Dislocations and Chronic Volar Instability of the Thumb Metacarpophalangeal Joint
DEFINITIO
Disruption of the restraining structures on the volar surface of the joint between the metacarpal and proximal phalanx of the thumb may result in excessive joint motion and abnormal hyperextension.Often painful, this instability frequently causes significant functional deficits because so much of what humans do with their hands depends on having a stable, pain-free thumb to oppose the other digits.Acute injuries, including joint dislocations, must be treated correctly and promptly to afford the best chance for successful outcomes.Chronic volar instability is seen less often than is collateral ligament incompetence, but it should not be overlooked. It can be treated effectively with a variety of techniques which will be discussed in this chapter.
ANATOMY
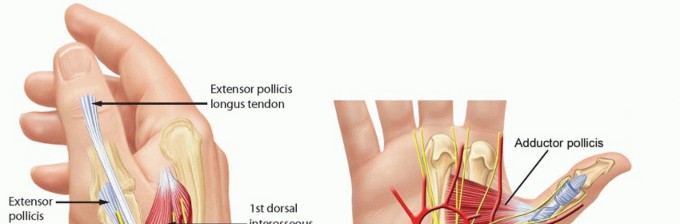


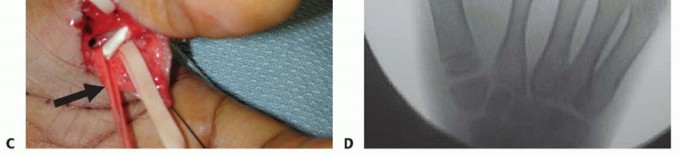
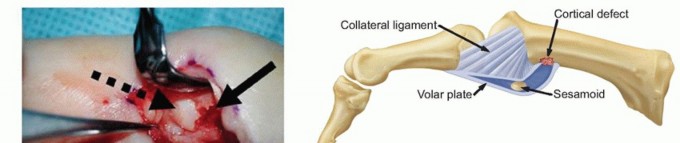
FIG 1 • Anatomy of the thumb MP joint. Thumb MP joint motion varies widely from individual to individual because of the spectrum of metacarpal head geometry seen in “normal” hands.Some metacarpal heads are more rounded and allow greater flexion, extension, and rotation, whereas others are flatter and allow relatively less range of motion (ROM).The joint derives its stability mostly from soft tissue constraints not bony architecture (FIG 1).The proper collateral ligaments originate from the region of the lateral condyles of the metacarpal and pass palmarly and obliquely to insert on the palmar portion of the proximal phalanx.The accessory collateral ligaments originate from the same region but slightly more proximal and traverse distally and palmarly in an oblique fashion to insert on the volar plate and sesamoids.The volar plate serves as the floor of the MP joint. The adductor pollicis (AdP) inserting into the ulnar sesamoid at the distal edge of the volar plate and the insertions of the flexor pollicis brevis (FPB) and abductor pollicis brevis (APB) into the radial sesamoid at the radial distal edge of the volar plate provide additional volar support.The AdP, FPB, and APB also contribute fibers to the extensor mechanism by way of the adductor and abductor aponeuroses and thus provide a modicum of lateral joint stability.P.419Dorsally, the extensor pollicis brevis inserts onto the base of the thumb proximal phalanx and the extensor pollicis longus inserts at the base of the thumb distal phalanx; both traverse the MP joint and add to the stabilizing forces surrounding the joint.The MP joint capsule itself surrounds the joint and contributes slightly to stability.
PATHOGENESIS
Dorsal dislocations of the thumb MP joint are much more common than are volar dislocations.4,5The typical mechanism is a hyperextension force strong enough to rupture the volar plate and joint capsule.For example, dislocations may occur when a ball strikes a player's thumb or when there is a direct blow or fall that drives the proximal phalanx into sudden hyperextension.Occasionally, the radial or ulnar collateral ligaments (or both) of the MP joint are ruptured along with the volar plate. Their treatment is addressed in other chapters.Sometimes, the instability occurs in the setting of a patient with generalized ligamentous laxity such as Ehlers-Danlos syndrome (or other collagen disorders), but in those situations, symptoms are less common and patients typically learn to compensate for the joint laxity.
NATURAL HISTORY
Posttraumatic instability left untreated may result in weakness of pinch and grip and progress to painful arthrosis due to the abnormal biomechanics of the damaged joint.
HISTORY AND PHYSICAL EXAMINATION
In traumatic cases, it is important to inquire about the mechanism of injury.If patients recall which way the thumb was “pointing” at the time of injury, it helps the examiner determine which structures were likely injured.With the ubiquitous presence of cell phone cameras and digital cameras, photos of the deformity right after the injury are often available and can be helpful in confirming the suspected injury.Was the joint dislocated and did it reduce spontaneously or with assistance from a coach, trainer, or the patient?How difficult was the reduction?Physical examination should include an assessment of ROM and grip and pinch strength, particularly in comparison with the contralateral thumb. Focal areas of tenderness should be ascertained. Residual tenderness along the volar plate may persist long after the injury.The examiner should observe the resting joint posture; dislocated joints exhibit obvious deformity.The examiner should check for open wounds and assess the vascular status. Open wounds or vascular compromise mandate emergent treatment.Limited or absent interphalangeal joint ROM suggests flexor pollicis longus tendon entrapment. Dislocated or painful MP joints will have limited ROM.Volar plate stability is assessed because instability must be recognized and treated appropriately to maximize outcomes.Severe collateral ligament injury is uncommon in conjunction with volar plate instability but must be recognized and treated where indicated.An acute dislocation is rarely subtle, but when patients present with chronic instability symptoms, there may be guarding against full joint extension and soft tissue thickening in areas of chronic pathology.
IMAGING AND DIAGNOSTIC STUDIES


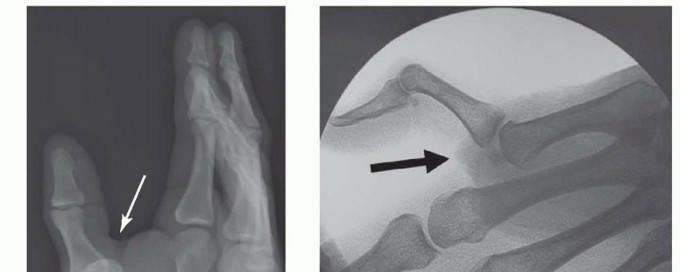
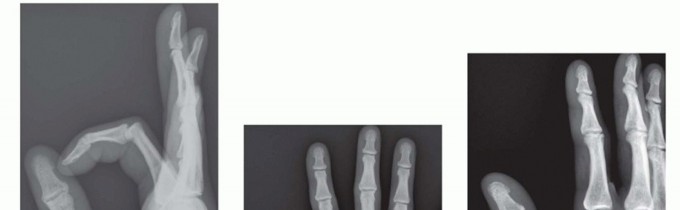
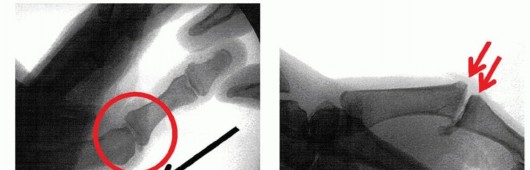
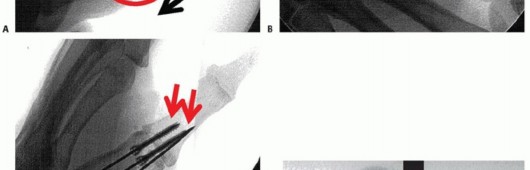
FIG 2 • X-rays showing MP joint dislocation on AP (A) and lateral (B) films. (continued)

DIFFERENTIAL DIAGNOSIS
FractureCollateral ligament injuryLigament laxity, generalized (eg, Ehlers-Danlos syndrome) ArthritisLocked trigger thumb (stenosing tenosynovitis)
NONOPERATIVE MANAGEMENT

SURGICAL MANAGEMENT
Open reduction is required when attempts at closed manipulation and reduction of acute dislocations fail.Failure is typically the result of soft tissue interposition in the joint that blocks reduction. Tissue interposition may have happened at the time of the original injury or as a result of a well-meaning coach, friend, or medical colleague trying to reduce the dislocation by applying vigorous traction, which can cause the soft tissues to become incarcerated.Chronic instability, which is persistently symptomatic despite nonoperative treatment, is best treated with a soft tissue stabilization technique unless moderate to severe arthrosis is present or the instability is global and exceedingly severe. In those cases, arthrodesis is the treatment of choice.
PREOPERATIVE PLANNING
The physician should review all imaging studies. In most cases, those will be limited to plain radiographs and perhaps spot films from fluoroscopic evaluations.Films should be reviewed for any bony abnormalities, especially nondisplaced fractures. One should avoid fracture displacement during intraoperative manipulation of the thumb.In fracture-dislocations of the MP joint, larger fragments are stabilized using Kirschner wires or screws and smaller avulsion-type fragments are excised and the ligament is secured to the bone.For chronic cases, it is important to review the films and rule out osteoarthrosis, which would warrant different treatment strategies.Examination under anesthesia with the assistance of fluoroscopy can be useful to confirm the degree and direction of joint instability.Spot films obtained before and after surgical stabilization can be helpful visual aids for use in postoperative discussions with the patient and his or her family to explain again the nature of the problem and how it was treated.
POSITIONING
The patient should be supine on the operating table with a standard hand table attached and projecting out from the operating table to support the operative hand.A tourniquet should be placed on the operative arm and checked for proper function and pressure before initiation of the surgery (typically 250 or 100 mm Hg greater than systolic blood pressure).
APPROACH
P.422Acute, irreducible MP joint dislocations are best approached from the volar side of the joint so that any soft tissues that may be trapped in the joint can be identified and carefully protected, before they are injured by approaching them “blindly” from the dorsal side.If there is an open wound, it can be incorporated into the surgical incision. A lateral approach is also possible but less often used.Chronic MP joint volar instability that is amenable to soft tissue stabilization should also be approached from the volar aspect of the joint so the pathology can be visualized and addressed directly.If chronic MP joint instability has resulted in arthritis, arthrodesis is a better solution. This may be accomplished in a variety of ways using a variety of hardware options, including screws, plates, and wires. All are best placed through a dorsal approach.
TECHNIQUES
Open Reduction of Acute Metacarpophalangeal Joint Dislocations
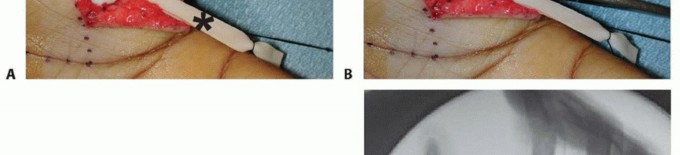
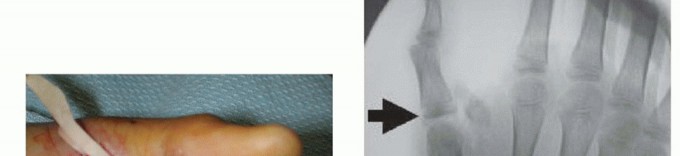
Volar Plate Advancement and Sesamoid Arthrodesis

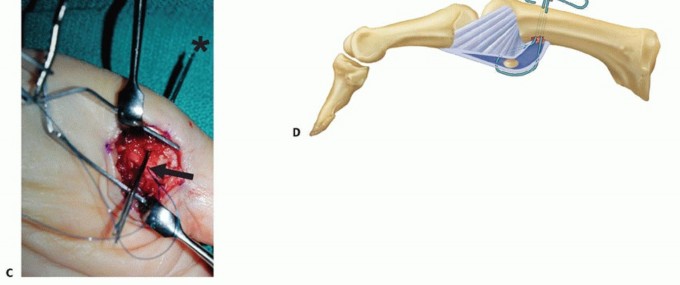
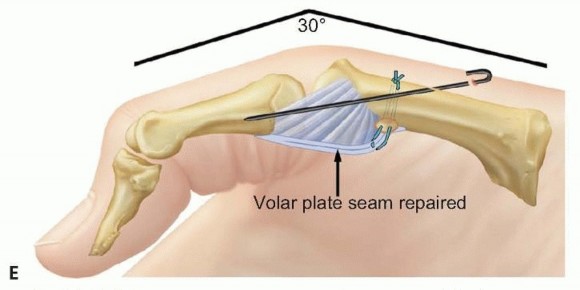
TECH FIG 2 • (continued) E. A Kirschner wire is drilled across the MP joint to keep it flexed 30 degrees, protecting the repaired volar structures during initial healing. VariationsSchuurman and Bos12: Place sutures through the proximal edge of the volar plate and pass them through the metacarpal via the Keith needles. Reinforce the construct with nonabsorbable sutures to local tissue where possible.Eaton and Floyd1: Place sutures in the proximal corner of the volar plate and pass them subperiosteally from volar to dorsal around the metacarpal and secure them to advance the volar plate snugly into the prepared retrocondylar fossa.Pin the MP joint in about 30 degrees of flexion using a Kirschner wire (TECH FIG 2E). Close the wound in routine fashion and apply dressings and a thumb spica splint.Remove the sutures at 10 to 14 days as usual and apply a thumb spica cast.Remove the Kirschner wire and cast at 4 weeks and begin active flexion exercises using a removable protective splint for an additional 2 weeks.
TENDON GRAFT TENODESIS
A procedure used by Littler and cited by Glickel et al3 has been described whereby a free tendon graft (usually the palmaris longus) is woven through drill holes in the proximal phalanx and metacarpal and secured in place to provide a passive restraint against MP joint hyperextension.However, the bulk of soft tissue that results from this procedure and the amount of dissection needed to perform it have caused this operation to fall out of favor.Local tissue mobilization in conjunction with suture anchors provides a better solution.2. Arthrodesis
CANNULATED HEADLESS COMPRESSION SCREW FIXATION

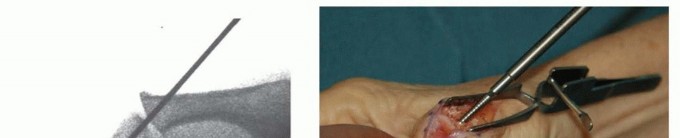
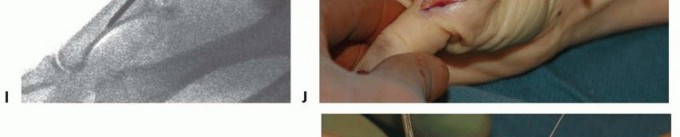

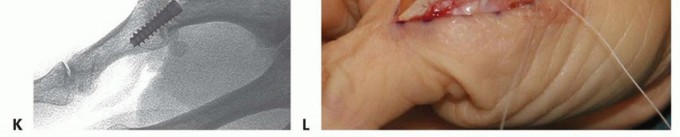
TECH FIG 3 • (continued) I. Its position is checked with fluoroscopy. J. After the proper implant length is measured and the leading cortex overdrilled, the screw is inserted over the guidewire. K. Confirm correct final positioning with fluoroscopy. L. The joint capsule is closed and the extensor mechanism reapproximated. Reconfirm correct alignment in all planes, paying particular attention to rotation. Confirm satisfactory hardware positioning (TECH FIG 3K).Morselized bone graft can be harvested from the resected metacarpal head and packed in and around the arthrodesis site if needed.Close the joint capsule with absorbable suture to minimize extensor tendon adhesions.Approximate the extensor tendon interval with interrupted, inverted permanent suture and close the wound in a routine fashion (TECH FIG 3L).Place a forearm-based thumb spica splint.
DUAL CANNULATED COMPRESSION SCREWS
As an alternative to the technique described earlier using a single compression screw, dual parallel cannulated screws is an alternative (TECH FIG 4A-E).The advantage of using two screws is to better resist rotation and provide additional stability to the construct.The disadvantage is the added cost of the second implant and the increased technical challenge. The surgical steps are the same as those for a single screw, but care is necessary to place the firstguidewire to one side of midline so there is sufficient space to place the second screw in parallel fashion (see TECH FIG 4A-E).
TENSION BAND WIRING


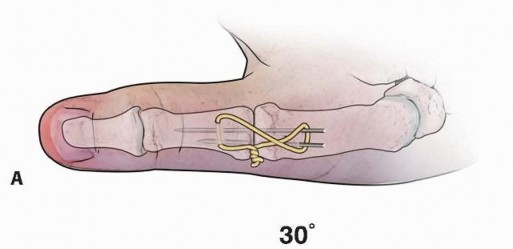
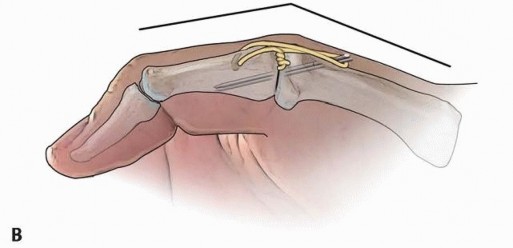
TECH FIG 5 • Tension band wire technique of arthrodesis in AP (A) and lateral (B) projections. Note the presence of the two parallel Kirschner wires, bent over at ends, and the stainless steel wire figure-8 construct.
PLATE AND SCREW FIXATION
It may be desirable to use plate and screw fixation rather than cannulated screws in such cases as nonunion after attempted arthrodesis; failure of implant arthroplasty; and traumatic injuries with severe deformity, bone loss, or segmental defects (TECH FIG 6).The advantage of plates and screws is that more rigid, secure fixation can be achieved immediately, avoiding the concern for rotation or loosening around a single cannulated screw.The disadvantage of that technique is that hardware prominence and tendon irritation and adhesions are more often a source of subsequent trouble.If plate and screw fixation is chosen as the desired technique, then the overall approach and bone preparation are similar to that described for the cannulated screw technique.With the arthrodesis site reduced and temporarily stabilized with a Kirschner wire, a 2.0-mm, five-hole compression plate is contoured to the dorsal surface of the bones.The plate is first secured distally and then applied proximally using compression technique principles.It is critical to avoid long screws and irritation of the flexor pollicis longus.Closure and postoperative care are similar to that described earlier. TECH FIG 6 • Arthrodesis with plate and screw fixation.

Initialtreatment1. Acute MP joint dislocations should be reduced promptly, but straight tractionshould be avoided because it can result in soft tissue entrapment and turn a simple dislocation into a complex, irreducible injury requiring open reduction.2. The joint should be immobilized and protected long enough and rehabilitated carefully enough to avoid chronic volar instability.Treatment ▪ Chronic volar instability without arthritic change can be treated with a variety ofindications capsulodesis procedures.1. When arthritic changes have developed as a result of chronic instability, MP joint arthrodesis should be done.Hardwareproblems1. Cannulated screws work well for MP arthrodesis and leave the hardware buried.2. Plates and screws, Kirschner wire fixation, and transosseous wiring techniques can be effective ways of achieving arthrodesis but are more likely to cause hardware problems requiring subsequent treatment.
PEARLS AND PITFALLS
POSTOPERATIVE CARE
ACUTE DISLOCATION
The MP joint is generally stable once a dislocation is reduced acutely, whether by closed or open methods. The MP joint should be held in about 30 degrees of flexion in a short-arm thumb spica splint or cast for 2weeks.ROM exercises can begin thereafter, using a removable thumb spica splint for an additional 4 weeks, gradually weaning out of the splint and advancing activities as symptoms allow.Supervised hand therapy is often helpful for patients to guide their recovery of motion and strength and optimize their outcomes.
CHRONIC INSTABILITY
Volar plate advancement procedures and the Tonkin sesamoid arthrodesis procedure should be protected with the thumb MP joint flexed in a cast for 4 to 6 weeks, depending on the surgeon's assessment of tissue quality and patientP.429compliance. Then, supervised ROM can begin, but MP joint hyperextension forces should be avoided for 8 to 12 weeks.MP joint arthrodesis procedures require longer protection so that the fusion site is not stressed or disrupted before final bony union.Generally, it is best to use a thumb spica splint (plaster) for the first 10 to 14 days after surgery until the swelling decreases and the sutures are removed.Then a thumb spica cast can be used for an additional 3.5 to 4 weeks, at which time a custom-molded, removable splint can be used to protect the arthrodesis site but allow ROM of the uninvolved adjacent joints of the hand to prevent undue stiffness.By 12 weeks, most arthrodeses are healed solidly enough to allow unrestricted hand use.
OUTCOMES
Acute volar instability and dorsal dislocations of the MP joint that are treated appropriately can beexpected to have a good prognosis.2,3,11 Whether the dislocation is reduced closed or open reduction is required, once the joint is reduced it is usually stable.Following rehabilitation as outlined earlier, there may be some residual joint stiffness. Although that may continue to improve for up to 1 year after injury, the lost ROM is rarely a functional problem.Tonkin et al13 reported successful outcomes in 38 of 42 cases (90%) of sesamoid arthrodeses for chronic MP joint volar instability. Those results compare favorably with outcomes following othercapsulodesis and volar plate reinforcing procedures.6 The advantage of all such procedures is that hyperextension is blocked, restoring stability to the joint, while still allowing the MP joint to flex. Mean loss of flexion compared with the preoperative condition was 8 degrees in the series reported by Tonkin etal.13More recently, Kim et al9 reported excellent results and improved Disability of the Arm, Shoulder, and Hand (DASH) scores in patients treated with sesamoidectomy and volar plate repair using suture anchors.Outcomes after arthrodesis for chronic volar instability must be viewed with the proper surgical goal in mind. The goal is to relieve pain (from instability and arthritic change) and provide stability to the thumb ray. Success rates are high, barring any unfortunate complications as discussed next.
COMPLICATIONS
Complications following MP joint dislocations are uncommon and mostly limited to the sequelae of concomitant soft tissue injuries.Damage to the adjacent neurovascular structures can result from the initial traumatic injury or careless surgical technique at the time of open reduction.Damage to the flexor pollicis longus tendon may occur when it gets trapped in the joint or again when it is manipulated surgically during an open reduction.A complication encountered more often is persistent, chronic instability of the MP joint that results from failure to recognize the nature of the original injury or rehabilitate it properly.Complications after treatment for chronic MP joint volar instability are likewise uncommon and generally related to failure of the chosen procedure.Volar plate advancement can fail due to stretching out over time or a second trauma that causes acute rupture of the repair or sutures.Nonunion of attempted arthrodesis is always a risk, but fortunately, in the small joints of the hand, including thumb MP joints, it is uncommon. Nonunion rates range from 0% to 12% in several reported series.14Hardware causing soft tissue irritation is a potential complication. That can be from superficial pin tract infections in cases where Kirschner wires are used to maintain joint reduction to extensor tendon irritation when fusions are done using plates and screws.
REFERENCES
- Eaton RG, Floyd WE III. Thumb metacarpophalangeal capsulodesis: an adjunct procedure to basal joint arthroplasty for collapse deformity of the first ray. J Hand Surg Am 1988;13(3):449-453.
- Glickel SZ. Metacarpophalangeal and interphalangeal joint injuries and instabilities. In: Peimer CA, ed. Surgery of the Hand and Upper Extremity. New York: McGraw-Hill, 1996:1043-1067.
- Glickel SZ, Barron OA, Catalano LW. Dislocations and ligament injuries in the digits. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Elsevier, 2005: 343-388.
- Gunther SF, Zielinski CJ. Irreducible palmar dislocation of the proximal phalanx of the thumb: case report. J Hand Surg Am 1982;7(5): 515-517.
- Hirata H, Takegami K, Nagakura T, et al. Irreducible volar subluxation of the metacarpophalangeal joint of the thumb. J Hand Surg Am 2004;29(5):921-924.
- Jones DM, Jebsen PJ, Blair WF. Chronic post-traumatic hyperextension instability of the thumb MP joint: results of the volar capsulodesis procedure. Iowa Orthop J 1996;16:122-125.
- Kahler DM, McCue FC III. Metacarpophalangeal and proximal interphalangeal joint injuries of the hand,including the thumb. Clin Sports Med 1992;11:57-76.
- Kijowski R, De Smet AA. The role of ultrasound in the evaluation of sports medicine injuries of the upper extremity. Clin Sports Med 2006;25:569-590.
- Kim BS, Yoon HG, Park KH, et al. Sesamoidectomy and volar plate repair using suture anchor for hyperextension injury of the MP joint of the thumb. Hand Surg 2013;18:287-295.
- Masson JA, Golimbu CN, Grossman JA. MR imaging of the metacarpophalangeal joints. Magn Reson Imaging Clin North Am 1995;3: 313-325.
- Posner MA, Retaillaud JL. Metacarpophalangeal joint injuries of the thumb. Hand Clin 1992;8:713-732.
- Schuurman AH, Bos KE. Treatment of volar instability of the metacarpophalangeal joint of the thumb by volar capsulodesis. J Hand Surg Br 1993;18(3):346-349.
- Tonkin MA, Beard AJ, Kemp SJ, et al. Sesamoid arthrodesis for hyperextension of the thumb metacarpophalangeal joint. J Hand Surg Am 1995;20(2):334-338.
- Weiland AJ. Small joint arthrodesis. In: Green DP, Hotchkiss RN, Pederson WC, eds. Green's Operative Hand Surgery. Philadelphia: Churchill Livingstone, 1999:95-107.
