Pain frequently radiates into the toes. The most common location is the third intermetatarsal space, affecting the third common digital nerve which receives contributions from both the medial and lateral plantar nerves. The second intermetatarsal space is the next most common site, while the first and fourth spaces are rarely involved.
Epidemiologically, Morton's neuroma is significantly more prevalent in women than men, with a reported ratio of approximately 4:1. It most frequently affects individuals in their middle decades, typically between 30 and 60 years of age. Factors implicated in its etiology include repetitive microtrauma, biomechanical abnormalities leading to increased pressure on the interdigital nerve, and entrapment beneath the deep transverse metatarsal ligament (DTML). The dorsal surgical approach for Morton's neuroma excision offers distinct advantages, particularly concerning incision placement in a non-weight-bearing area, which minimizes post-operative scar tenderness and facilitates earlier mobilization compared to traditional plantar approaches.
Differential diagnosis is crucial and includes metatarsophalangeal joint (MTPJ) synovitis, plantar plate tears, stress fractures of the metatarsals, Freiberg's infraction, ganglion cysts, and tarsal tunnel syndrome. Clinical diagnosis is supported by findings such as localized tenderness in the affected web space and a positive Mulder's click, though this sign is not pathognomonic. Diagnostic imaging, primarily ultrasound and magnetic resonance imaging (MRI), plays a vital role in confirming the diagnosis, assessing neuroma size, and excluding other forefoot pathologies. Ultrasound offers a dynamic evaluation, demonstrating the neuroma's compressibility and characteristic "tear-drop" shape. MRI provides superior anatomical detail and can differentiate the neuroma from soft tissue masses or inflammatory conditions.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the forefoot is paramount for a successful dorsal approach. The common digital nerves arise from the medial and lateral plantar nerves. The third common digital nerve, being the most frequently affected, is unique in receiving contributions from both the medial (via the second common digital nerve) and lateral (via the fourth common digital nerve) plantar nerves. This bifurcation often positions the nerve more anteriorly within the third web space, making it potentially more susceptible to compression.
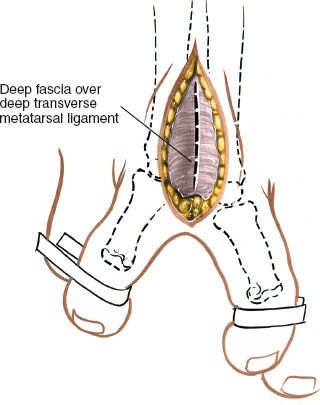
The common digital nerves run longitudinally within the intermetatarsal spaces, superficial to the interosseous muscles and deep to the deep transverse metatarsal ligament (DTML). The DTML is a strong fibrous band connecting the heads of the metatarsals, effectively creating a tunnel through which the common digital nerves pass as they bifurcate into their respective proper digital branches. Compression of the nerve beneath the DTML, exacerbated by metatarsal head splaying during weight-bearing and constrictive footwear, is a primary biomechanical factor in neuroma development. The nerve's vascular supply, derived from the plantar metatarsal arteries, is also vulnerable to this compression, potentially leading to ischemic changes and perineural fibrosis.
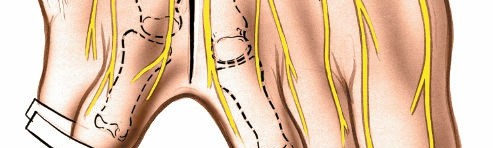
Adjacent structures of critical surgical importance include the dorsal digital arteries and veins, which lie superficial to the deep fascia and must be carefully identified and protected or ligated during the dorsal approach. The lumbrical muscles are situated plantar to the common digital nerves, and the interossei lie deep. The fat pad within the intermetatarsal space provides some cushioning but can itself become inflamed or fibrotic around the nerve.

The image above illustrates the anatomical relationship of the common digital nerve within the intermetatarsal space, highlighting its proximity to the metatarsal heads and the DTML, which are key structures in the pathophysiology of Morton's neuroma.
Indications & Contraindications
Surgical intervention for Morton's neuroma is typically considered only after failure of comprehensive non-operative management strategies. The decision for surgery is guided by the persistence and severity of symptoms and the impact on the patient's quality of life.
Indications for Surgical Intervention
- Failure of Conservative Management : Persistent, debilitating pain despite a minimum of 3-6 months of non-operative treatment, including appropriate footwear modifications, orthotics, activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), and at least two appropriately administered corticosteroid/local anesthetic injections. Other non-operative modalities such as alcohol sclerosing injections or radiofrequency ablation may also have been attempted without success.
- Severe and Disabling Pain : Pain that significantly impairs daily activities, ambulation, and quality of life, unresponsive to less invasive measures.
- Clear Clinical and Radiographic Diagnosis : A well-defined neuroma identified through clinical examination (e.g., Mulder's click, localized tenderness) and confirmed by imaging (ultrasound or MRI), ruling out other forefoot pathologies.
- Recurrent Neuroma : Cases where previous non-operative treatments or even prior surgical decompressions/excisions have failed to provide lasting relief, necessitating re-excision or stump neuroma management.
Contraindications for Surgical Intervention
- Resolved Symptoms : Spontaneous resolution or complete relief with conservative measures.
- Unwillingness or Inability to Undergo Surgery : Patients who decline surgery or have co-morbidities that significantly increase surgical risk.
- Active Local or Systemic Infection : Presence of infection at the surgical site or uncontrolled systemic infection.
- Severe Peripheral Neuropathy : Pre-existing conditions such as diabetic neuropathy, which can confound diagnosis and alter post-operative sensory outcomes.
- Coagulopathy or Bleeding Disorders : Uncorrected bleeding diatheses that increase surgical risk.
- Poor Skin Integrity : Compromised skin at the intended surgical site, which could impair wound healing.
- Unrealistic Patient Expectations : Patients who have not been thoroughly educated on the potential outcomes, including persistent numbness or the risk of stump neuroma.
Operative vs. Non-Operative Indications
| Indication Type | Non-Operative Management | Operative Management |
|---|---|---|
| Symptom Severity | Mild to moderate pain, intermittent symptoms | Severe, debilitating, constant pain |
| Duration | Acute onset, symptoms present for < 3-6 months | Chronic symptoms, present for > 6 months despite adequate conservative trials |
| Previous Tx | Initial presentation, no prior interventions | Failed multiple conservative modalities (footwear, orthotics, NSAIDs, injections, ablation) |
| Imaging Findings | Small neuroma (e.g., <5 mm) or equivocal findings | Confirmed neuroma on imaging, especially larger lesions (>5-7 mm) |
| Associated Path. | No significant co-existing forefoot pathology | Clear diagnosis of Morton's neuroma, other pathologies ruled out or adequately addressed |
| Patient Factors | Willingness to comply with conservative measures, low surgical risk | High impact on daily activities, desire for definitive treatment, appropriate surgical risk assessment |
| Recurrence | Not applicable | Recurrent neuroma after previous non-operative or operative treatment, particularly a painful stump neuroma formation |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is crucial for optimizing surgical outcomes and minimizing complications.
Pre-Operative Planning
- Comprehensive History and Physical Examination : Reconfirm the diagnosis, identify the precise web space(s) involved, and rule out other concurrent forefoot pathologies. Assess for any signs of peripheral neuropathy.
- Imaging Review : Meticulously review pre-operative ultrasound and/or MRI images to confirm the size and exact location of the neuroma, its relationship to surrounding structures, and to identify any other incidental findings that could influence the surgical approach.
- Patient Education : Thoroughly counsel the patient regarding the nature of the procedure, expected post-operative course, potential complications (especially persistent numbness in the resected nerve distribution and the risk of stump neuroma), and realistic outcome expectations.
- Surgical Consent : Obtain informed consent explicitly detailing the risks and benefits.
- Anesthesia Consultation : Determine appropriate anesthesia (regional block, general anesthesia, or monitored anesthesia care). A popliteal nerve block can be beneficial for post-operative pain control.
- Antibiotic Prophylaxis : Administer prophylactic broad-spectrum antibiotics (e.g., cefazolin) within 60 minutes prior to incision, as per institutional guidelines.
- Tourniquet : Prepare for the use of a pneumatic tourniquet, typically placed on the proximal thigh or ankle, to ensure a bloodless field.
- Marking : Pre-operatively mark the incision site over the affected web space with the patient standing and non-weight-bearing to accurately localize the anatomy.
Patient Positioning
- Supine Position : The patient is placed in the supine position on the operating table.
- Lower Extremity Preparation : The operative leg is externally rotated to allow comfortable access to the dorsal aspect of the foot. A bump or bolster may be placed under the ipsilateral hip to facilitate this.
- Tourniquet Application : A pneumatic thigh tourniquet is applied proximally. An ankle tourniquet can also be used if the patient has suitable lower leg anatomy and no contraindications. The tourniquet is inflated to appropriate pressure after exsanguination of the limb.
- Sterile Prep and Drape : The foot and ankle are prepped with an antiseptic solution (e.g., povidone-iodine or chlorhexidine gluconate) from the toes to the mid-calf. The limb is then draped in a sterile fashion, ensuring adequate exposure of the forefoot.
- Foot Position : The foot is positioned flat or with a slight degree of plantarflexion at the ankle to optimize access to the dorsal aspect of the forefoot. The toes should be free for manipulation.
Detailed Surgical Approach / Technique
The dorsal approach for Morton's neuroma excision is favored by many surgeons due to its advantages of a non-weight-bearing incision, reduced risk of painful plantar scar, and generally good exposure.
-
Incision :
- A longitudinal incision, approximately 3-4 cm in length, is made centered over the affected intermetatarsal space, extending from slightly proximal to the metatarsal heads distally towards the web space.
- Care is taken to avoid transverse skin creases to minimize scar contracture.
-
The skin incision can be slightly curvilinear or "lazy S" shaped for better cosmetic results and to avoid direct tension.

The image depicts the typical dorsal longitudinal incision used for accessing the intermetatarsal space for neuroma excision. The incision is placed directly over the affected web space.
-
Dissection to Deep Fascia :
- The skin and subcutaneous tissues are carefully incised.
- Dorsal digital veins are often encountered in the subcutaneous plane. These can be either carefully retracted or ligated/cauterized if necessary.
- The dorsal digital nerves are identified and protected; they lie superficial to the deep fascia.
- Careful blunt dissection with fine scissors or a scalpel through the subcutaneous fat exposes the deep fascia covering the intermetatarsal space.
-
Incision of Deep Fascia and Exposure of DTML :
- The deep fascia is incised longitudinally in line with the skin incision.
- The intermetatarsal fat pad is then meticulously separated by blunt dissection, typically using a small spreader or hemostat, to reveal the underlying deep transverse metatarsal ligament (DTML).
-
The DTML is identified as a thick, white, fibrous band running transversely between the metatarsal heads, typically deep to the fat pad.

This image demonstrates the deep dissection, showing the exposure of the deep transverse metatarsal ligament (DTML) and the identification of the underlying interdigital nerve. Retractors are carefully placed to maintain exposure.
-
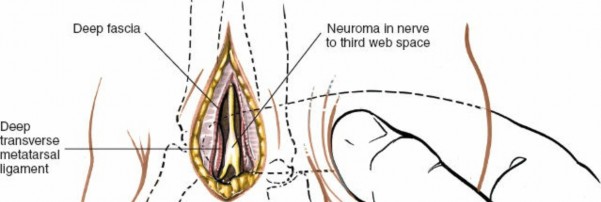
Identification and Isolation of the Common Digital Nerve :
- The common digital nerve is located plantar to the DTML. It is often necessary to carefully divide the DTML transversely to gain adequate exposure to the nerve, particularly when performing an excision to prevent recurrent compression. Some surgeons advocate for DTML release even without full neuroma excision to decompress the nerve.
- Once the DTML is exposed, careful blunt dissection directly plantar to it, typically in the intermetatarsal space, will reveal the common digital nerve. The neuroma itself often appears as a fusiform, whitish, thickened enlargement of the nerve.
-
A nerve hook or fine forceps can be used to gently elevate the nerve and distinguish it from surrounding tissues.
Here, the common digital nerve, enlarged by the neuroma, is clearly isolated with a nerve hook. The surrounding tissues are carefully retracted to ensure optimal visualization prior to transection.
-
Neurectomy (Neuroma Excision) :
- Once the neuroma and the healthy nerve proximally and distally are well visualized, the nerve is carefully dissected free from its surrounding attachments.
- Attention must be paid to the proper digital branches distally and the common digital nerve proximally.
- The nerve should be transected proximally as far as possible to minimize the risk of stump neuroma formation. Ideally, the proximal nerve stump should be resected into the non-weight-bearing musculature (e.g., interosseous muscle or lumbrical belly) to provide a soft tissue buffer.
- Fine suture ligatures (e.g., 5-0 or 6-0 absorbable) are placed proximal and distal to the neuroma to control any accompanying vascular supply and minimize retraction or hemorrhage.
- The nerve is sharply transected with a new, sharp scalpel blade to create a clean cut, minimizing nerve crush injury.
-
The neuroma specimen is sent for histopathological confirmation.
This image shows the neuroma after its proximal and distal attachments have been prepared for transection. The nerve has been carefully dissected free, and the planned transection points are visible.
-
Closure :
- Achieve meticulous hemostasis.
- The DTML, if incised, is typically not repaired to avoid potential recurrence of nerve compression.
- The deep fascia may be loosely approximated if desired, but often left open to further decompress the space.
- The subcutaneous tissues are closed with interrupted absorbable sutures (e.g., 3-0 or 4-0 absorbable) to obliterate dead space and reduce tension on the skin.
- The skin is closed with fine non-absorbable sutures (e.g., 4-0 or 5-0 nylon) or surgical staples.
-
A sterile dressing is applied, followed by a soft compressive bandage.
The resected Morton's neuroma is shown here, demonstrating the fusiform thickening typical of the condition. Histopathological examination of this specimen confirms the diagnosis.

This image illustrates the completed skin closure following the neuroma excision. The incision is neat, and a sterile dressing is being applied, signifying the end of the surgical procedure.
Complications & Management
While generally safe, Morton's neuroma excision can be associated with several complications. Patient education pre-operatively on these potential issues is critical.
| Complication | Incidence (Approximate) | Management Strategy |
|---|---|---|
| Stump Neuroma (Recurrent Neuroma) | 5-20% | Prevention : Meticulous proximal resection of the nerve into soft, non-weight-bearing tissue (e.g., interosseous muscle, lumbrical belly). Treatment : Re-excision of the painful stump, often with more aggressive proximal resection, nerve capping (e.g., silicone cap, vein graft), or implantation into muscle/bone. Cryoablation or radiofrequency ablation may also be considered for smaller stumps. |
| Persistent Numbness/Dysesthesia | 100% of nerve distribution (numbness), variable (dysesthesia) | Prevention : Patient counseling pre-operatively regarding expected numbness. Treatment : Reassurance that numbness is expected. Dysesthesia may improve over time; neuropathic pain medications (e.g., gabapentin, pregabalin, tricyclic antidepressants) may be helpful for persistent symptoms. Topical agents. |
| Infection | 1-2% | Prevention : Strict aseptic technique, prophylactic antibiotics. Treatment : Superficial infections: local wound care, oral antibiotics. Deep infections: surgical debridement, intravenous antibiotics, wound culture-guided therapy. |
| Wound Dehiscence/Delayed Healing | <5% | Prevention : Atraumatic tissue handling, appropriate skin closure, tension-free closure. Treatment : Local wound care, dressing changes. For significant dehiscence, secondary closure or surgical debridement and primary closure (if possible) may be required. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Prevention : Minimally traumatic surgery, good pain control. Treatment : Early diagnosis is critical. Multidisciplinary approach involving pain management specialists, physical therapy, sympathetic blocks, medications (e.g., gabapentin, NSAIDs, corticosteroids). |
| Vascular Injury | Rare | Prevention : Careful dissection, clear identification of dorsal digital vessels. Treatment : Ligation of minor vessels. Repair of major vessels (though rare in this region) by vascular surgeon if critical. |
| Scar Pain/Adhesions | Variable | Prevention : Dorsal approach inherently reduces weight-bearing scar pain. Treatment : Scar massage, silicone sheeting, physical therapy to mobilize soft tissues. Steroid injections into painful scar tissue may be considered. |
| Recurrence of Symptoms (non-neuroma related) | Variable | Prevention : Thorough pre-operative evaluation to rule out other pathologies. Treatment : Re-evaluation of diagnosis, repeat imaging, consideration of other forefoot pathologies (e.g., MTPJ synovitis, plantar plate injury, metatarsalgia). |
Post-Operative Rehabilitation Protocols
A structured post-operative rehabilitation protocol is essential to ensure optimal recovery, minimize complications, and facilitate a timely return to activity.
Immediate Post-Operative Phase (Days 0-14)
- Weight-Bearing : Non-weight-bearing or partial weight-bearing with crutches/walker in a rigid sole surgical shoe or boot, as tolerated. The goal is to protect the surgical site and reduce swelling.
- Elevation and Ice : Maintain elevation of the foot above heart level as much as possible to minimize swelling. Apply ice packs (20 minutes on, 20 minutes off) to the dorsal forefoot for the first 48-72 hours.
- Pain Management : Prescribe appropriate oral analgesics, as needed. Regional blocks can significantly aid initial pain control.
- Wound Care : Keep the dressing clean and dry. Instruct the patient on signs of infection. Suture removal typically occurs at 10-14 days post-operatively.
- Mobility : Gentle ankle pump exercises to promote circulation and prevent stiffness. Avoid active or passive toe range of motion in the affected digits for the first week to allow initial soft tissue healing.
Early Mobilization Phase (Weeks 2-6)
- Weight-Bearing : Gradually progress to full weight-bearing in a surgical shoe or boot. Once sutures are removed and the incision is well-healed, transition to a wide, comfortable athletic shoe with a stiff sole.
- Range of Motion : Begin gentle active and passive range of motion exercises for the toes and MTP joints, focusing on regaining flexibility.
- Scar Management : Once the incision is fully closed, initiate gentle scar massage with lotion or vitamin E oil to help prevent adhesions and improve scar pliability. Silicone sheeting can also be beneficial.
- Activity Modification : Avoid high-impact activities, prolonged standing, and constrictive footwear.
- Physical Therapy (Optional) : If stiffness, swelling, or gait abnormalities persist, referral to a physical therapist may be beneficial for targeted exercises and modalities.
Return to Activity Phase (Weeks 6-12 and Beyond)
- Footwear : Continue to wear wide, comfortable shoes with good arch support and a low heel. Custom orthotics may be considered if pre-operative biomechanical issues were identified or if symptoms persist with standard footwear.
- Activity Progression : Gradually increase activity levels. Begin with low-impact exercises such as walking, cycling, or swimming. Slowly reintroduce activities like jogging or sports, listening carefully to the body for any discomfort.
- Strengthening and Proprioception : Incorporate exercises to strengthen the intrinsic foot muscles and improve balance and proprioception.
- Full Recovery : Complete recovery and return to unrestricted activity can take anywhere from 3 to 6 months, depending on individual healing rates, neuroma size, and the presence of any complications. Persistent numbness in the affected web space is expected and should be continually reinforced with the patient.
Summary of Key Literature / Guidelines
The literature consistently supports neurectomy as an effective treatment for recalcitrant Morton's neuroma, with success rates generally reported between 70% and 90%. While both plantar and dorsal approaches have demonstrated comparable clinical outcomes regarding pain relief, the dorsal approach is increasingly favored due to its lower incidence of painful plantar scarring, which can be a significant source of post-operative morbidity with the plantar approach.
Several studies highlight the importance of meticulous surgical technique, particularly regarding the proximal transection of the nerve. Excision of the nerve as proximally as possible, preferably into the non-weight-bearing intrinsic musculature (e.g., interosseous muscle or lumbrical belly), has been shown to reduce the incidence of painful stump neuroma formation. The formation of a painful stump neuroma remains the most common and challenging long-term complication, with reported incidence rates varying widely but generally ranging from 5% to 20%.
The role of the deep transverse metatarsal ligament (DTML) in neuroma formation and recurrence is also a consistent theme in the literature. While some surgeons advocate for simple DTML release (neurolysis) without neurectomy for smaller neuromas, current consensus for established, painful neuromas typically favors excision to address the reactive hyperplasia and fibrosis. For recurrent cases, re-excision with careful consideration of nerve transposition or capping techniques is often employed.
Current guidelines emphasize the importance of a comprehensive non-operative trial before considering surgery. Corticosteroid injections, while providing temporary relief for many, rarely offer a permanent solution for true neuromas. Alcohol sclerosing injections and cryoablation are less invasive alternatives to surgery that have shown varying degrees of success, often considered as a bridge therapy or for patients unsuitable for surgery. However, for definitive treatment of well-established, symptomatic neuromas unresponsive to conservative measures, surgical excision via a dorsal approach remains the gold standard. Long-term studies underscore the durable efficacy of surgical neurectomy when performed with proper technique, providing significant pain relief and improved functional outcomes for appropriately selected patients.
Clinical & Radiographic Imaging