INTRODUCTION TO COMPLEX DISTAL RADIUS RECONSTRUCTION
The management of highly comminuted, intra-articular distal radius fractures presents a formidable challenge, particularly in the presence of severe metaphyseal extension or osteopenic bone. Historically, external fixation was the gold standard for maintaining radial length and alignment through ligamentotaxis. However, external fixators are fraught with complications, including pin-tract infections, superficial radial nerve irritation, pin loosening, and complex regional pain syndrome (CRPS).
To circumvent these issues, modern operative orthopaedics has evolved toward advanced internal fixation strategies. Two of the most significant advancements in this realm are Distraction Plate Fixation (the dorsal spanning plate) and Fragment-Specific Open Reduction and Internal Fixation (ORIF). These techniques provide rigid, low-profile stabilization, allowing for immediate postoperative mobilization and facilitating secondary procedures such as structural bone grafting without the physical obstruction of an external frame.
Before exploring these advanced salvage and reconstruction techniques, it is essential to understand the foundational approach to the distal radius, most commonly achieved via volar plating.
VOLAR PLATE FIXATION: THE MODIFIED HENRY APPROACH
While distraction plating is reserved for severe comminution, standard volar plate fixation remains the workhorse for the majority of displaced distal radius fractures. The volar approach utilizes the internervous plane between the flexor carpi radialis (FCR) and the radial artery, providing excellent exposure of the volar cortex while minimizing the risk of dorsal tendon irritation.
Step-by-Step Surgical Technique
The patient is positioned supine with the arm extended on a hand table. A tourniquet is applied to the proximal arm.
-
Incision and Superficial Dissection: A longitudinal incision is made over the course of the FCR tendon, extending proximally from the wrist crease.
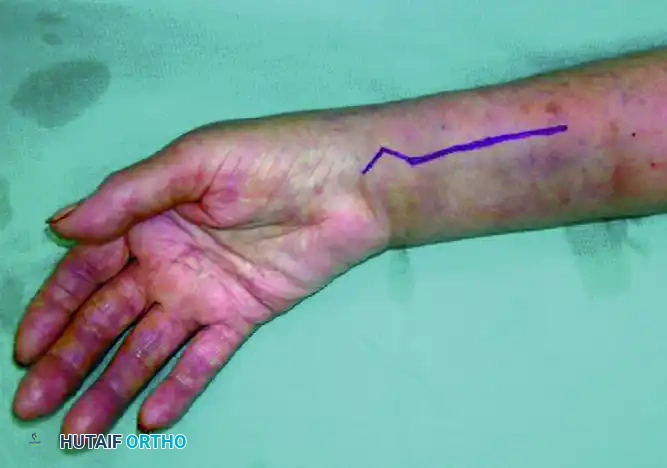
-
FCR Sheath Release: The incision is carried down through the subcutaneous tissue to the FCR sheath. The sheath is incised longitudinally, and the tendon is retracted ulnarly to protect the median nerve.
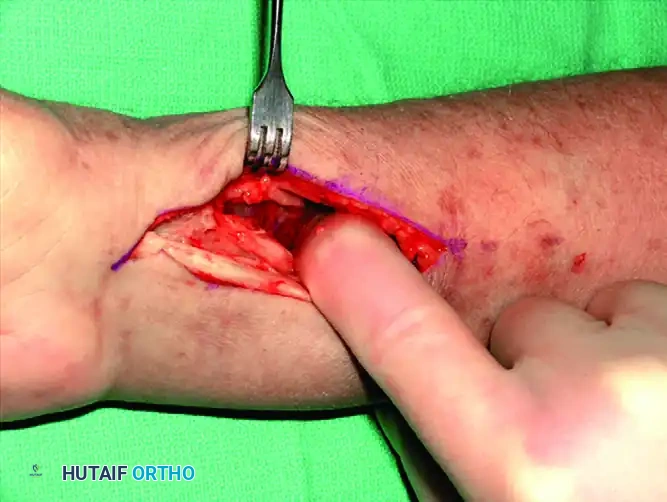
-
Deep Dissection: The floor of the FCR sheath is incised to access the deep compartment. The flexor pollicis longus (FPL) muscle belly is identified and partially detached or retracted ulnarly from the radius to expose the underlying pronator quadratus.
-
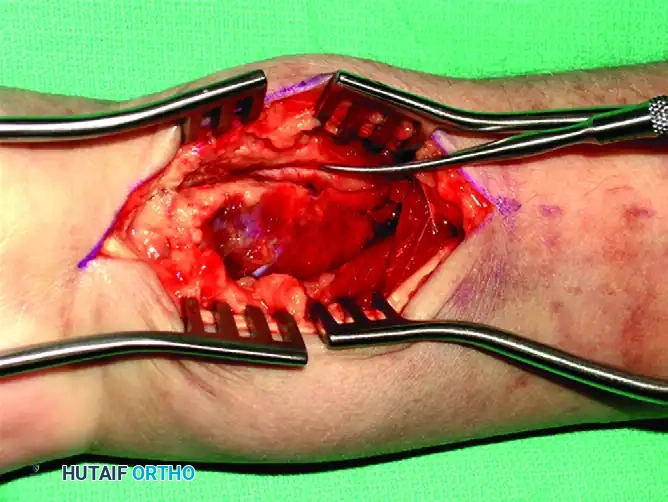
Pronator Quadratus Elevation: Using a Freer elevator or electrocautery, the pronator quadratus is elevated from its radial insertion in an L-shaped fashion, reflecting it ulnarly.
-
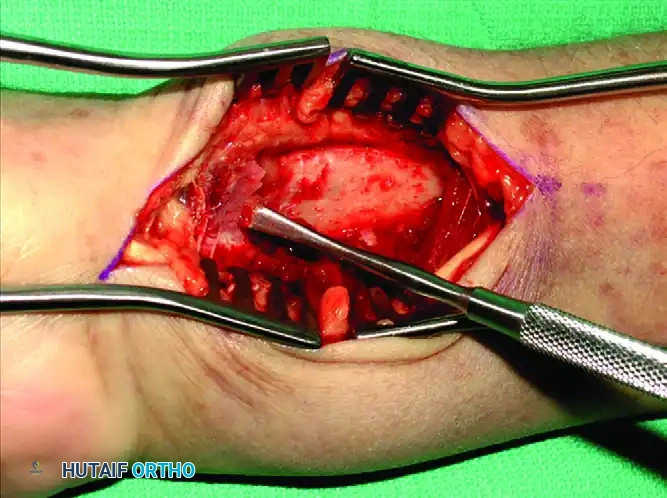
Fracture Exposure and Reduction: The fracture line is now fully exposed. Hematoma is evacuated, and the fracture is reduced under direct vision and fluoroscopic guidance.
-
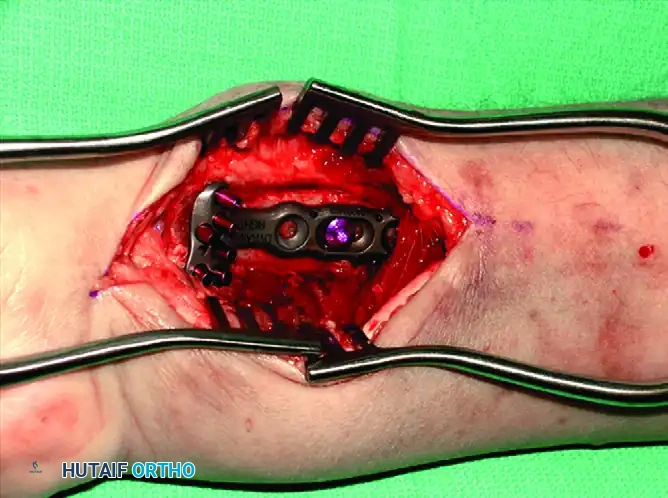
Plate Application: A pre-contoured volar locking plate is positioned proximal to the watershed line to prevent flexor tendon irritation. The first screw is inserted into the elongated gliding hole in the radial shaft to allow for proximal-distal adjustments.

-
Distal Fixation: After confirming restoration of volar tilt and radial inclination, distal locking screws are inserted to support the subchondral bone.
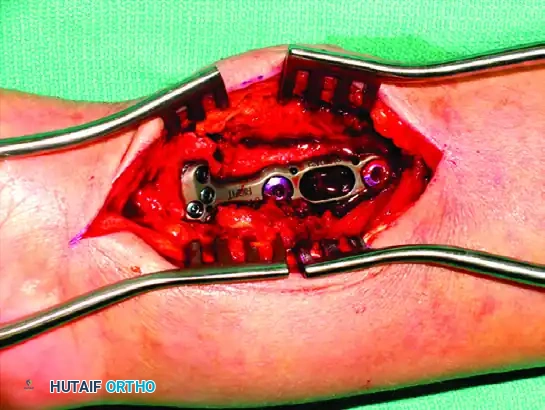
-
Proximal Fixation: The remaining proximal diaphyseal screws are placed to secure the construct.

-
Closure: The pronator quadratus is meticulously repaired and sutured back to the edge of the brachioradialis or radial periosteum to cover the plate and protect the flexor tendons.

🔪 Surgical Warning: Failure to repair the pronator quadratus or placing the plate distal to the watershed line significantly increases the risk of flexor pollicis longus (FPL) tendon rupture due to mechanical attrition against the hardware.
DISTRACTION PLATE FIXATION (DORSAL SPANNING PLATE)
As an alternative to external fixation for highly comminuted fractures of the distal radius, Burke and Singer described the use of a distraction plate as an internal fixator. This technique was later modified and popularized by Ruch et al., who reported good-to-excellent outcomes in 90% of patients.
The distraction plate is applied to the dorsal surface of the hand, wrist, and distal forearm. By spanning the radiocarpal joint, it relies on the principle of ligamentotaxis to restore radial length and alignment. Because the implant is entirely internal, external pin site problems are avoided, and the plate can remain in place as long as necessary for union (typically 12 to 16 weeks). Furthermore, secondary bone grafting procedures are performed much more easily without the physical obstruction of an overlying external fixator frame.
Indications
- Highly comminuted intra-articular distal radius fractures.
- Severe metaphyseal-diaphyseal bone loss.
- Polytrauma patients requiring immediate weight-bearing through the upper extremities (e.g., crutch use).
- Radiocarpal fracture-dislocations.
- Osteoporotic bone where standard locking plates fail to achieve adequate purchase.
Surgical Technique: The Ruch et al. Modification
The procedure utilizes three small incisions to slide a long plate submuscularly, minimizing soft tissue stripping over the fracture site.
1. Distal Incision and Exposure:
Make a 4-cm longitudinal incision over the dorsal aspect of the long finger (third) metacarpal shaft. Expose the bone by carefully retracting the long finger extensor tendon.
2. Proximal Incision and Exposure:
Make a second 4-cm dorsal incision over the radial diaphysis, at least 4 cm proximal to the comminuted segment of the radius. Expose the radial shaft.
3. Middle Incision (Lister's Tubercle):
Make a third 2-cm dorsal incision directly over Lister's tubercle. This exposes the extensor pollicis longus (EPL) tendon and allows for direct visualization of the joint surface if necessary.
4. Plate Tunneling:
Select a 12- to 16-hole, 3.5-mm dynamic compression plate or dedicated spanning plate. Pass the plate from the distal incision in a proximal direction. The plate must glide through the plane between the extensor tendons (specifically the fourth dorsal compartment) and the joint capsule/periosteum. Mobilize the extensor tendons as necessary to ensure the plate sits flat against the bone.
5. Distal Fixation:
Secure the plate to the long finger metacarpal shaft using three bicortical 3.5-mm screws.
6. Distraction and Proximal Fixation:
Under fluoroscopic guidance, apply longitudinal distal traction to the fingers to obtain normal radial length and restore the radiocarpal joint space via ligamentotaxis. With the hand held in approximately 60 degrees of supination, secure the plate to the proximal radius with a bone clamp. Confirm that full rotation of the forearm is possible without impingement. Once confirmed, secure the plate to the radial shaft with three bicortical 3.5-mm screws.
7. Adjunctive Fixation and Grafting:
* Reduce and fix any large diaphyseal fragments to the shaft with interfragmentary lag screws if possible.
* Through the middle incision, elevate the depressed lunate fossa.
* Insert a 3.5-mm screw through the plate and under the elevated lunate fossa to serve as a subchondral buttress.
* Percutaneously pin other intra-articular fragments using Kirschner wires to stabilize the articular surface.
* Place bone graft (autograft, allograft, or synthetic substitute) into the metaphyseal voids through the middle incision.
8. DRUJ Assessment:
Assess the stability of the distal radioulnar joint (DRUJ). If the DRUJ is unstable, immobilize the wrist in a sugar-tong splint postoperatively.
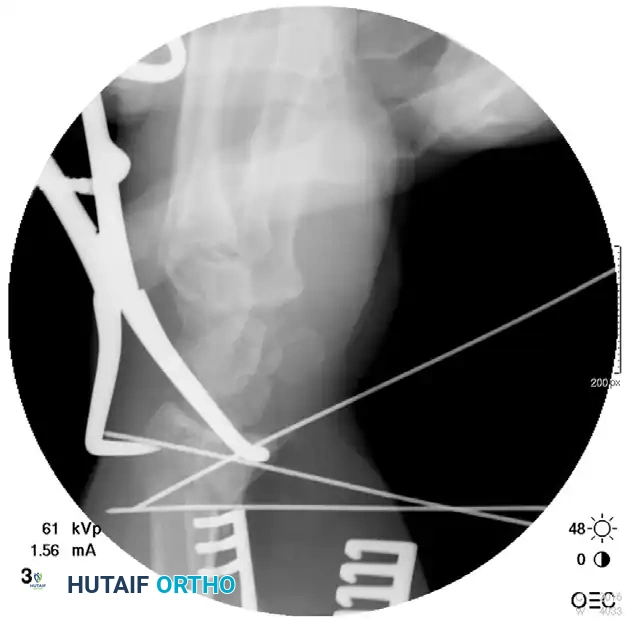
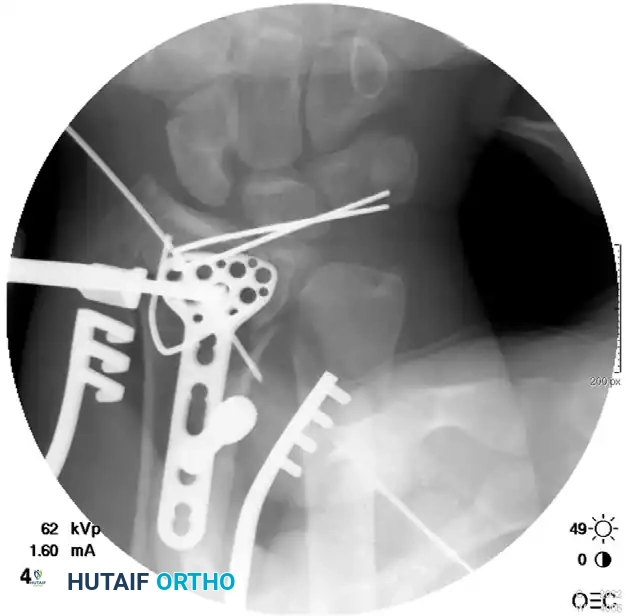
Radiographic Progression of Distraction Plating
The following sequence demonstrates a highly comminuted distal radius fracture successfully managed with a dorsal distraction plate:
Initial Injury Radiographs:



Postoperative Fixation with Distraction Plate:





Postoperative Care for Distraction Plating
Finger, elbow, and shoulder range-of-motion exercises are initiated immediately in the recovery room. If a sugar-tong splint was applied for DRUJ instability, it is removed at 3 weeks. Any percutaneous Kirschner wires used for articular reconstruction are removed at 6 weeks in the clinic. Patients are allowed to perform light activities of daily living, but lifting is strictly restricted to 5 lbs.
Once radiographic union is achieved (typically between 12 to 16 weeks), the distraction plate is surgically removed, and aggressive wrist range-of-motion exercises are commenced.
💡 Clinical Pearl: When applying the distraction plate, ensure the wrist is not fixed in excessive flexion or extension. Neutral extension (0-10 degrees) is preferred to maintain optimal tension on the extrinsic flexor and extensor tendons, facilitating immediate digit mobilization.
FRAGMENT-SPECIFIC OPEN REDUCTION AND INTERNAL FIXATION
Recognizing the biomechanical pitfalls of isolated Kirschner wire fixation and standard plate-and-screw constructs—especially when dealing with highly comminuted intra-articular fractures in osteopenic bone—Medoff developed a comprehensive wrist fixation system. This system (commercialized as the TriMed system) combines the principles of pinning and plating to achieve stable, fragment-specific reconstruction of the distal radius.
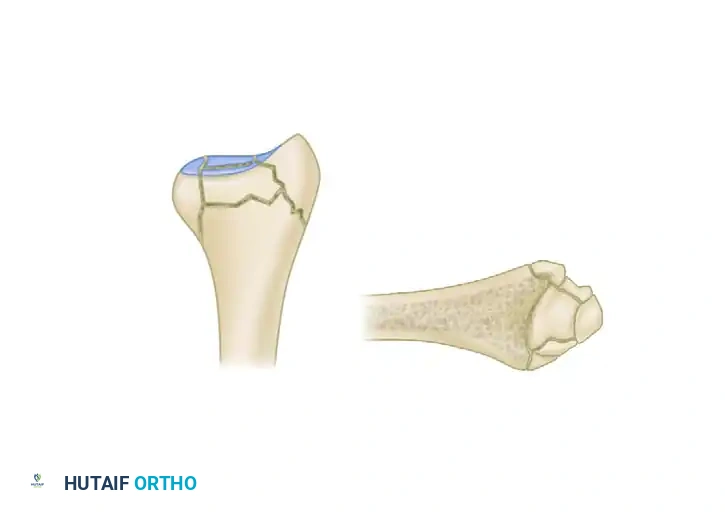
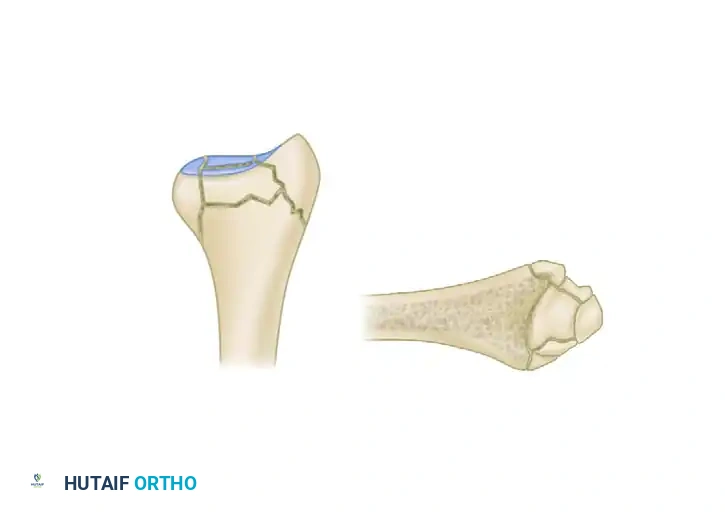
The Five Fracture Fragments
In severe high-energy or osteoporotic distal radius fractures, the bone typically fails in a predictable pattern, resulting in up to five distinct potential fracture fragments:
1. Radial Column (Styloid)
2. Dorsal Cortical Wall
3. Dorsal Ulnar Split
4. Volar Rim (Lunate Facet)
5. Central Intra-articular Fragment



Thin metaphyseal cortical bone does not hold standard screws well. Furthermore, conventional thick plates cannot be applied easily to the dorsal aspect of the distal radius due to the high risk of extensor tendon irritation and eventual rupture. Fragment-specific fixation utilizes low-profile wire-forms and pin-plates to capture these specific fragments without adding excessive bulk.
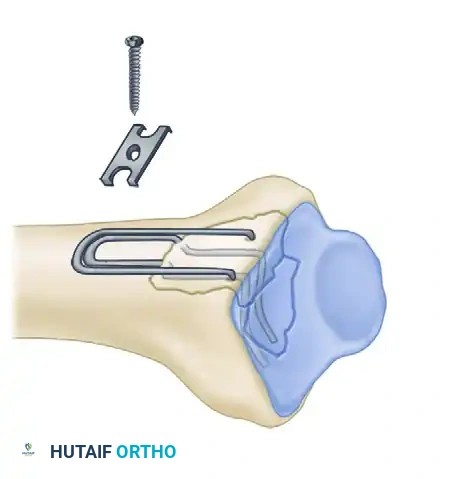
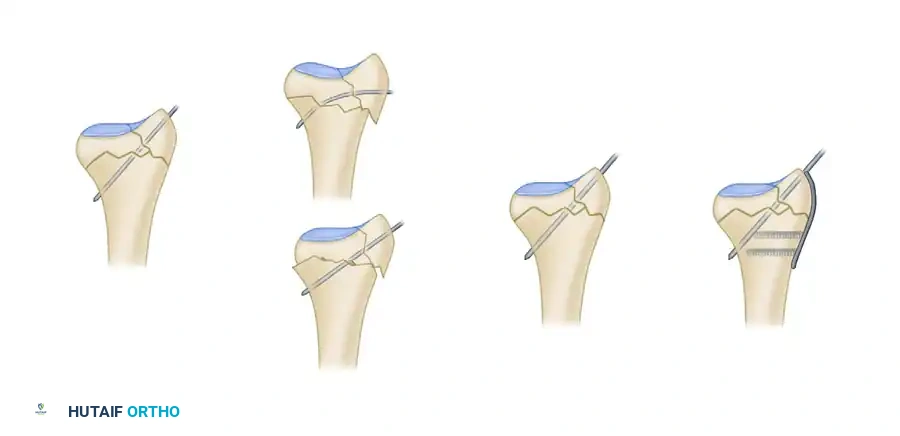
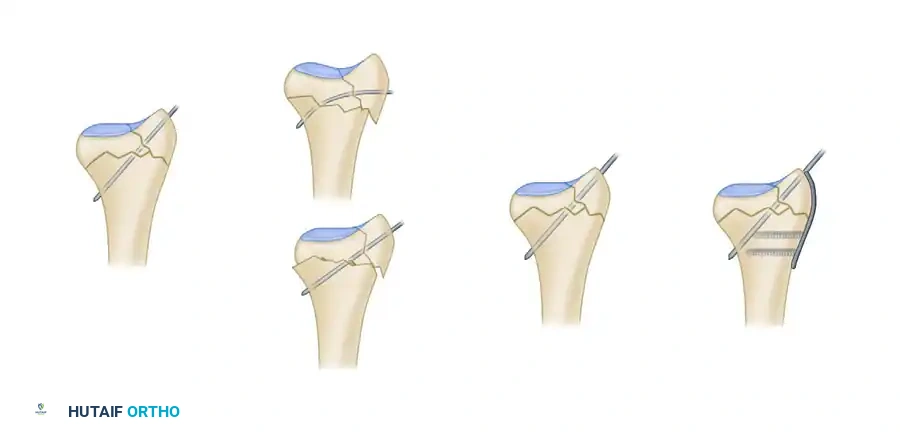
Biomechanics of Pin-Plate Fixation
Traditional radial styloid Kirschner wire fixation provides only a single point of constraint. This single point of fixation acts as a pivot, failing to prevent settling, bending, or radial drift of the distal fragments under physiological loads.
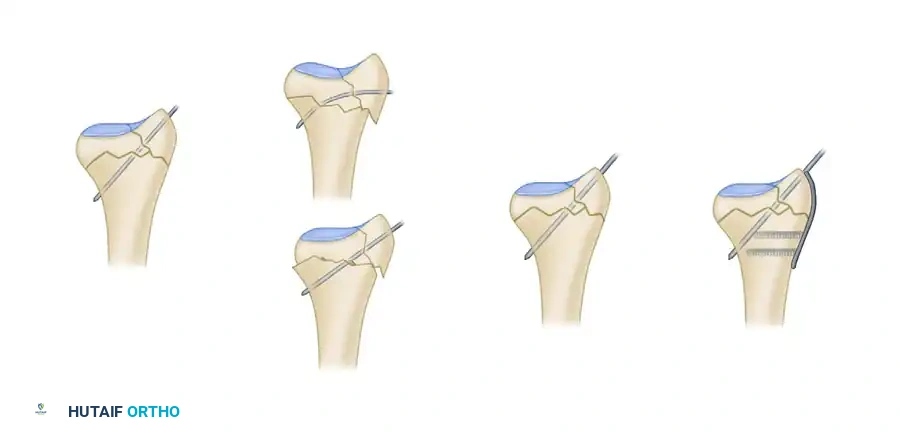
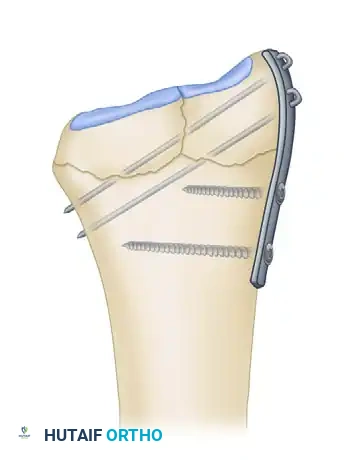
By adding a small buttress plate to the radial styloid pin, the construct is transformed. The pin-plate provides two distinct fixation points: the first through the distal end of the plate, and the second through the intact medial radial cortex. This dual-point constraint prevents collapse, resists dorsal torque, and halts radial migration.
Fragment-Specific Implants and Application
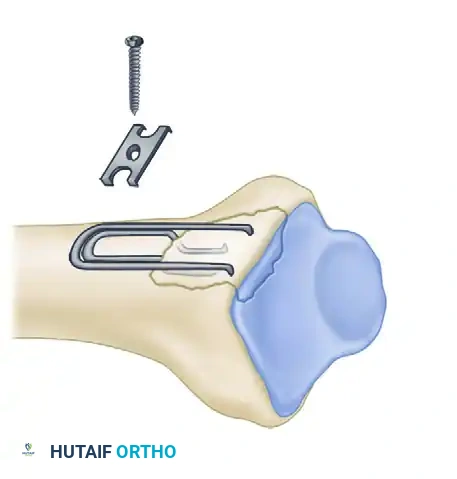
1. The Radial Pin-Plate:
Applied to the radial column, this implant enhances stability by providing a radial buttress. It effectively neutralizes bending forces that would otherwise cause the radial styloid to displace proximally and radially.
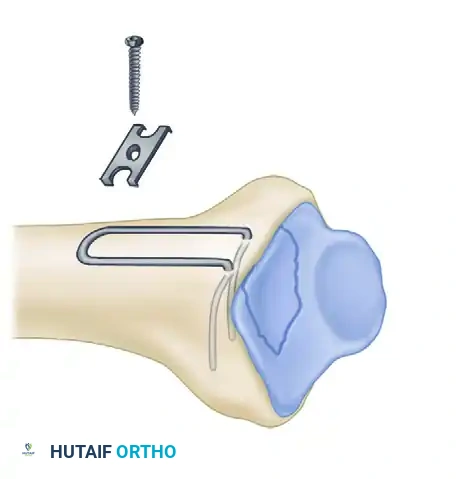
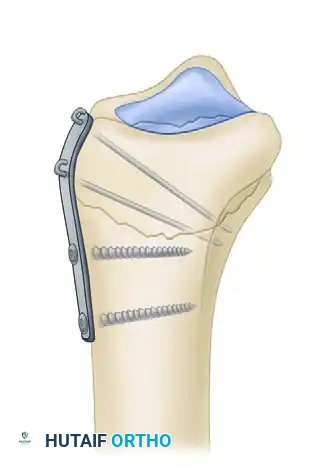
2. The Ulnar Pin-Plate:
The dorsal ulnar fragment (often involving the sigmoid notch) is stabilized with an ulnar pin-plate. By proper contouring, this plate can close gaps in the sagittal plane,
Associated Surgical & Radiographic Imaging