Introduction to Distal Radioulnar Arthrodesis with Distal Ulnar Pseudarthrosis
The distal radioulnar joint (DRUJ) is a critical component of forearm biomechanics, facilitating pronation and supination while transmitting axial loads from the carpus to the forearm. Severe destruction of the DRUJ—whether secondary to rheumatoid arthritis, post-traumatic osteoarthritis, or previously failed surgical interventions—presents a profound reconstructive challenge.
The concept of fusing the DRUJ while intentionally creating a distal ulnar pseudarthrosis to maintain forearm rotation was pioneered independently by Baldwin, Lauenstein, and most notably, Sauvé and Kapandji. Today, the Sauvé-Kapandji procedure remains a cornerstone salvage operation. By arthrodesing the ulnar head to the sigmoid notch of the radius, the procedure effectively restores a stable platform for the carpus, preventing the ulnar translation of the carpus often seen in rheumatoid patients. Simultaneously, the proximal ulnar osteotomy (pseudarthrosis) preserves forearm rotation.
While highly effective at resolving DRUJ pain and providing ulnocarpal support, the procedure's primary historical complication has been the painful instability of the proximal ulnar stump. Consequently, modern iterations of the procedure incorporate complex soft-tissue stabilizations—utilizing the pronator quadratus, flexor carpi ulnaris (FCU), and extensor carpi ulnaris (ECU)—to tether the proximal stump and prevent radioulnar impingement.
Indications and Patient Selection
The Sauvé-Kapandji procedure is indicated as a salvage operation for patients with irreversible DRUJ pathology who require preservation of ulnocarpal support.
Primary Indications
- Rheumatoid Arthritis (RA): Particularly in patients with extensive destruction of the DRUJ, caput ulnae syndrome, and impending or actual ulnar translation of the carpus. The retained ulnar head provides a vital buttress against carpal slide.
- Post-Traumatic Osteoarthritis: Following severe distal radius fractures with intra-articular DRUJ involvement or chronic instability that cannot be reconstructed anatomically.
- Failed Previous Surgery: Salvage of a painful wrist following a failed Darrach procedure (distal ulnar resection), failed hemiresection interposition arthroplasty, or failed ulnar shortening osteotomy.
- DRUJ Incongruity: Secondary to severe premature physeal closure or Madelung's deformity where joint preservation is impossible.
Clinical Pearl:
The Sauvé-Kapandji procedure is generally preferred over the Darrach procedure in younger, higher-demand patients, and in rheumatoid patients with carpal instability, because the arthrodesed ulnar head provides a stable osseous shelf that supports the ulnar carpus and prevents ulnarward carpal subluxation.
Biomechanics and Pathoanatomy
Normal forearm rotation dictates that the radius rotates around a fixed ulna. The DRUJ is stabilized by the triangular fibrocartilage complex (TFCC), the joint capsule, and the dynamic tension of the ECU and pronator quadratus.
When the DRUJ is arthrodesed, the radius and the ulnar head become a single functional unit. Forearm rotation is subsequently transferred to the surgically created pseudarthrosis site proximal to the fusion.
The Challenge of the Proximal Ulnar Stump
The most significant biomechanical consequence of the ulnar osteotomy is the loss of the distal skeletal tether for the proximal ulna. During forceful grip or pronation, the proximal ulnar segment tends to converge toward the radius. If the gap is insufficient or the soft tissues are inadequate, the proximal ulnar stump will dynamically impinge against the radius, causing severe pain, snapping, and a profound feeling of weakness.
To counteract this, modern surgical techniques mandate rigorous soft-tissue stabilization of the proximal stump, utilizing tenodesis to resist dorsal translation and radioulnar convergence.
Preoperative Planning
- Clinical Evaluation: Assess the range of motion, grip strength, and the presence of extensor tendon ruptures (Vaughan-Jackson syndrome), which are common in RA patients and may require simultaneous tendon transfers.
- Radiographic Analysis: Standard posteroanterior (PA) and lateral radiographs of the wrist are mandatory. Evaluate ulnar variance.
- Templating: The length of the ulnar resection depends on the patient's native ulnar variance. In patients with neutral or negative ulnar variance, a 15-mm segment is typically resected. In patients with positive ulnar variance, a larger segment must be removed to allow the ulnar head to be arthrodesed in a neutral position relative to the radius, while still leaving a sufficient 15-mm gap to prevent impingement.
Surgical Technique: The Sauvé-Kapandji Procedure
1. Patient Positioning and Setup
- Position the patient supine on the operating table.
- Apply a well-padded pneumatic tourniquet to the proximal arm.
- Extend the arm on a radiolucent hand table.
- Prepare and drape the limb in a standard sterile fashion to expose the elbow, forearm, and hand.
- Exsanguinate the limb with an Esmarch bandage and inflate the tourniquet (typically to 250 mm Hg).
2. Surgical Approach
The choice of incision depends on the underlying pathology:
* Rheumatoid Patients: Utilize a dorsal longitudinal incision centered over the wrist. This extensile approach allows for a comprehensive extensor tenosynovectomy, evaluation of the extensor compartments, and repair or transfer of ruptured tendons.
* Non-Rheumatoid Patients: Make a dorsoulnar incision centered directly over the ulnar head and DRUJ.
Surgical Warning:
Meticulous dissection is required to identify and protect the dorsal sensory branch of the ulnar nerve (DSBUN), which typically crosses from volar to dorsal approximately 5 cm proximal to the ulnar styloid. Injury to this nerve results in painful neuromas.
- Identify the interval between the extensor carpi ulnaris (ECU) and the extensor digiti minimi (EDM).
- Open the extensor retinaculum. Create a proximal flap based laterally (radially) and a distal flap based medially (ulnarward). Preserve these flaps; they are critical for later reinforcement of the ECU and joint capsule.
3. Joint Preparation and Arthrodesis
- Perform a capsulotomy to expose the DRUJ.
- Using narrow osteotomes, a high-speed burr, and a rongeur, meticulously decorticate the articular cartilage and subchondral bone of both the ulnar head and the sigmoid notch of the radius. Expose healthy, bleeding cancellous bone to ensure a robust arthrodesis.
- Position the ulnar head in the sigmoid notch. Ensure neutral ulnar variance.
- Temporarily stabilize the DRUJ with a 0.045-inch Kirschner wire driven from the ulnar head into the radius.

Diagrammatic representation of the Sauvé-Kapandji procedure demonstrating distal radioulnar arthrodesis and the creation of a pseudarthrosis in the distal ulna.
4. Creation of the Pseudarthrosis (Ulnar Osteotomy)
- Identify the ulnar neck just proximal to the DRUJ capsule.
- Using an oscillating saw under continuous saline irrigation (to prevent thermal necrosis), perform the proximal ulnar osteotomy.
- Measure and resect the appropriate segment of the ulna:
- For neutral/negative variance: Resect a 15-mm segment.
- For positive variance: Resect a larger segment to allow the ulnar head to be shifted proximally (achieving neutral variance at the arthrodesis site) while still maintaining a definitive 15-mm gap.
- Crucial Step: Excise the periosteum surrounding the resected segment completely. Leaving the periosteal sleeve intact highly increases the risk of spontaneous ossification and healing of the pseudarthrosis, which would eliminate forearm rotation and defeat the purpose of the procedure.
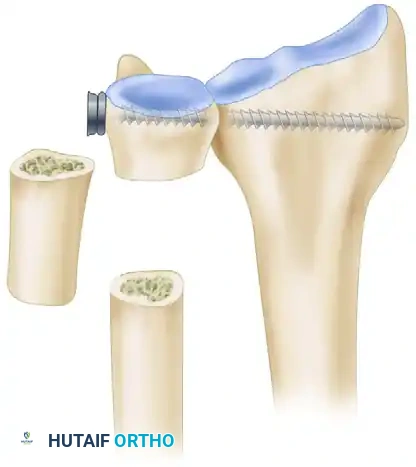
Resected segment of the distal ulna, typically 10 to 15 mm in length. This bone is morselized and utilized as local autograft for the arthrodesis site.
5. Permanent Fixation of the Arthrodesis
- Remove the temporary K-wire.
- Achieve permanent rigid fixation using a 3.5-mm cortical bone screw utilizing a standard lag technique (overdrilling the ulnar head, underdrilling the radius).
- In osteoporotic bone (common in RA), use a washer to prevent the screw head from sinking into the ulnar cortex, or substitute the screw with multiple divergent Kirschner wires.
- Pack the decorticated DRUJ space with the morselized cancellous bone harvested from the excised ulnar segment.
Soft-Tissue Stabilization of the Proximal Ulnar Stump
Instability of the proximal ulna after distal ulnar excision causes profound discomfort, weakness with grasp, and painful clunking during forearm rotation. To mitigate this, several stabilization modifications have been developed. The surgeon must select the appropriate tenodesis based on tissue availability and patient demand.
Modification 1: The Lamey and Fernandez Technique (FCU Tenodesis)
This technique utilizes a distally based slip of the flexor carpi ulnaris (FCU) combined with pronator quadratus interposition.
- Screw Placement Adjustment: To allow for a more distal resection and leave a smaller head-neck segment, use a 3.5-mm cortical screw as the distal lag screw and a 2.7-mm cortical screw for the proximal fixation of the arthrodesis.
- FCU Harvest: Harvest a slip of the FCU tendon, approximately half its width and 8 to 10 cm in length, leaving its distal insertion on the pisiform intact.
- Bone Tunnel Creation: Drill a 4.0- to 4.5-mm hole in the volar cortex of the proximal ulnar segment, approximately 1 cm proximal to the osteotomy site. Direct the drill obliquely from distal to proximal, passing through the medullary canal from dorsal to volar.
- Tendon Routing: Pass the FCU tendon slip through the drill hole from outside the bone, into the medullary canal, and out through the distal end of the osteotomy site.
- Tensioning: With the forearm in neutral rotation and the wrist in neutral flexion-extension, pull the tendon taut and suture it to itself using robust nonabsorbable sutures (e.g., 2-0 Ethibond).
- Pronator Quadratus Interposition: Mobilize the pronator quadratus muscle from the distal segment, transpose it into the 15-mm osteotomy gap, and suture it to the volar aspect of the ECU sheath. This creates a biological spacer that prevents radioulnar convergence.
Modification 2: The Kleinman Salvage Reconstruction (ECU Tenodesis & PQ Transfer)
For severe instability, or as a salvage for a failed Darrach procedure, Kleinman described a robust stabilization utilizing the ECU and the Pronator Quadratus.

Pronator quadratus (white arrows), held by hemostats, is mobilized free from its palmar-medial insertion on the ulna in preparation for interosseous transfer to the dorsomedial aspect of the ulna.
- Pronator Mobilization: The pronator quadratus is carefully elevated from its ulnar insertion, preserving its radial attachment and neurovascular pedicle (anterior interosseous nerve/artery).

A drill hole is created approximately 1.5 cm proximal to the distal end of the proximal ulnar segment, through which the harvested half of the extensor carpi ulnaris (ECU) is passed in preparation for longitudinal tenodesis.
- ECU Harvest and Routing: A distally based slip of the ECU (half-width) is harvested. A transverse drill hole is made in the distal end of the proximal ulnar stump.

Half of the ECU prepared for longitudinal tenodesis of the distal ulna; the free end is reflected distally and anchored to itself under appropriate tension before pronator quadratus transposition.
- Tenodesis Execution: The ECU slip is passed through the ulnar drill hole, reflected back upon itself, and sutured under tension. This longitudinal tenodesis acts as a powerful checkrein against radioulnar impingement.
- PQ Transposition: The mobilized pronator quadratus is then passed through the interosseous space and sutured dorsally. This transfer actively retards dorsal translation of the ulnar stump during pronation.
Modification 3: The Breen and Jupiter Technique
This comprehensive approach incorporates three distinct components:
1. A distally based slip of the FCU tendon.
2. A proximally based slip of the ECU tendon.
3. Dorsal stabilization of the ECU utilizing the previously preserved retinacular flaps.
Clinical Pearl:
Regardless of the specific soft-tissue modification chosen, the retinacular flaps created during the initial exposure should always be utilized to stabilize the ECU tendon dorsally. In rheumatoid patients, volar subluxation of the ECU exacerbates carpal supination and deformity; relocating and stabilizing the ECU dorsally restores its function as a wrist extensor.
Closure and Postoperative Protocol
Closure
- Deflate the pneumatic tourniquet and achieve meticulous hemostasis. Hematoma formation in the pseudarthrosis gap can act as a scaffold for unwanted heterotopic ossification.
- Irrigate the wound copiously to remove any remaining bone debris from the osteotomy.
- Close the subcutaneous tissues and skin with interrupted sutures (e.g., 5-0 nonabsorbable suture for skin).
Postoperative Care
- Immediate Post-Op: Apply a bulky compressive dressing reinforced by a well-molded above-elbow or sugar-tong splint. The forearm is immobilized in neutral rotation to minimize tension on the tenodesis and allow the soft tissues to heal.
- 10 to 14 Days: Remove the skin sutures. Transition the patient to a short-arm cast or a rigid custom thermoplastic splint. If extensive tendon transfers or rheumatoid reconstructions were performed concurrently, longer or more restrictive immobilization may be required.
- 4 Weeks: Discontinue rigid cast immobilization. Transition to a removable wrist splint to be worn for comfort and protection.
- Rehabilitation Phase: Initiate a therapist-supervised rehabilitation program. Begin active and active-assisted range of motion exercises for wrist flexion/extension and forearm pronation/supination.
- 6 to 8 Weeks: Radiographic evaluation to confirm the progression of the DRUJ arthrodesis. Once clinical and radiographic stability is achieved, progressive strengthening exercises are introduced. The wrist is protected with the splint during heavy activities until the arthrodesis is fully consolidated (typically 8 to 12 weeks).
Complications and Management
While the Sauvé-Kapandji procedure is highly reliable, surgeons must be prepared to manage potential complications:
- Nonunion of the Arthrodesis: Occurs in a small percentage of patients, often due to inadequate decortication or poor bone quality. If symptomatic, it requires revision bone grafting and rigid internal fixation (often upgrading from K
