Damage Control Orthopaedics: Rescuing a Severely Injured Patient
Introduction & Epidemiology
Damage Control Orthopaedics (DCO) represents a critical paradigm shift in the management of multiply injured patients, particularly those presenting with significant physiological derangement. It emerged as an extension of Damage Control Surgery (DCS) principles from general trauma, recognizing that aggressive, prolonged definitive orthopedic interventions in physiologically unstable patients contribute to a "second hit" phenomenon, exacerbating systemic inflammatory response syndrome (SIRS), multi-organ failure (MOF), and ultimately, mortality. The core tenet of DCO is to perform rapid, life- or limb-saving surgical interventions, temporizing skeletal and soft tissue injuries, to stabilize the patient's physiology before proceeding with definitive reconstruction once hemodynamic stability, normothermia, and coagulopathy are restored.
The epidemiology of polytrauma highlights the necessity of DCO. Severe multiple trauma, often defined by an Injury Severity Score (ISS) greater than 16, remains a leading cause of death and disability worldwide, particularly in younger populations. Blunt trauma, frequently from high-energy mechanisms such as motor vehicle collisions or falls, accounts for the majority of cases. These patients often present with multiple concomitant injuries, including traumatic brain injury (TBI), chest and abdominal trauma, and significant orthopedic injuries. While advances in pre-hospital care, ATLS (Advanced Trauma Life Support) protocols, and critical care have improved early survival, the challenge shifts to preventing late complications and optimizing long-term outcomes. The "lethal triad" of acidosis, hypothermia, and coagulopathy is a hallmark of severe polytrauma and a primary driver for adopting DCO strategies. Early identification of patients at risk for physiological decompensation is paramount in dictating the timing and extent of orthopedic intervention.
Surgical Anatomy & Biomechanics
While DCO prioritizes physiological stabilization over meticulous anatomical reduction in the initial phase, an understanding of surgical anatomy and biomechanics is fundamental for effective temporary fixation and prevention of iatrogenic injury. The objective is to achieve sufficient stability to prevent ongoing hemorrhage, minimize pain, facilitate patient transport and nursing care, and prepare for future definitive reconstruction, all while respecting critical neurovascular structures.
Skeletal Anatomy & Fracture Patterns:
Polytrauma often involves long bone fractures (femur, tibia, humerus), pelvic ring injuries, and complex periarticular fractures.
*
Femur:
Fractures typically involve the diaphysis, often with significant displacement and muscle energy transfer. These are major sources of blood loss.
*
Tibia:
Diaphyseal and pilon fractures are common, frequently associated with open wounds and high risk of soft tissue compromise.
*
Pelvis:
Unstable pelvic ring injuries (e.g., APC II/III, LC II/III, Vertical Shear) are critical, often leading to massive hemorrhage from venous plexuses and arterial sources. They require immediate stabilization.
*
Humerus:
Diaphyseal fractures, while less immediately life-threatening, still require stabilization.
Biomechanics of Temporary Fixation:
The primary goal of DCO fixation is
relative stability
, allowing for soft tissue healing and physiological recovery, as opposed to the
absolute stability
often sought in definitive fixation.
*
External Fixation:
The cornerstone of DCO. External fixators provide rigid or semi-rigid stability by connecting pins inserted into bone segments to an external frame.
*
Pin Placement:
Meticulous attention to safe zones (e.g., anterior-medial aspect of tibia, anterior-lateral aspect of femur) to avoid neurovascular structures (e.g., superficial peroneal nerve, femoral neurovascular bundle).
*
Frame Constructs:
*
Uniplanar:
Simple, rapid to apply, but less stable. Often sufficient for initial stabilization.
*
Biplanar/Multiplanar:
Increased stiffness and stability, potentially allowing for earlier mobilization, but more complex to construct.
*
Bridging vs. Non-bridging:
Bridging joint frames (e.g., knee, ankle) provide excellent stability but limit early joint motion. Non-bridging frames allow for early range of motion if soft tissues permit.
*
Pelvic External Fixation:
Anterior frame placement is common, providing anterior compression and rotational stability for APC-type injuries. Posterior fixation (e.g., iliosacral screws) is definitive but often delayed in DCO.
*
Traction:
Skeletal traction (e.g., distal femoral, proximal tibial) can provide excellent provisional reduction and pain control for long bone fractures, particularly in the femur, serving as a temporizing measure before external fixation or during transport.
*
Splinting:
Simple circumferential splints (e.g., long leg splint, sugar tong splint) are useful for initial transport and can stabilize less complex fractures or those where external fixation is delayed.
The biomechanical principles applied in DCO aim to minimize operative time, blood loss, and physiological stress while providing adequate stability for patient management. The trade-off is often a less-than-perfect anatomical reduction, which is acceptable in the initial phase, with the expectation that definitive surgery will address this.
Indications & Contraindications
The decision to pursue DCO versus Early Total Care (ETC) is complex and multidisciplinary, relying heavily on the patient's physiological status rather than solely on the severity of orthopedic injuries. The overarching goal is to prevent the "second hit" phenomenon.
Indications for Damage Control Orthopaedics (DCO):
The primary indication for DCO is physiological instability or a high risk of developing it. This is often quantified by parameters of the "lethal triad" and overall injury burden.
-
Physiological Derangement:
- Hypothermia: Core body temperature <35°C.
- Acidosis: Base deficit >6 mEq/L or pH <7.24.
- Coagulopathy: INR >1.5, PTT >60s, platelet count <50,000/µL, or active transfusion protocol (e.g., >6 units PRBCs in 24 hours).
- Hemodynamic Instability: Persistent hypotension (SBP <90 mmHg) despite adequate fluid resuscitation, or high-dose vasopressor requirement.
-
High Injury Severity:
- High ISS: Generally >40, but can be lower with specific critical injuries.
- Polytrauma with Multiple Long Bone Fractures: Especially bilateral femur fractures or concomitant pelvic and long bone injuries.
-
Concomitant Life-Threatening Injuries:
- Severe Traumatic Brain Injury (TBI): GCS <8 with intracranial hypertension.
- Severe Thoracic Trauma: Flail chest, pulmonary contusion, ARDS risk.
- Severe Abdominal Trauma: Active intra-abdominal hemorrhage, large retroperitoneal hematoma requiring DCS.
-
Logistical Limitations:
- Mass casualty incidents overwhelming resources.
- Prolonged transport times to definitive care facility.
-
Risk of Local Complications:
- Severe open fractures with extensive contamination requiring serial debridement.
- Limb-threatening vascular injury requiring immediate revascularization, with fracture stabilization as a secondary priority.
- Impending or established compartment syndrome, where fasciotomy is the priority and fracture stabilization is minimal.
Contraindications for Damage Control Orthopaedics:
True contraindications for DCO are rare and generally relate to patients who are physiologically stable and would benefit from ETC. The decision to perform ETC on a seemingly compromised patient should be made cautiously.
- Physiological Stability: Patients who are hemodynamically stable, normothermic, not acidotic, and not coagulopathic are generally candidates for ETC, even with multiple injuries. However, careful monitoring for occult instability or impending decompensation is critical.
- Isolated Fractures: Single-system trauma or isolated fractures that can be definitively treated without significant physiological insult.
- Borderline Stable Patients: These patients represent a "gray zone" where clinical judgment and continuous reassessment are paramount. The trend of physiological parameters (e.g., improving base deficit, decreasing lactate) is often more informative than a single snapshot. A limited definitive procedure (e.g., short intramedullary nail for a femoral fracture) might be considered if it can be performed quickly and safely without exceeding physiological reserves.
Table 1: Operative vs. Non-Operative (DCO vs. ETC) Indications in Polytrauma
| Parameter / Injury | Indications for Damage Control Orthopaedics (DCO - Operative) | Indications for Early Total Care (ETC - Non-Operative, or Definitive Operative) |
|---|---|---|
| Physiological Status | Hypothermia (<35°C), Acidosis (BD >6 or pH <7.24), Coagulopathy (INR >1.5, Plt <50k, massive transfusion) | Normothermic, Normal pH/BD, Coagulation within limits |
| Hemodynamics | Persistent hypotension despite resuscitation, high-dose vasopressor support | Hemodynamically stable, minimal or no vasopressor support |
| Injury Severity Score (ISS) | ISS > 40-50 (or >20-30 with specific critical injuries like severe TBI/chest trauma) | ISS < 20-30 (generally lower risk patients, but not absolute) |
| Traumatic Brain Injury (TBI) | Severe TBI (GCS <8, intracranial hypertension requiring active management) | Mild to moderate TBI (GCS >8, stable intracranial pressure) |
| Chest Trauma | Severe pulmonary contusion, ARDS risk, flail chest, ongoing thoracic hemorrhage | Minor pulmonary contusion, stable chest wall, no respiratory compromise |
| Abdominal Trauma | Active intra-abdominal or retroperitoneal hemorrhage, requiring laparotomy | Stable abdominal injuries, no active bleeding or surgical intervention required |
| Pelvic Ring Injury | Unstable pelvic ring injury with hemodynamic instability (often requiring embolization/packing) | Stable pelvic ring injury or unstable injury in a physiologically stable patient |
| Long Bone Fractures | Multiple long bone fractures (esp. bilateral femur), Open fractures Gustilo IIIB/C with contamination | Isolated long bone fractures, most closed fractures, Gustilo I/II open fractures (if stable patient) |
| Associated Injuries | Limb-threatening vascular injury, impending/actual compartment syndrome | No significant associated limb-threatening injuries |
| Logistics/Resources | Mass casualty, limited OR availability, prolonged transfer | Adequate resources, direct transfer to definitive care |
Pre-Operative Planning & Patient Positioning
Efficient and well-coordinated pre-operative planning is crucial in DCO to minimize operative time and maximize patient safety. This is a multidisciplinary effort involving trauma surgeons, orthopedic surgeons, anesthesiologists, critical care specialists, and nursing staff.
Pre-Operative Planning:
1.
Rapid Assessment & Resuscitation:
Adherence to ATLS principles. Initial assessment focuses on ABCDEs. Aggressive resuscitation for hypovolemic shock, correction of hypothermia, acidosis, and coagulopathy. Massive Transfusion Protocols (MTPs) should be activated early.
2.
Imaging:
Rapid pan-scan (CT head, C-spine, chest, abdomen, pelvis) is often performed upon arrival in the emergency department for initial injury identification. Plain radiographs of suspected extremity injuries are typically sufficient for DCO planning. Angiography may be indicated for pelvic or extremity vascular injuries.
3.
Prioritization of Injuries:
Life-threatening injuries (e.g., active intra-abdominal hemorrhage, severe TBI requiring craniotomy) take precedence. Orthopedic injuries are addressed after immediate life threats are controlled, or concurrently if they are contributing to hemodynamic instability (e.g., unstable pelvic fracture).
4.
Team Briefing:
A concise pre-operative briefing with the entire surgical team (anesthesia, nursing, residents, attending surgeons) to outline the expected injuries, planned procedures (e.g., external fixation of bilateral femurs and pelvis, fasciotomies), potential challenges, and estimated operative time. This ensures everyone is on the same page.
5.
Equipment Preparation:
All necessary external fixation components, pin insertion kits, fasciotomy trays, and wound care supplies should be readily available and opened. C-arm fluoroscopy must be functional and draped.
6.
Blood Products:
Ensure adequate blood products (PRBCs, FFP, platelets, cryoprecipitate) are in the operating room or immediately accessible.
7.
Surgical Site Preparation:
Broad-spectrum antibiotics administered within one hour of incision. Skin preparation should be wide, covering potential future incisions for definitive fixation if possible, recognizing the need for speed.
Patient Positioning:
Patient positioning in DCO is designed for rapid access to multiple injury sites and efficient external fixation application, often in a supine position on a radiolucent operating table.
*
Supine Position:
This is the most common position for DCO procedures. It allows for simultaneous access to the chest, abdomen, pelvis, and all four extremities, facilitating multidisciplinary trauma surgery.
*
Radiolucent Operating Table:
Essential for fluoroscopic guidance during external fixator pin placement and fracture reduction. Avoid traction tables initially, as they are time-consuming to set up and may hinder access to other injury sites.
*
Extremity Exposure:
Injured extremities are prepared and draped to allow for full range of motion at proximal and distal joints, which aids in reduction maneuvers.
*
Pelvic Stabilization:
For unstable pelvic fractures, initial external compression with a sheet or commercial binder is applied in the emergency department. In the OR, this can be maintained, and a definitive external fixator (e.g., anterior frame) can be applied. The patient may require slight Trendelenburg position to improve venous return and facilitate central venous access if not already established.
*
Spinal Positioning:
If spinal injuries are suspected or confirmed, meticulous log-rolling techniques and maintenance of spinal precautions (e.g., cervical collar, backboard if not contraindicated for other reasons) are critical during transfer and positioning.
The entire process, from patient arrival to skin incision, must be streamlined to minimize the "golden hour" and provide timely intervention for life- and limb-threatening injuries.
Detailed Surgical Approach / Technique
The surgical approach in DCO focuses on speed, simplicity, and effectiveness in achieving temporary stability while minimizing physiological insult. Definitive anatomical reduction is deferred.
General Principles:
1.
Hemostasis First:
Address any active bleeding, whether from the fracture site, soft tissues, or elsewhere.
2.
Debridement & Contamination Control:
For open fractures, perform rapid, thorough debridement of contaminated and devitalized tissue. Irrigation with copious amounts of saline. Temporary wound closure (e.g., vacuum-assisted closure, sterile dressings) to prevent further contamination and desiccation.
3.
Reduction & Stabilization:
Achieve an acceptable reduction (length, alignment, rotation) that allows for adequate temporary fixation. This does not need to be anatomical.
4.
Minimally Invasive:
Prioritize approaches that minimize soft tissue dissection and operative time.
Specific Techniques:
1. Pelvic External Fixation
For unstable pelvic ring injuries, particularly those involving anterior-posterior compression (APC II/III) or lateral compression with vertical instability components.
*
Patient Positioning:
Supine on a radiolucent table.
*
Anterior Superior Iliac Spine (ASIS) Pin Placement:
*
Incision:
Small stab incisions (1-2 cm) are made 2 cm posterior and 2 cm superior to the ASIS. This entry point targets the thickest part of the iliac crest for better purchase and avoids the lateral femoral cutaneous nerve and abdominal contents.
*
Dissection:
Blunt dissection down to the outer table of the ilium.
*
Pin Insertion:
A threaded 5 or 6 mm Schanz pin (or similar) is inserted manually or with a power driver, aiming for the dense cancellous bone of the iliac crest. The pin should be directed posteriorly and medially, parallel to the plane of the iliac wing, ensuring full bicortical purchase without violating the inner table or abdominal cavity.
*
Confirmation:
Fluoroscopy (inlet/outlet views) confirms pin placement.
*
Frame Construction:
* Connect the pins with external fixation bars and clamps. A simple, triangular or quadrilateral frame across the anterior pelvis provides excellent rotational stability.
*
Reduction:
Compression can be applied to the frame to help reduce the anterior ring injury.
*
Pitfalls:
Inadequate pin purchase, iatrogenic injury to lateral femoral cutaneous nerve, bowel or vascular perforation (rare if correct technique followed).
2. Femoral External Fixation
Primarily for diaphyseal femoral fractures, especially in open injuries or severely unstable patients.
*
Patient Positioning:
Supine on a radiolucent table. Traction may be applied manually or with a femoral distractor to achieve length and alignment.
*
Pin Placement (Proximal Segment):
*
Entry:
Lateral aspect of the proximal femur, typically 2-3 cm distal to the greater trochanter, avoiding the tensor fascia lata.
*
Insertion:
Schanz pin is inserted through a small stab incision, directed medially and slightly anteriorly, aiming for bicortical purchase. Avoid excessively anterior placement to prevent neurovascular injury and posterior placement to avoid sciatic nerve.
*
Safe Zone:
Typically the anterior-lateral aspect of the femur.
*
Pin Placement (Distal Segment):
*
Entry:
Lateral aspect of the distal femur, 15-20 cm proximal to the knee joint line.
*
Insertion:
Similar technique, ensuring bicortical purchase. Avoid violating the quadriceps tendon or articular surface.
*
Frame Construction:
Connect pins with bars, typically in a uniplanar or biplanar fashion. Apply gentle distraction or compression to achieve acceptable length, alignment, and rotation.
*
Image:
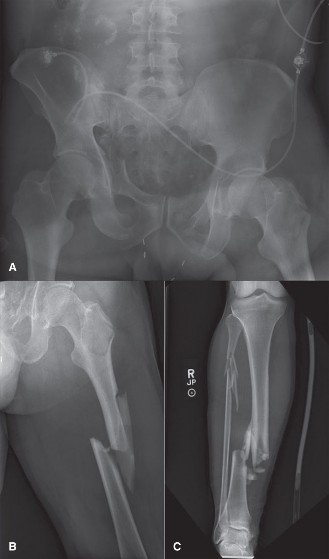
Figure 1: Example of a unilateral external fixator construct applied to a long bone, typical of a Damage Control Orthopaedics strategy. Note the strategically placed Schanz pins and connecting bars providing immediate stabilization.
*
Pitfalls:
Neurovascular injury (e.g., femoral nerve/vessels proximally, popliteal vessels distally), inadequate reduction, loosening/infection of pins.
3. Tibial External Fixation
Common for open tibial fractures, pilon fractures, or tibia diaphyseal fractures in polytrauma.
*
Patient Positioning:
Supine on a radiolucent table. Manual traction or a femoral distractor can be used.
*
Pin Placement (Proximal Tibia):
*
Entry:
Anteromedial aspect of the tibia, approximately 2 cm distal to the tibial tuberosity, ensuring clearance from the patellar tendon.
*
Insertion:
Directed posterolaterally to achieve bicortical purchase. Avoid posterior structures (e.g., popliteal neurovascular bundle, common peroneal nerve laterally).
*
Pin Placement (Distal Tibia):
*
Entry:
Anteromedial aspect of the tibia, 2-3 cm proximal to the ankle joint, avoiding the extensor tendons and neurovascular bundle.
*
Insertion:
Directed posterolaterally.
*
Frame Construction:
Uniplanar or biplanar frame, often extending across the ankle joint (bridging) for severe pilon or distal tibia fractures.
*
Pitfalls:
Pin site infection, neurovascular injury (e.g., superficial peroneal nerve if pins are placed too laterally in the distal leg), compartment syndrome if not recognized.
4. Humeral External Fixation
Less common, but useful for highly comminuted, open, or pathologically fractured humeri in unstable patients.
*
Patient Positioning:
Supine or beach chair position, with the arm draped free.
*
Pin Placement:
*
Proximal:
Anterolateral aspect of the humerus, distal to the deltoid insertion.
*
Distal:
Anterolateral aspect of the humerus, proximal to the olecranon fossa.
*
Care:
Extreme caution to avoid radial nerve (spirals posterolaterally), axillary nerve (around surgical neck), and brachial artery/median nerve (medial aspect).
*
Frame Construction:
Uniplanar frame.
*
Pitfalls:
Radial nerve palsy, pin site infection, inadequate stability for early mobilization.
5. Fasciotomy
Essential for management of actual or impending compartment syndrome, often performed during the initial DCO surgery or shortly thereafter.
*
Indications:
Clinical signs (pain out of proportion, pain with passive stretch, tense compartment) or measured compartment pressures >30 mmHg (or ΔP <30 mmHg).
*
Technique (Lower Leg):
*
Two-Incision Technique:
Anterolateral incision for anterior and lateral compartments; posteromedial incision for superficial and deep posterior compartments.
*
Excision:
Meticulous release of all fascia longitudinally.
*
Wound Management:
The skin and subcutaneous tissue are left open. Temporary closure options include sterile dressings, negative pressure wound therapy (NPWT), or vessel loops/sutures for gradual approximation. Definitive closure is typically delayed.
*
Pitfalls:
Incomplete fasciotomy, iatrogenic nerve/vascular injury, wound infection, skin necrosis.
6. Temporary Wound Management
For open fractures or fasciotomy sites, definitive soft tissue coverage is delayed.
*
Options:
Sterile dressings, wet-to-dry dressings, vacuum-assisted closure (VAC) systems, sterile impermeable dressings.
*
Goals:
Prevent desiccation, control infection, manage exudate, prepare for delayed definitive closure or reconstruction.
The DCO technique is not a one-size-fits-all approach but rather a set of principles applied with judgment, aiming to buy time for the patient to recover physiologically before undergoing more demanding definitive orthopedic procedures.
Complications & Management
Complications associated with DCO can be broadly categorized into systemic and orthopedic, often stemming from the patient's underlying physiological compromise and the nature of temporary fixation. Proactive recognition and management are critical.
Systemic Complications:
These are often related to the initial trauma and the "second hit" phenomenon, potentially exacerbated if DCO principles are not strictly adhered to.
*
Systemic Inflammatory Response Syndrome (SIRS) / Sepsis:
*
Incidence:
High in polytrauma patients (up to 30-50% for SIRS), sepsis varies depending on initial injury severity and infection control.
*
Management:
Aggressive critical care support, early recognition and treatment of infection sources, appropriate antibiotics, maintenance of physiological stability. Adherence to DCO principles helps mitigate SIRS.
*
Acute Respiratory Distress Syndrome (ARDS):
*
Incidence:
10-20% in severe trauma patients, especially with chest injuries.
*
Management:
Lung-protective ventilation strategies, prone positioning, fluid balance optimization. Avoiding the "second hit" by delaying definitive surgery reduces ARDS risk.
*
Multi-Organ Failure (MOF):
*
Incidence:
Directly correlates with injury severity and physiological derangement.
*
Management:
Comprehensive critical care, support for failing organ systems, aggressive infection control.
*
Venous Thromboembolism (VTE - DVT/PE):
*
Incidence:
High in trauma (DVT 10-60%, PE 1-10%), especially with lower extremity and pelvic injuries.
*
Management:
Early chemical prophylaxis (once safe from bleeding), mechanical prophylaxis (compression devices), early mobilization.
*
Fat Embolism Syndrome (FES):
*
Incidence:
0.5-2% in long bone fractures, higher with multiple fractures.
*
Management:
Supportive care, prevention by early stabilization of long bone fractures (even if temporary).
Orthopedic Complications:
These are often directly related to the temporary nature of DCO fixation or inadequate initial management.
*
Pin Site Infection:
*
Incidence:
Common, ranging from 5-20% for superficial infections to 1-5% for deep infections/osteomyelitis.
*
Management:
Meticulous pin care, oral antibiotics for superficial infections, IV antibiotics for deeper infections, pin removal/exchange if osteomyelitis develops. Prophylactic antibiotics are given during insertion.
*
Nonunion/Malunion:
*
Incidence:
Higher in DCO due to delayed definitive fixation and less precise initial reduction (can be 5-15% or more depending on fracture).
*
Management:
Requires definitive surgical intervention with anatomical reduction, rigid fixation, and potentially bone grafting. Pre-operative planning for definitive fixation should account for potential malalignment.
*
Neurovascular Injury (Iatrogenic):
*
Incidence:
Rare (<1%), but devastating. Can occur during pin insertion (e.g., radial nerve, peroneal nerve, major vessels).
*
Management:
Prevention through careful anatomical knowledge and fluoroscopic guidance. Immediate surgical exploration and repair if injury is suspected.
*
Compartment Syndrome (Missed or Recurrent):
*
Incidence:
Varies widely, high index of suspicion in trauma.
*
Management:
Prevention by liberal use of fasciotomy based on clinical suspicion or objective measurements. If missed, emergent fasciotomy, potentially with muscle necrosis and functional loss.
*
Deep Wound Infection (Open Fractures):
*
Incidence:
High in severe open fractures (Gustilo III: 10-50%).
*
Management:
Aggressive serial debridement, appropriate antibiotics, delayed primary closure, negative pressure wound therapy, muscle flap coverage.
*
Implant Failure (External Fixator):
*
Incidence:
Variable, due to loosening, bending, or breakage of pins/bars.
*
Management:
Revision of the fixator, replacement of components, or proceeding to definitive fixation if physiological status allows.
*
Stiffness/Contracture:
*
Incidence:
Common around joints bridged by external fixators or in limbs with extensive soft tissue injury.
*
Management:
Early and aggressive rehabilitation once definitive fixation is in place. If fixator bridges a joint, consider removing it or converting to non-bridging if stability allows.
Table 2: Common Complications in Damage Control Orthopaedics (DCO)
| Complication | Incidence (Approximate) | Salvage Strategies / Management Principles |
|---|---|---|
| Systemic: | ||
| SIRS / Sepsis | 30-50% / Varies | Critical care, infection source control, antibiotics, physiological optimization |
| ARDS | 10-20% | Lung-protective ventilation, prone positioning, fluid management, mitigate "second hit" |
| MOF | Varies with ISS | Multidisciplinary critical care, organ support, infection control |
| VTE (DVT/PE) | DVT 10-60%, PE 1-10% | Early chemical/mechanical prophylaxis, early mobilization |
| Orthopedic: | ||
| Pin Site Infection | 5-20% (superficial) | Meticulous pin care, oral/IV antibiotics, pin removal/exchange if deep |
| Nonunion / Malunion | 5-15%+ | Definitive fixation with anatomical reduction, bone grafting, osteotomy |
| Iatrogenic Neurovascular Injury | <1% | Prevention (anatomical knowledge, fluoroscopy), emergent exploration/repair |
| Missed Compartment Syndrome | Variable | High index of suspicion, emergent fasciotomy, close monitoring |
| Deep Wound Infection (Open Fractures) | 10-50% (Gustilo III) | Serial debridement, antibiotics, NPWT, delayed closure, flap coverage |
| Implant Failure (External Fixator) | Variable | Revision of fixator, component replacement, conversion to definitive fixation |
| Joint Stiffness / Contracture | Common | Early rehabilitation post-definitive fixation, consider early fixator removal if stable |
Post-Operative Rehabilitation Protocols
Rehabilitation in DCO is a phased process, closely mirroring the patient's physiological and orthopedic recovery. It emphasizes early mobilization within the constraints of temporary fixation to prevent secondary complications of immobility, followed by more aggressive, fracture-specific rehabilitation after definitive fixation.
Phase 1: Damage Control Phase (Temporary Fixation)
This phase begins immediately post-DCO surgery and continues until the patient is physiologically stable enough for definitive orthopedic reconstruction. The focus is on preventing systemic complications and maintaining limb viability.
*
Goals:
* Prevent pulmonary complications (atelectasis, pneumonia).
* Prevent deep vein thrombosis (DVT) and pressure ulcers.
* Maintain joint range of motion (ROM) in uninjured or unbridged joints.
* Minimize muscle atrophy.
* Control pain.
*
Mobility:
*
Early Bed Mobility:
Frequent repositioning, log-rolling (if spinal precautions).
*
Out-of-Bed Mobilization:
As soon as physiologically stable, patients should be assisted to a chair. This improves respiratory mechanics, bowel function, and reduces pressure ulcer risk.
*
Weight-Bearing Restrictions:
Strict non-weight-bearing (NWB) on injured extremities with external fixators. Upper extremity injuries may allow limited, protected ROM.
*
Physical Therapy (PT) / Occupational Therapy (OT):
*
Respiratory Therapy:
Incentive spirometry, deep breathing exercises, coughing.
*
Active-Assistive / Passive ROM:
For all uninjured joints. For joints with bridging external fixators, ROM is typically limited until the fixator is removed or converted, but gentle passive motion may be initiated if the fixator design allows (e.g., dynamic external fixators).
*
Strengthening:
Isometric exercises for muscles that do not cross the fracture site.
*
Functional Mobility:
Transfer training (bed to chair), balance exercises in sitting.
*
Pain Management:
Multimodal analgesia to facilitate early mobilization and patient comfort.
*
Pin Care:
Daily pin site cleaning as per institutional protocol to prevent infection.
Phase 2: Definitive Fixation Phase
Once the patient is physiologically optimized (typically 3-14 days post-initial DCO), temporary fixation is converted to definitive internal fixation (e.g., intramedullary nail, plate and screws). Rehabilitation protocols then become specific to the type of fracture and definitive fixation.
*
Goals:
* Achieve full, pain-free joint ROM.
* Restore muscle strength and endurance.
* Regain functional independence.
* Promote fracture healing.
*
Progression:
*
Weight-Bearing:
Progressed based on fracture stability, type of fixation, and fracture healing (e.g., touch-down weight-bearing, partial weight-bearing, full weight-bearing). Radiographic evidence of healing guides progression.
*
ROM:
Aggressive active and passive ROM exercises, often with therapist assistance. Scar tissue mobilization.
*
Strengthening:
Progressive resistance exercises, targeting specific muscle groups, core strengthening.
*
Proprioception and Balance:
Neuromuscular re-education, balance boards, single-leg stance.
*
Gait Training:
Progression from assistive devices (walker, crutches) to independent ambulation.
*
Functional Activities:
Tailored to patient's daily living and vocational requirements.
*
Monitoring:
Regular clinical and radiographic follow-up to assess fracture healing and identify potential complications (e.g., nonunion, malunion, infection). Adjust rehabilitation as needed.
Throughout both phases, patient education regarding their injury, surgical interventions, and the importance of adherence to rehabilitation protocols is crucial for optimizing outcomes. Close communication between the orthopedic team, critical care, physical therapists, and occupational therapists ensures a coordinated and effective rehabilitation strategy.
Summary of Key Literature / Guidelines
The evolution of DCO has been driven by extensive clinical experience and a growing body of literature highlighting the physiological impact of early aggressive surgery in polytrauma.
- "Second Hit" Phenomenon: Early work by Pape et al. (1995, 2000) and Giannoudis et al. (1998, 2005) elucidated the concept of the "second hit" – where the initial trauma (first hit) sensitizes the patient's immune system, and subsequent aggressive surgical interventions (second hit) in physiologically unstable patients trigger an exaggerated systemic inflammatory response, leading to SIRS, ARDS, and MOF. This research provided the physiological rationale for DCO.
-
Early Total Care (ETC) vs. Damage Control Orthopaedics (DCO):
- Historically, ETC (early definitive fixation within 24 hours) was the preferred strategy for long bone fractures, shown to reduce complications in stable polytrauma patients.
- However, meta-analyses and large retrospective studies (e.g., from the German Trauma Registry, published by Keel & Trentz, 2005; Nowotarski et al., 2008) confirmed that while ETC is beneficial for stable patients, DCO significantly improves outcomes (reduced ARDS, MOF, mortality) in unstable or borderline polytrauma patients.
- A critical aspect is defining "physiological stability." Parameters such as base deficit, lactate, pH, core temperature, and transfusion requirements are consistently cited as indicators for DCO. The concept of "borderline patient" further complicates the decision-making, where the trend of these physiological markers is more important than a single measurement.
- Pelvic Trauma Management: The ATLS guidelines emphasize rapid stabilization of hemodynamically unstable pelvic fractures with external compression (e.g., pelvic binder) and consideration of pre-peritoneal packing or angiography for arterial embolization. Orthopedic external fixation is a key DCO intervention for these injuries.
- Open Fracture Management: Gustilo-Anderson classification and subsequent management guidelines dictate urgent debridement and stabilization. In the DCO setting, this often involves serial debridement and external fixation, with delayed definitive coverage.
- Timing of Definitive Fixation: The optimal "window" for definitive fixation after DCO is typically when the "physiological storm" has subsided – patients are normothermic, acidosis has resolved, coagulopathy is corrected, and inflammatory markers are trending down. This usually occurs between 3 and 14 days post-injury, but is highly individualized. Delaying too long can lead to complications like joint stiffness and nonunion.
- Multidisciplinary Approach: Consensus guidelines (e.g., from the Orthopaedic Trauma Association, AO Foundation) consistently advocate for a highly coordinated, multidisciplinary team approach involving trauma surgeons, orthopedic surgeons, anesthesiologists, and intensivists. Communication and clear decision-making algorithms are paramount.
- Evolving Concepts: Research continues into optimal fluid resuscitation strategies, the role of viscoelastic testing (e.g., TEG/ROTEM) in guiding MTPs, and less invasive definitive fixation techniques. The "safe zones" for external fixator pin placement are continually refined based on anatomical studies and clinical outcomes.
In conclusion, Damage Control Orthopaedics is not merely a set of surgical techniques but a comprehensive strategy deeply rooted in an understanding of trauma physiology. Its judicious application in appropriately selected, severely injured patients has unequivocally improved survival and reduced morbidity, establishing it as a cornerstone of modern trauma care.
