INTRODUCTION AND PATHOANATOMY
Instability of the lesser metatarsophalangeal (MTP) joints, frequently preceded by chronic synovitis, is a complex and progressive forefoot pathology. The condition is characterized by the gradual attenuation and eventual rupture of the primary static stabilizers of the joint, most notably the plantar plate and the collateral ligament complex.
The plantar plate is a robust, fibrocartilaginous structure composed primarily of type I collagen. It originates from the plantar aspect of the metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. It serves to resist hyperextension forces during the terminal stance phase of gait. When subjected to repetitive microtrauma—often exacerbated by restrictive footwear or altered forefoot biomechanics—the plantar plate undergoes degenerative changes, leading to synovitis, subluxation, and ultimately, a crossover toe deformity.
CLINICAL PRESENTATION AND DIAGNOSIS
Patients with synovitis and instability of the metatarsophalangeal joint usually present with an insidious, slowly progressive course of metatarsalgia. Symptoms are characteristically aggravated by weight-bearing activities and are especially pronounced when wearing high-heeled shoes, which force the MTP joints into sustained hyperextension.
Occasionally, neuritic symptoms may be present in the second web space, with radiation into the second and third toes. This presentation creates a significant diagnostic dilemma.
🚨 CLINICAL PEARL: The Neuroma Trap
It must be emphatically stressed that pain in the second web space is far more likely to originate from MTP joint pathology (synovitis/plantar plate tear) than from an associated interdigital (Morton's) neuroma. Coughlin reported that previous neuroma excision had failed to relieve pain in up to 14% of patients presenting with this specific problem. Misdiagnosis leads to unnecessary nerve resections and delayed treatment of the true mechanical instability.
While the onset is typically chronic, some patients—especially athletes—may recall an acute hyperextension injury (a variant of "turf toe" affecting the lesser digits) that initiated their symptoms.
Physical Examination
Clinical evaluation should begin with an inspection of the patient's standing posture. Look for splaying of the digits, loss of ground purchase by the affected toe, or a frank crossover toe deformity (most commonly the second toe crossing over the hallux).

Clinical presentation demonstrating localized swelling, effusion, and early hammer toe deformity indicative of underlying MTP joint synovitis and instability.
Palpation will often reveal a localized effusion and exquisite tenderness directly over the MTP joint, rather than in the intermetatarsal space. The Lachman test of the MTP joint (dorsal-plantar drawer test) is the gold standard for assessing instability. A positive test is indicated by dorsal translation of the proximal phalanx on the metatarsal head, often accompanied by a palpable "clunk" or reproduction of the patient's pain.
Radiographic and Advanced Imaging
Standard weight-bearing radiographs of the foot (anteroposterior, lateral, and oblique views) are mandatory. Early in the disease process, radiographs may appear entirely normal. As instability progresses, the AP view may show widening of the intermetatarsal space or medial/lateral deviation of the digit.
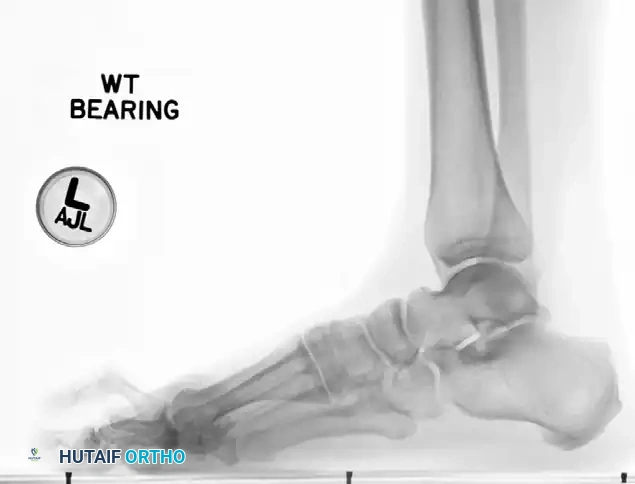
Weight-bearing lateral radiograph of the foot. Note the dorsal subluxation of the proximal phalanx relative to the metatarsal head, a hallmark of advanced plantar plate insufficiency.
When clinical suspicion remains high despite normal radiographs, Magnetic Resonance Imaging (MRI) is the modality of choice. High-resolution MRI, utilizing a small receiver coil, provides excellent visualization of the plantar plate, collateral ligaments, and joint effusion.
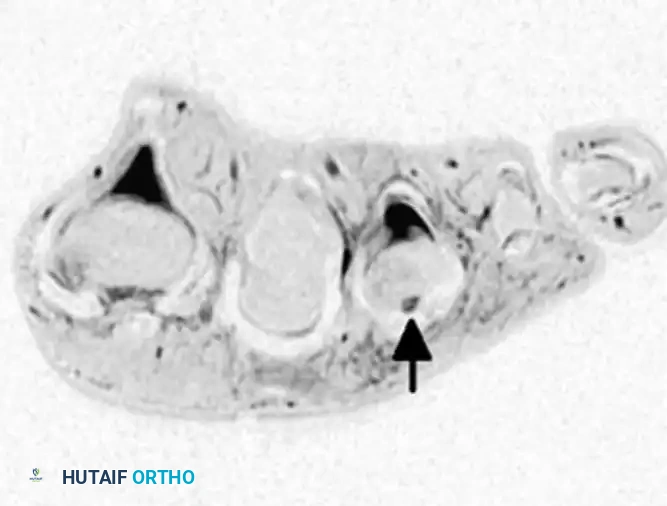
Axial/Coronal MRI utilizing a small receiver coil. The arrow indicates a localized joint effusion and disruption of the lateral collateral ligament complex.
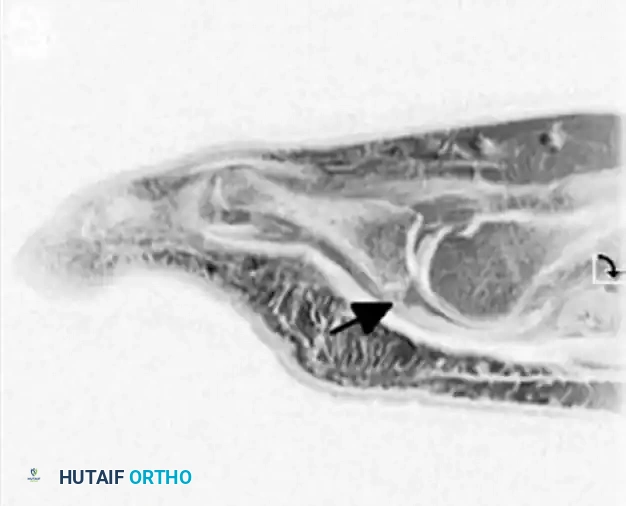
Sagittal MRI demonstrating a high-signal intensity defect at the insertion of the plantar plate into the base of the proximal phalanx, confirming an attritional rupture.
CONSERVATIVE MANAGEMENT
In the early stages of synovitis, when minimal to no deformity is present, aggressive conservative management is highly effective. The goal is to reduce inflammation and mechanically offload the attenuated plantar plate.
- Immobilization and Taping: Taping the toe in a neutral or slightly plantarflexed position (using crossover taping techniques) prevents hyperextension and allows the capsular structures to rest.
- Pharmacotherapy: A single intraarticular corticosteroid injection can be diagnostic and therapeutic, rapidly reducing acute synovitis. This should be used judiciously to avoid further collagen degradation. Oral anti-inflammatory agents (NSAIDs) are also beneficial.
- Orthotics and Footwear Modifications: Metatarsal supports (pads placed proximal to the metatarsal heads) help unload the joint. The use of stiff-soled shoes limits MTP joint dorsiflexion during the propulsive phase of gait. The addition of a spring steel plate to the orthosis, or directly integrated into the sole of the shoe, may help to completely eliminate extension forces on the toe.
When significant deformity or frank instability is present, however, conservative treatment is generally insufficient to provide long-term relief, and surgical intervention is warranted.
SURGICAL TREATMENT STRATEGIES
Surgical decision-making is dictated by the degree of instability, the presence of fixed deformities, and the specific anatomical structures that have failed.
1. Synovectomy and Soft Tissue Balancing (Mild Disease)
For chronic synovitis of the joint that is unresponsive to conservative treatment, but where no significant instability is present (negative dorsal drawer test), a joint-preserving soft tissue procedure is indicated.
Surgical Steps:
1. A dorsal longitudinal incision is made over the affected MTP joint.
2. The extensor digitorum longus (EDL) tendon is identified and lengthened (typically via a Z-lengthening technique).
3. A dorsal capsulotomy is performed to expose the joint space.
4. A meticulous synovectomy is carried out, removing all hypertrophic synovial tissue to relieve capsular distension.
5. Very occasionally, a true second web space neuroma is present concurrently. It should be resected only if preoperative symptoms strongly suggest neuritic pain that is distinct from the mechanical joint pain.
2. Plantar Plate Repair and Joint Stabilization (Moderate to Severe Instability)
If the joint subluxates more than 50% on clinical examination, a stabilizing procedure must be added to the synovectomy. Attritional rupture of the plantar plate has been reported to occur primarily at its distal attachment into the plantar aspect of the proximal phalanx.
Approaches to Plantar Plate Repair:
* Plantar Approach: Direct repair of the plantar plate to the base of the proximal phalanx using a plantar approach provides excellent visualization of the pathology. However, it carries risks of painful plantar scar formation, and no robust long-term outcome studies are currently available to definitively support its superiority.
* Dorsal Approach: Plantar plate repair through a dorsal approach is highly reasonable, although technically tedious. It is currently the favored option in the management strategy of this condition. It typically requires a concurrent Weil osteotomy of the metatarsal to decompress the joint and allow sufficient visualization of the plantar structures. Suture passing devices are used to weave non-absorbable sutures through the torn plantar plate, which are then passed through drill holes in the base of the proximal phalanx.
🔪 SURGICAL WARNING: Plantar Condylectomy
Care should be taken to remove any adherent plantar plate from the plantar surface of the metatarsal head. We have found that, especially if a plantar intractable plantar keratosis (callosity) is present, a plantar condylectomy of the metatarsal head provides a bleeding, cancellous surface for the attachment and healing of the plantar plate. This step provides critical additional static stability to the joint.
3. Tendon Transfers for Dynamic Stability
When static repairs are insufficient or the tissue is too poor to repair, dynamic stabilization is required. Transfer of the flexor tendon to the extensor tendon (the Girdlestone-Taylor procedure) has been highly effective in stabilizing the joint and producing satisfactory long-term results.
Although originally described as a treatment for flexible hammer toes, this procedure is arguably best used for providing dynamic plantarflexion stability to an unstable MTP joint.
Alternatively, flexor-to-extensor transfer or rerouting of the extensor digitorum brevis (EDB) tendon underneath the deep transverse intermetatarsal ligament has been reported to be effective in the treatment of crossover second toe deformities. Transfer of the flexor digitorum longus (FDL) is also a standard technique to restore the plantarflexion vector.
4. Metatarsal Osteotomies
Addressing the bony architecture is often necessary to decompress the joint, reduce tension on the soft tissue repairs, and correct abnormal metatarsal cascade lengths.
The Segmental Osteotomy:
Garg et al. described a modification of the traditional Weil osteotomy—a “segmental” osteotomy—that effectively shortens the metatarsal and reduces the plantar load under the metatarsal head.

Diagram A: The segmental osteotomy technique. Two parallel, oblique dorsal-to-plantar cuts are made in the distal metatarsal metaphysis to remove a precise segment of bone, allowing for controlled shortening.

Diagram B: Following the removal of the bone segment, the capital fragment is translated proximally and secured with a single dorsal-to-plantar compression screw.
While technically easier to perform than the standard Weil osteotomy (which requires a long oblique cut parallel to the weight-bearing surface), the segmental osteotomy has been associated with frequent complications. These include transfer metatarsalgia (due to unpredictable elevation of the metatarsal head), floating toe deformity, infection, and delayed wound healing. Consequently, the traditional Weil osteotomy remains the gold standard for most reconstructive forefoot surgeons.
COMPLEX RECONSTRUCTION AND PATIENT EXPECTATIONS
In cases of severe, rigid crossover toe deformity, a multi-level approach is required. Myerson and Jung reported combining flexor digitorum longus (FDL) tendon transfer with proximal interphalangeal (PIP) resection arthroplasty, PIP fusion, and/or Weil osteotomy of the metatarsal.
While this comprehensive approach addresses all components of the deformity, the complication profile is not insignificant. Although many patients were highly pleased with the pain relief obtained, frequent complications were noted, such as:
* Residual extension contractures at the MTP joint.
* Recurrent medial or lateral deviation of the joint.
* Severe stiffness of the toe (loss of physiological flexion).
These complications resulted in 14% of patients being dissatisfied with the procedure.
🗣️ CLINICAL PEARL: Managing Expectations
It cannot be emphasized enough that with lesser toe surgery, preoperative counseling regarding patient expectations is mandatory. Patients must be explicitly informed that the primary goal of surgery is pain relief and the restoration of a plantigrade foot, not the restoration of a perfectly straight, highly mobile, or cosmetically flawless toe. Postoperative stiffness is an expected outcome of joint stabilization, not a complication.
POSTOPERATIVE PROTOCOL
- Weeks 0-2: The patient is placed in a rigid postoperative shoe or controlled ankle motion (CAM) boot. Weight-bearing is typically restricted to the heel to protect the soft tissue repair and osteotomy sites. The toe is held in a slightly plantarflexed position with compressive dressings.
- Weeks 2-6: Sutures are removed at 14 days. The toe is continuously taped in plantarflexion to protect the plantar plate repair or tendon transfer. Progressive weight-bearing in a stiff-soled shoe is initiated.
-
Weeks 6-12: Taping is discontinued. Active and passive range of motion exercises are initiated, focusing heavily on plantarflexion to prevent dorsal contracture. Return to standard footwear is allowed as swelling permits, though wide-toe-box shoes are recommended indefinitely. High-impact activities and high-heeled shoes are strictly prohibited until at least 4 to 6 months postoperatively.
