Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
DEFINITION
Malunion of the radial or ulnar shaft can lead to pain, loss of motion, loss of strength, and instability at the level of the wrist or elbow.Malrotation, angulation (with narrowing of the interosseous space between the radius and ulna), shortening, and loss of the radial bow have been shown in various studies to lead to decreased functional outcomes. 4,5,9,10,12Arthritis has been reported at the level of the proximal radioulnar joint (PRUJ) with long-standing malunions, although the distal radioulnar joint (DRUJ) is most commonly affected by forearm malunions. 11
ANATOMY
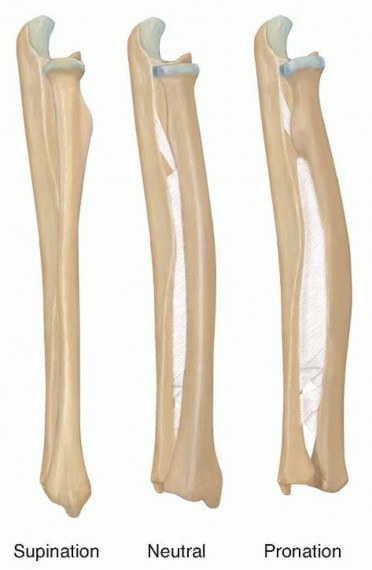
FIG 1 • Lateral projection of the radius and ulna. Relationship of the interosseous membrane to the radius and ulna during forearm rotation. The fibers of the interosseous membrane are longest with the forearm in neutral position and shorten in both pronation and supination.
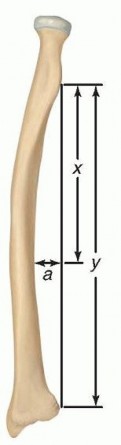
FIG 2 • Measurement of the location and magnitude of the radial bow. The distanceyrepresents the length of the radius as measured from the bicipital tuberosity to the ulnar aspect of the radius. Linea, drawn perpendicular toyfrom the point of greatest curvature of the radius, represents the magnitude of the radial bow (expressed in millimeters). The distancexrepresents the length of the radius from the bicipital tuberosity to the point whereaintersectsy. The location of the radial bow is calculated byx/y× 100. (Adapted from Schemitsch EH, Richards RR. The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 1992;74(7):1068-1078.)
PATHOGENESIS
P.218Both-bone forearm fractures occur through a variety of mechanisms, including indirect trauma (such as falls on an outstretched arm or motor vehicle accidents) and direct trauma (such as blows to the forearm).Acute fractures treated closed or with intramedullary nailing techniques are more likely to heal malunited. 7,8 Radius malunions have a greater effect on forearm rotation than ulna malunions.10,12A torsional deformity of greater than 30 degrees in the radius leads to significant loss of forearm motion. 4 Changes in the length-tension curve of the interosseous membrane may also account for loss of rotation.12
NATURAL HISTORY
Fifty degrees of supination and 50 degrees of pronation are needed for activities of daily living. 6Patients with untreated forearm malunions may experience loss of forearm rotation, PRUJ or DRUJ instability,wrist pain, loss of strength, and arthritis at the PRUJ. 11 The severity of the symptoms depends on the degree of malunion and the corresponding alteration in degree and location of the bow of the radius.Malunions of 10 degrees or less lead to less than a 20-degree loss of forearm rotation and hence are clinically insignificant. 7Angular malalignment of more than 20 degrees in the radius or ulna results in clinically significant loss of motion. Greater than 15 degrees of malalignment leads to inability to perform activities of daily living. 5,7,10Patients with greater than 15 degrees of malalignment or loss of the radial bow will have clinically significant loss of motion and strength if left untreated.
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation for patients with forearm malunions includes a detailed assessment of the patient's functional limitations as well as documentation of elbow and wrist range of motion, the supination-pronation arc of the forearm, and the stability of the PRUJ and DRUJ.Physical examinationThe skin is inspected for scarring or previous incision sites. Muscle bulk and tone are examined.The wrist, elbow, and malunion site are palpated for tenderness.Range of motionThe flexion-extension arc of the elbow is measured with the shoulder at 30 degrees of forward flexion.Rotation of the forearm is ascertained with the humerus stabilized against the chest wall and the elbow at 90 degrees of flexion.Wrist flexion and extension are determined with the forearm in neutral rotation. Joint loss of motion may indicate location of pathology.A high degree of motion loss will lead to functional deficits.PRUJ and DRUJStability of the PRUJ is assessed by palpation during passive pronation and supination.The DRUJ is evaluated by stressing the ulna volarly and dorsally while stabilizing the radius.Subluxation of the ulnar head or the ECU is evaluated during passive range of motion (ECU subluxation test).The piano key test can also be used to assess for an unstable DRUJ. Patients with a positive piano key sign will have an ulnar head that shifts volarly with a minimal volarly directed force and then rebounds dorsally once that force is removed, much like a key in a piano.Pain with compression of the radius and ulna at the level of the DRUJ may also be indicative of DRUJ instability or arthritis (DRUJ compression test).Neurovascular examinationThe examiner should check for anterior interosseous nerve (OK sign), posterior interosseous nerve (PIN) (thumb extension), and ulnar nerve (abduction-adduction of fingers) function.Inability to perform tasks identifies nerve injury.
IMAGING AND OTHER DIAGNOSTIC STUDIES


FIG 3 • A,B. AP and lateral radiographs demonstrate a segmental radius shaft fracture resulting in a malunion both proximally and distally despite open reduction and internal fixation. Note the loss of radial bow in both direction and magnitude, narrowing of the interosseous space between the radius and ulna, dorsal positioning of the distal ulna, and nonunion of the basilar ulnar styloid fracture. The patient was unable to supinate to neutral and demonstrated instability at the DRUJ. C. CT scan demonstrates narrowing of the interosseous space with heterotopic bone formation. P.219The degree of angulation and comminution can be calculated from these films.Contralateral forearm films provide a comparison for the amount of shortening as well as for the location and angle of the radial bow. 9A computed tomography (CT) ( FIG 3C) scan or magnetic resonance imaging (MRI) can also be obtained to assess for malrotation.2
DIFFERENTIAL DIAGNOSIS
DRUJ injury or instability PRUJ injury or instabilityInjury to the interosseous membrane SynostosisNonunion
NONOPERATIVE MANAGEMENT
Nonoperative treatment of malunions depends on the patient's symptoms and includes occupational therapy for strengthening and range of motion, removable off-theshelf braces, non-narcotic medications, and custom-molded DRUJ orthoses.
SURGICAL MANAGEMENT
Operative intervention for forearm malunions depends on the functional limitations of the patient, not the degree of deformity apparent on radiographs.Indications for surgery include loss of forearm rotation that leads to a functional deficit (rotational arc less than 100 degrees), DRUJ instability, unacceptable cosmesis, and painful nonunion.Risks to the patient include vascular injury, nerve injury or paresthesias (specifically the superficial radial nerve), infection, nonunion, delayed union, need for iliac crest bone graft, synostosis, loss of motion, and DRUJ instability.Patients treated within 1 year of the initial injury may be more likely to improve functionally and have a lower surgical complication rate. 11Malunions of the radius and ulna are generally treated with an open approach, corrective osteotomy of one or both bones, compression plating, and bone grafting as necessary.Generally, the more deformed bone is corrected first. If after correction of the first bone forearm rotation is still lacking, an osteotomy is performed on the second bone.If both bones are equally deformed, the ulna is osteotomized and provisionally plated first to provide a working length for the radius.Restoration of the radial bow in large part determines functional outcome.Patients whose radial bow is restored within 1.5 mm of magnitude and located within 4.3% of the contralateral forearm regain 80% of normal motion.Eighty percent of grip strength is regained if the radial bow is located within 5% of the contralateral side. 9Anatomic realignment of the radius and ulna will not improve functional deficits if a synostosis or significant scarring and contracture involving the soft tissues has occurred.Occult injury to or contracture of the DRUJ and PRUJ must be identified and treated at the time of surgery.
PREOPERATIVE PLANNING
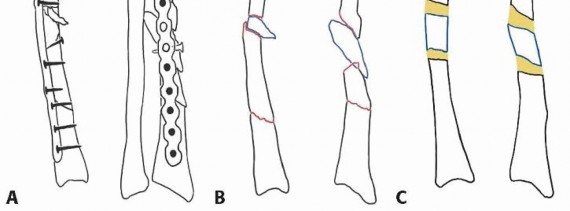
Radiographs of the affected and contralateral extremity should be reviewed.A CT scan is helpful to assess for rotational deformity.A corrective three-dimensional osteotomy is planned using standard AO technique ( FIG 4).The need for corticocancellous iliac crest bone graft should be determined by the degree of shortening.The surgeon should be familiar with techniques for reconstruction or stabilization of the DRUJ should it remain unstable after correction of the malunion.
POSITIONING
The patient is positioned supine on the operating table. A radiolucent hand board is attached to the table, centered on the patient's axilla. The affected extremity is then extended and can be positioned for either a volar or dorsal approach to the radius by rotating through the shoulder.The subcutaneous border of the ulna can be visualized by flexing the arm at the elbow or by placing the arm across the chest.A nonsterile tourniquet may be used on the arm.
APPROACH

TECHNIQUES
Volar Approach to the Radius
Landmarks: biceps tendon, brachioradialis (BR), radial styloid
Center the skin incision over the malunion site and follow a line that begins lateral to the biceps tendon, continues over the medial edge of the BR, and ends distally at the level of the radial styloid.
The length of the incision depends on the amount of exposure needed to take down the malunion and plate the osteotomy.
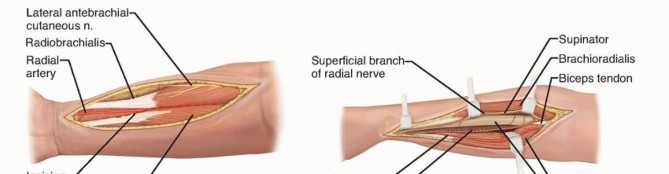
To expose the midshaft, dissect between the BR and the pronator teres (PT) proximally ( TECH FIG 1).
The superficial radial nerve lies on the undersurface of the BR and must be protected.
VOLAR APPROACH TO THE RADIUS
TECH FIG 1 • A-C. Exposure of the radial shaft through the volar approach. This approach is best for midshaft and distal shaft malunions.
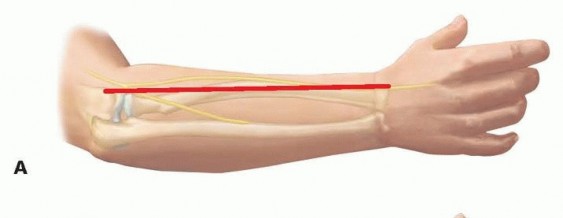
TECH FIG 2 • Exposure of the radius through the dorsal approach. This approach is best for proximal shaft malunions. A. Skin incision on dorsal surface, running from tip of lateral epicondyle toward radial styloid. B. The PIN is followed through the supinator, with its branches preserved.
APPROACH TO THE ULNA
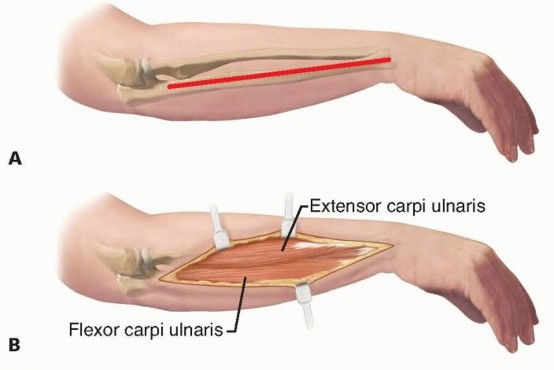
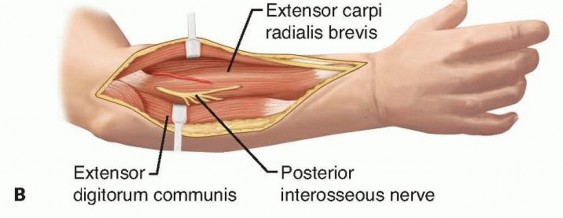
TECH FIG 3 • Exposure of the ulna. A. Skin incision along subcutaneous border of ulna. B. Dissection is performed between the ECU dorsally and the FCU volarly.
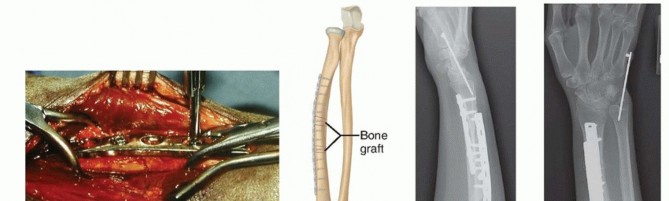
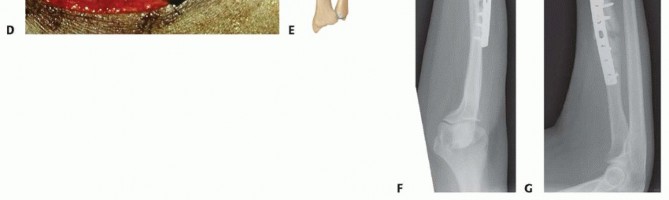
REDUCTION, PLATING, AND BONE GRAFTING


PEARLS AND PITFALLS
|Indications ▪ Assess DRUJ stability.1.Determine that lack of motion is not due to soft tissue contracture, synostosis, or interosseous membrane scarring, for which realignment of the malunion would not improve motion.Osteotomy ▪ Obtain contralateral forearm films to determine location and magnitude of radial bow.2.Obtain CT or MRI if concerned for rotational malunion.3.Perform detailed preoperative drawings to determine the ideal location for the osteotomy, the degree and direction of correction required, and the need for bone graft.4.Obtain consent for bone graft.Approach ▪ If a volar approach to the proximal radius is chosen, avoid injury to the PIN by careful subperiosteal stripping of the supinator from the radius and gentle retraction of the supinator laterally to prevent a traction neurapraxia. Avoid placing a retractor around radial neck, as this can compress the PIN (or cause a traction injury of the nerve).Gently retract the superficial radial nerve and radial artery.5.Protect the PIN during dissection when approaching the proximal radius dorsally. The nerve lies directly on bone dorsally, opposite of the bicipital tuberosity in 25% of patients. Avoid trapping the nerve between the plate and bone when placing a plate proximally.DRUJ ▪ Determine the cause of instability of the DRUJ once malalignment is restored.6.Perform a procedure that addresses the precise cause of the DRUJ instability.|------
POSTOPERATIVE CARE
P.223In a compliant patient with secure fixation, the splint may be removed 5 to 7 days after surgery and range-of-motion exercises initiated.A removable orthosis is worn for the next 4 to 5 weeks. Strengthening exercises are begun 6 weeks after surgery.Resistive strength training is delayed until radiographic evidence of healing is present (usually 8 to 12 weeks postoperatively).Normal activities are resumed when a solid union is present. Plates are generally not removed in adults.If concomitant DRUJ instability is present:A Munster cast is applied at the first postoperative visit. The forearm is held in full supination for 6 weeks. Finger range-of-motion and elbow flexion-extension exercises are begun at the first postoperative visit.At 6 weeks, any pins in the DRUJ are removed and supination-pronation exercises are initiated.
OUTCOMES
Trousdale and Linscheid 11 retrospectively reviewed 27 patients with corrective osteotomies for forearm malunions. Indications for surgery included loss of rotation (20 patients), unstable DRUJ (6 patients), and cosmesis (1 patient).11Of the 6 patients with DRUJ instability, 5 had stable wrist joints at follow-up. Three patients were stabilized with correction of the deformity alone and 3 required reefing of the palmar capsule and temporary pinning of the DRUJ with Kirschner wires (K-wires).The patient who underwent the procedure for cosmesis lost 10 degrees of rotation but was happy with the overall appearance and function.The age of the patient at the time of injury, location of the malunion, and involvement of one or both bones were not associated with the final outcome.Shorter time from injury to corrective surgery ( <12 months) was associated with improved forearm rotation and a lower complication rate.
COMPLICATIONS
A 48% complication rate was noted in Trousdale and Linscheid's 11 study. InfectionWrist pain Loss of motionHeterotopic ossification DRUJ instabilityDelayed union or nonunion Superficial radial nerve paresthesias
REFERENCES
- Botte M. Skeletal anatomy. In: Doyle J, Botte M, eds. Surgical Anatomy of the Hand and Upper Extremity. Philadelphia: Lippincott Williams & Wilkins, 2003:3-91.
- Dumont CE, Pfirrmann CW, Ziegler D, et al. Assessment of radial and ulnar torsion profiles with cross-sectional magnetic resonance imaging. J Bone Joint Surg Am 2006;88(7):1582-1588.
- Hoppenfeld S, deBoer P. The forearm. In: Hoppenfeld S, deBoer P, eds. Surgical Exposures in Orthopaedics, ed 2. Philadelphia: Lippincott Williams & Wilkins, 1994:117-146.
- Kasten P, Krefft M, Hesselbach J, et al. How does torsional deformity of the radial shaft influence the rotation of the forearm? A biomechanical study. J Orthop Trauma 2003;17:57-60.
- Matthews LS, Kaufer H, Garver DF, et al. The effect on supination-pronation of angular malalignment offractures of both bones of the forearm. J Bone Joint Surg Am 1982;64(1):14-17.
- Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63(6):872-877.
- Sarmiento A, Ebramzadeh E, Brys D, et al. Angular deformities and forearm function. J Orthop Res 1992;10:121-133.
- Schemitsch EH, Jones D, Henley MB, et al. A comparison of malreduction after plate and intramedullary nail fixation of forearm fractures. J Orthop Trauma 1995;9:8-16.
- Schemitsch EH, Richards RR. The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 1992;74(7):1068-1078.
- Tarr RR, Garfinkel AI, Sarmiento A. The effects of angular and rotational deformities of both bones of the forearm. An in vitro study. J Bone Joint Surg Am 1984;66(1):65-70.
- Trousdale RT, Linscheid RL. Operative treatment of malunited fractures of the forearm. J Bone Joint Surg Am 1995;77(6):894-902.
- Tynan MC, Fornalski S, McMahon PJ, et al. The effects of ulnar axial malalignment on supination and pronation. J Bone Joint Surg Am 2000;82-A(12):1726-1731.
