Corrective Osteotomy for Distal Radius Malunion
DEFINITION
Distal radius malunion is best defined as malalignment associated with dysfunction.Malalignment does not always result in dysfunction. In particular, the vast majority of older, low-demand patients function very well with deformity.Dysfunction can include loss of motion, loss of strength, or pain. 1,2,5Pain can be the most difficult to associate with deformity. Osteotomy for pain—as with any surgery for pain—is relatively unpredictable and should be undertaken with caution. Carpal malalignment, ulnocarpal impaction, and distal radioulnar joint (DRUJ) malalignment are all potentially painful and can be variably addressed.The relationship between distal radius malunion and carpal tunnel syndrome is debated. Some surgeons claim a direct causal relationship as well as the ability to improve carpal tunnel syndrome with osteotomy alone.
ANATOMY
Loss of alignment can be measured on radiographs.Angulation of the articular surface on the lateral view is measured as the angle between a line connecting the dorsal and palmar lips of the distal radius articular surface on the lateral view and a line perpendicular to the radius shaft.Ulnarward inclination (often calledradial inclination, a misnomer because the articular surface tilts toward the ulna) is measured as the angle between a line connecting the ulnar limit and the radial limit of the distal radius articular surface on the posteroanterior (PA) view and a line perpendicular to the radial shaft.Ulnar variance is a better measure of shortening of the radius than radial length. It is measured as the distance between two lines drawn perpendicular to the radial shaft on the PA view, one at the level of the most ulnar corner of the lunate facet and the other at the distal limit of the ulnar head.Positive ulnar variance means that the ulna is longer than the radius. Negative means the ulna is shorter.Loss of articular surface alignment can be measured on radiographs as gap, step, or subluxation.This is most accurately measured using computed tomography (CT) images ( FIG 1).Sources of variability in radiographic measurements include variation in the radiographs, imprecision in the measurement techniques, and imprecision in the selection of the points of reference.
PATHOGENESIS
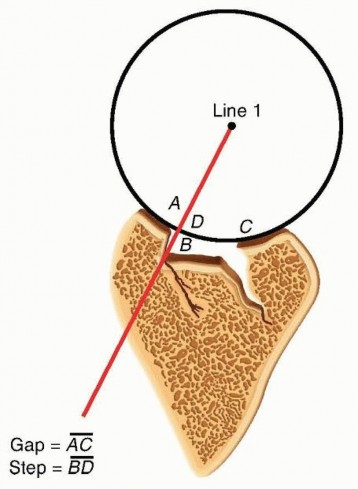
FIG 1 • The arc method for measuring articular malalignment of the distal radius. The distance betweenBandDis the articular step, and the distance betweenAandCis the maximum articular gap. (After Catalano LW III, Cole RJ, Gelberman RH, et al. Displaced intra-articular fractures of the distal aspect of the radius: long-term results in young adults after open reduction and internal fixation. J Bone Joint Surg Am 1997;79[9]:1290-1302.)P.323Early removal of pins or an external fixator. Settling of the fracture can also be observed after implant removal more than 6 weeks after injury, particularly when there is substantial metaphyseal comminution.Nonlocked plates may loosen in osteopenic metaphyseal bone.Complacence must be avoided. Many older patients desire optimal wrist alignment and function, and treatment decisions should not be made on chronologic age alone.
NATURAL HISTORY
Ulnar-sided wrist pain can improve for a year or more after fracture of the distal radius, so patience is warranted.Lack of forearm rotation may be related to capsular contracture or bony malalignment. For slight malunions, patience with exercises and rehabilitation is advisable.Although it is often stated that an extra-articular distal radius malunion leads to future arthrosis, there are no data to support this contention.After a recovery period of 1 to 2 years from fracture, the functional deficits seem fairly stable.Articular incongruity or subluxation in relatively nonarticular areas can be reasonably well tolerated, but in most cases, intra-articular incongruity will lead to arthrosis, pain, and dysfunction. There is no clear time frame for these changes— indeed, symptoms do not correlate well with radiographic anatomy or arthrosis and the predictors of arthrosis are not well established.
PATIENT HISTORY AND PHYSICAL FINDINGS
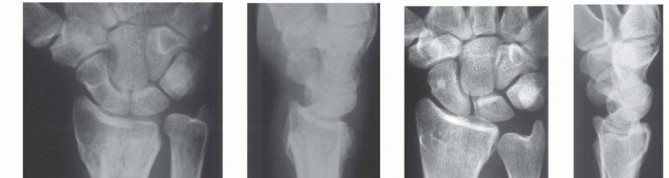
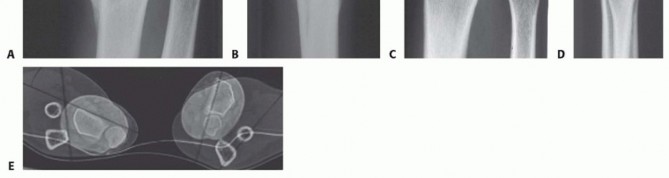
FIG 2 • A,B. Anteroposterior (AP) and lateral radiographs of extra-articular dorsally angulated malunion. C,D. PA and lateral radiographs of an extra-articular dorsally displaced malunion. E. CT shows rotational deformity associated with a volarly displaced extra-articular fracture. (Copyright Diego Fernandez, MD, PhD.) Lack of motion should be clearly due to malalignment and not due to pain or protectiveness—likewise for instability of the DRUJ.Range of motion: A goniometer is used to measure wrist flexion, extension, radial and ulnar deviation, supination, and pronation.Ulnocarpal compression: The carpus is forcefully ulnarly deviated toward the ulna.Consistent reproduction of usual pain with ulnar deviation tasks is consistent with ulnocarpal impaction.The examiner can test for DRUJ instability by stabilizing the radius and trying to subluxate the distal ulna dorsal and volar from the sigmoid notch of the radius.Substantially, less stability than the opposite side may correlate with symptomatic DRUJ instability, but this is a very difficult and subjective test.Scaphoid shift test: Instability compared to the opposite wrist would indicate a possible scapholunate interosseous ligament tear, indicating a potential dissociative rather than the typical nondissociative carpal malalignment usually associated with distal radius malunion.Grip strength is one of the measure of wrist dysfunction, but it is largely determined by pain and effort—both strongly influenced by psychosocial factors.
IMAGING AND OTHER DIAGNOSTIC STUDIES
PA and lateral radiographs of the wrist ( FIG 2A-D) can be supplemented by specific radiographs for evaluation of the joint surface, particularly for potential articular malunions.Comparison with the opposite, uninjured wrist is useful and serves as a template for surgical correction.CT, particularly three-dimensional CT, is useful to precisely evaluate the joint surfaces ( FIG 2E).Neurophysiologic tests (nerve conduction velocity and electromyography) are ordered to evaluate any symptoms or signs of carpal tunnel syndrome that may need to be addressed.P.324
DIFFERENTIAL DIAGNOSIS
Stiffness: capsular stiffness and tendon adhesions Numbness: idiopathic carpal tunnel syndromePain: another discrete source of pain or even nonspecific pain
NONOPERATIVE MANAGEMENT
Nonoperative management is appropriate for low-demand and infirm individuals. Splints are weaned after 6 weeks of cast immobilization. Patients who struggle to regain motion may benefit from working with an occupational therapist or a certified hand therapist. Normal activities are resumed in 3 or 4 months. The patient may return every 2 or 4 months or so until satisfied with the result.Patience is warranted in many situations, particularly for patients with ulnar-sided wrist pain thought to be due to an extra-articular malunion.This discomfort is the last pain to go away after a distal radius fracture and can last up to a year.
SURGICAL MANAGEMENT
Surgery is appropriate when a radiographic deformity correlates with a specific anatomically correctable problemand the deformity is associated with a substantial risk of dysfunction or arthrosis.The patient must understand the risks and benefits of intervening.The surgeon should be wary of pain as the primary complaint because pain is strongly influenced by psychosocial factors, and pain relief is an achievable goal only when consistent with an objective, correctable anatomic deformity such as discomfort clearly associated with a substantial ulnocarpal impingement.When the issue is restriction of motion and there is less than 20 degrees of dorsal tilt or less than 5 mm of ulnar positive variance, a nonoperative approach may be warranted.There are no fixed rules or thresholds for acceptable alignment. The correlation with symptoms and disability is more important.Intra-articular osteotomies should be considered only when the malalignment is simple and the planned correction is straightforward.For instance, osteotomy of a volar shearing fracture would be considered when the fragment is large, there is little or no articular comminution or impaction, and the dorsal fragments are not healed in a malaligned position.Distal radius osteotomy need not be performed urgently. The patient should have demonstrated excellent exercise skills and full finger motion and there should be no significant nerve or tendon dysfunction or edema.In the case of an intra-articular malunion, intervening early (optimally within 10 weeks) when the fracture is not completely healed may take precedence over these concerns.
PREOPERATIVE PLANNING
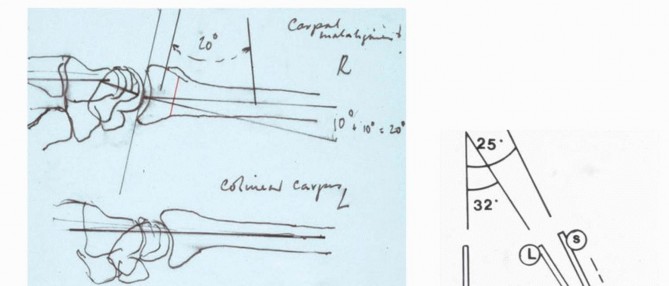
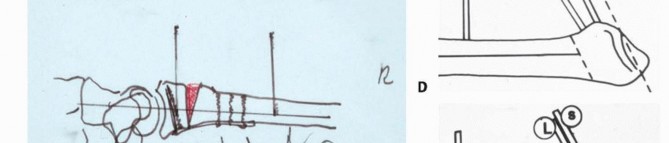
The desired angular, rotational, and length corrections are planned based on preoperative radiologic studies, including a radiograph of the opposite wrist if uninjured ( FIG 3A,B).It can be useful to draw and write out a reconstruction plan, particularly for complex malunions ( FIG 3C-E). In that way, every contingency is anticipated and the surgery is likely to go more smoothly.
POSITIONING
The patient is positioned supine with the arm supported on a hand table.A nonsterile pneumatic tourniquet is used and inflated after exsanguination and before the skin incision.
APPROACH


TECHNIQUES
Dorsal Extra-articular Distal Radius Osteotomy: Corticocancellous Graft
Dorsal Extra-articular Distal Radius Osteotomy: Corticocancellous Graft
EXPOSURE
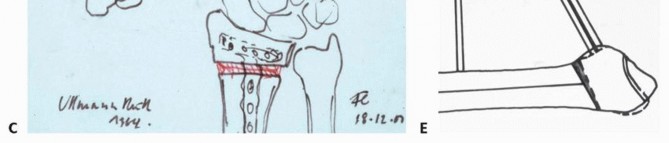
Make a longitudinal incision centered over the tubercle of Lister, in line with the third metacarpal ( TECH FIG 1A).Elevate skin flaps, taking care to protect the branches of the superficial radial nerve in the radial skin flap.Incise the retinaculum over the third extensor compartment. Remove the tendon of the extensor pollicis longus (EPL) and transpose it radialward ( TECH FIG 1B).The EPL tendon will be left in the subcutaneous tissues at the completion of the procedure.Elevate the fourth dorsal compartment and its tendons subperiosteally.Preserve the integrity of this compartment.It is usually not possible to elevate the second dorsal compartment subperiosteally, so simply retract the extensor carpi radialis brevis and longus tendons radialward after opening the compartment.
OSTEOTOMY AND REALIGNMENT
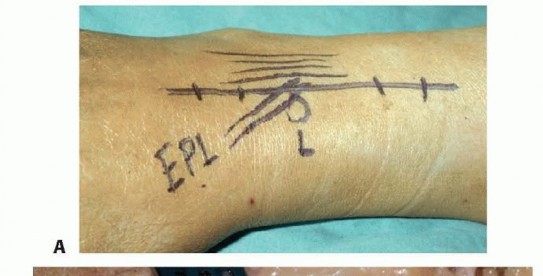


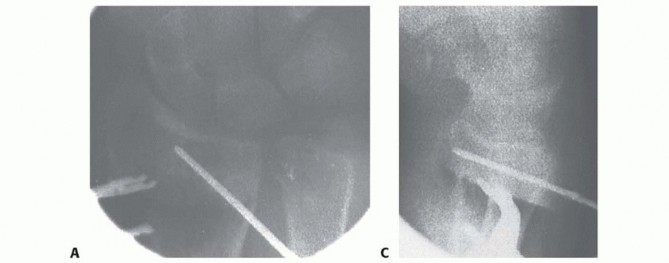


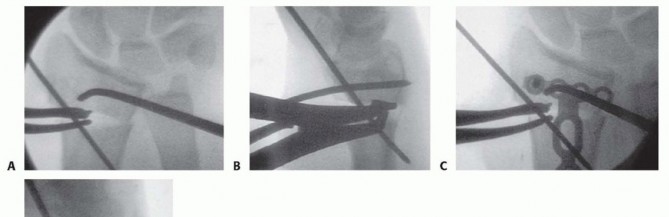
TECH FIG 2 • A. Kirschner wires are placed parallel to the articular surface. Fluoroscopic image showing pin placement. B. The osteotomy is made with a saw as close as possible to the original fracture site. C. Lateral fluoroscopic image showing use of a lamina spreader to realign the distal fragment. D. The osteotomy has been opened and is ready for graft placement. (Copyright Diego Fernandez, MD, PhD.) A distractor or small external fixator may facilitate realignment and provisionally stabilize the fracture.The proximal threaded pin is drilled into the radial diaphysis perpendicularly in a position that will not interfere with implant application.The distal threaded pin is drilled at an angle equal to the desired correction of the lateral tilt of the distal radius articular surface so that distraction of the two pins will bring this pin parallel to the proximal pin (perpendicular to the radius), thereby restoring alignment.The pins should be drilled so that they also help restore the appropriate ulnarward inclination of the distal radius articular surface when distracted.Planned angular corrections can be monitored with sterile geometric templates.The osteotomy is made parallel with the distal Kirschner wire and as close to the original fracture site as possible using an oscillating saw ( TECH FIG 2B).If the fracture is not yet completely healed (nascent malunion— usually within 4 months of injury), recreate the original fracture line by carefully removing fracture callus at the fracture site.This callus can be saved and used as bone graft.If the fracture is solidly healed, attempt to identify the prior fracture site. If this is uncertain, choose a site that creates a distal fragment large enough to facilitate manipulation and internal fixation while trying tostay distal enough to take advantage of the healing capacity of metaphyseal bone.A lamina spreader can be used to help realign the distal fragment as well ( TECH FIG 2C,D).Care must be taken when operating on osteoporotic bone.Additional provisional stability can be provided by placing 1.6-mm smooth Kirschner wires.If the ulnar variance can be restored with angular realignment alone, the volar cortex can be cracked and hinged open in an attempt to maintain some stability of the osteotomy. If lengthening of the volar cortex is required to restore ulnar variance, a second distractor in another plane (eg, direct radial) may prove useful for obtaining and maintaining alignment.
GRAFT INSERTION AND FIXATION
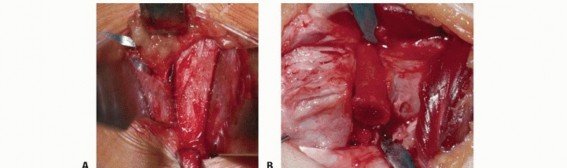
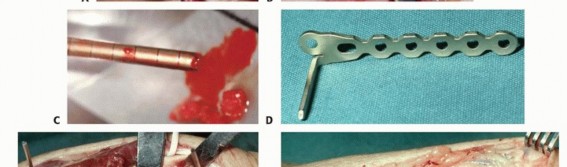
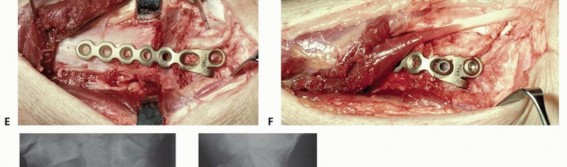

TECH FIG 3 • A. Corticocancellous bone graft is harvested from the iliac crest. B. After final sculpting, it is applied to the osteotomy site. C. Autogenous cancellous bone graft is harvested from the iliac crest using a trephine. D. A 2.0-mm condylar blade plate can provide fixed-angle internal fixation. E,F. Intraoperative photographs of the fixation. G,H. Final anteroposterior (AP) and lateral radiographs. (Copyright Diego Fernandez, MD, PhD.) When a structural, corticocancellous bone graft is used, a single plate or a plate and separate screw may be adequate ( TECH FIG 3D-H).Plates with angular stable screws or blades in the distal fragment may be more reliable than standard screws, particularly if the bone is of poor quality and if nonstructural graft is chosen.Once implants are placed and stability is ensured, remove all provisional fixation devices.This entire process is monitored using image intensification to confirm appropriate osteotomy site, correction of alignment, and implant placement.Repair the extensor retinaculum with absorbable suture.In some cases, a flap of retinaculum is brought deep to the tendons to add a layer of protection betweenthe implants and extensor tendons.We usually do not close the retinaculum, and we no longer make retinacular flaps.The tourniquet is deflated and hemostasis ensured. The skin is closed.A bulky dressing incorporating a volar plaster wrist splint is applied.1. Volar Extra-articular Distal Radius Osteotomy
EXPOSURE

REALIGNMENT AND PROVISIONAL FIXATION
The fragments are realigned using the techniques described earlier ( TECH FIG 4).The techniques are similar to those for acute fractures once an adequate soft tissue release has been performed.Apply a fixed-angle volar implant.Insert provisional Kirschner wires either through or adjacent to the plate (see TECH FIG 4).
PLATE FIXATION


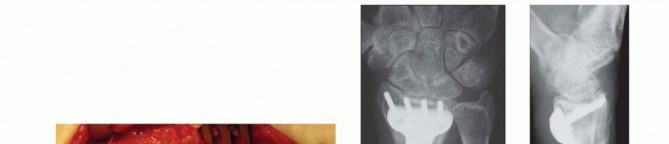
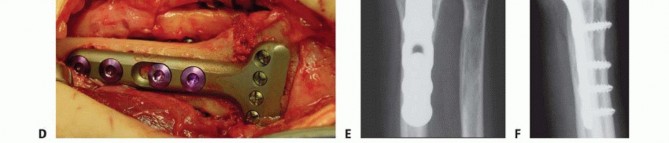
TECH FIG 5 • A. Fluoroscopic image of plate fixation and realignment. B. Defect after correction. Autogenous cancellous graft (C) and graft placement (D), showing final clinical appearance. E,F. Final PA and lateral radiographs. (Copyright Diego Fernandez, MD, PhD.)
INTRA-ARTICULAR DISTAL RADIUS OSTEOTOMY




TECH FIG 6 • A-C. PA and lateral radiographs and CT of an intra-articular dorsally angulated malunion. D. A Freer elevator is used under fluoroscopy to reposition the articular fragment. E,F. Intraoperative fluoroscopic views showing provisional correction and fixation. G,H. Final plate and screw fixation. (Copyright Diego Fernandez, MD, PhD.)
PEARLS AND PITFALLS
Preoperative plan3.A poor or incomplete preoperative plan will increase the amount of uncertainty and hesitation during surgery. This will increase the operative time and the frustration level and will decrease the satisfaction with the surgery.4.Making a detailed preoperative plan will improve the efficiency and efficacy of the procedure.Extra-articular malunions1.Manipulating the distal fragment can be much more difficult with poor-quality bone.2.The use of a distractor or small external fixator greatly facilitates realignment and provisional stabilization of the fragments.3.Consider using two distractors in perpendicular planes (eg, one dorsal and one direct radial) to help obtain and maintain alignment.4.Restoration of length in addition to that gained with angular realignment (ie, lengthening of both the dorsal and volar cortices) is much more difficult.5.The most difficult part of performing an osteotomy for a dorsal angulated malunion from a volar approach is realignment of the bone.6.An extended FCR exposure allows release of the dorsal periosteum and Z-lengthening of the brachioradialis, both of which facilitate realignment of the radius.Intraarticular malunions7.Handling small articular fracture fragments can be difficult.8.Each fragment can be realigned using a Kirschner wire as a joystick.9.The articular osteotomy is easiest when the original fracture lines can be identified.10.Try to intervene within 3 months of injury when articular malunion is identified.
POSTOPERATIVE CARE
P.331Active and active-assisted exercise of the fingers and forearm, finger exercises to reduce swelling, and active functional use of the limb for light tasks are encouraged immediately.The initial plaster splint is exchanged for a custom Orthoplast removable splint 2 weeks after the surgery.The patient gradually weans out of the splint between 4 and 6 weeks after surgery and initiates active and active-assisted wrist exercises.Strengthening and forceful use of the arm are restricted until early radiographic union is apparent.Unrestricted use of the limb is allowed when solid union is present clinically and radiographically.
OUTCOMES
Fernandez' 1,2 articles describing dorsal osteotomy with corticocancellous bone graft with and without Bowers arthroplasty of the DRUJ established the value of the technique for improving function in patients with symptomatic distal radius malunions.He documented good or excellent results in 75% and 80% of patients, respectively, noting thatsatisfactory results depend on the absence of degenerative changes in the radiocarpal and intercarpal joints, and the presence of adequate preoperative range of motion of the wrist.Corrective osteotomy with carefully preoperatively planned structural corticocancellous bone graft does not reliably achieve the planned correction. 12Nonunions, loss of alignment, and major complications were not reported in these series.Jupiter and Ring 5 demonstrated that early correction of distal radius deformity shortened the period of disability without increasing complications and that the combination of cancellous autograft and lockingplates was as reliable as corticocancellous bone grafting. 9Nonunions, loss of alignment, and major complications were not reported in these series.Several small articles have established the safety and efficacy of volar osteotomy for a dorsally displaced fracture. 4,6Shea et al 10 established the safety and efficacy of osteotomy for volar extra-articular malunions in a case series.Fernandez et al 3 established the safety and efficacy of osteotomy for a radially deviated extra-articular malunion in a case series.Several case series have documented the safety and efficacy of intra-articular osteotomy. 7,8,11
COMPLICATIONS
NonunionLoss of alignment Loss of fixation InfectionWound problems Nerve injury
REFERENCES
- Fernandez DL. Correction of post-traumatic wrist deformity in adults by osteotomy, bone grafting, and internal fixation. J Bone Joint Surg Am 1982;64(8):1164-1178.
- Fernandez DL. Radial osteotomy and Bowers arthroplasty for malunited fractures of the distal end of the radius. J Bone Joint Surg 1988;70(10):1538-1551.
- Fernandez DL, Capo JT, Gonzalez E. Corrective osteotomy for symptomatic increased ulnar tilt of the distal end of the radius. J Hand Surg Am 2001;26(4):722-732.
- Henry M. Immediate mobilisation following corrective osteotomy of distal radius malunions with cancellous graft and volar fixed angle plates. J Hand Surg Eur Vol 2007;32:88-92.
- Jupiter JB, Ring D. A comparison of early and late reconstruction of the distal end of the radius. J Bone JointSurg 1996;78(5):739-748.
- Malone KJ, Magnell TD, Freeman DC, et al. Surgical correction of dorsally angulated distal radius malunions with fixed angle volar plating: a case series. J Hand Surg Am 2006;31(3):366-372.
- Marx RG, Axelrod TS. Intraarticular osteotomy of distal radial malunions. Clin Orthop Relat Res 1996; (327):152-157.
- Ring D, Prommersberger KJ, Gonzalez del Pino J, et al. Corrective osteotomy for intra-articular malunion of the distal part of the radius. J Bone Joint Surg Am 2005;87(7):1503-1509.
- Ring D, Roberge C, Morgan T, et al. Osteotomy for malunited fractures of the distal radius: a comparison of structural and structural autogenous bone grafts. J Hand Surg Am 2002;27(2):216-222.
- Shea K, Fernandez DL, Jupiter JB, et al. Corrective osteotomy for malunited, volarly displaced fractures of the distal end of the radius. J Bone Joint Surg Am 1997;79(12):1816-1826.
- Thivaios GC, McKee MD. Sliding osteotomy for deformity correction following malunion of volarly displaced distal radial fractures. J Orthop Trauma 2003;17:326-333.
- von Campe A, Nagy L, Arbab D, et al. Corrective osteotomies in malunions of the distal radius: do we get what we planned? Clin Orthop Relat Res 2006;450:179-185.
