INTRODUCTION TO COMPLEX THUMB DUPLICATIONS
Congenital anomalies of the thumb encompass a broad spectrum of morphological and functional deficits, ranging from simple soft-tissue duplications to complex osseous and syndromic deformities. Among the most challenging to reconstruct are the higher-order bifid thumbs (Wassel Types III through VI) and the triphalangeal thumb.
The primary goal of surgical intervention in these anomalies is not merely the ablation of a supernumerary digit, but the meticulous reconstruction of a single, stable, sensate, and biomechanically functional thumb. Achieving this requires a profound understanding of hand kinematics, intrinsic muscle anatomy, and pediatric physeal development. Simple amputation of the extra digit is universally condemned in modern orthopedic practice, as it invariably leads to progressive angular deformity, joint instability, and a functionally compromised pinch mechanism.
CORRECTION OF TYPES III THROUGH VI BIFID THUMBS
The Wassel classification remains the gold standard for categorizing radial polydactyly. Types III through VI involve duplication at or proximal to the metacarpophalangeal (MCP) joint:
* Type III: Bifid proximal phalanx.
* Type IV: Complete duplication of the proximal and distal phalanges (the most common variant).
* Type V: Bifid metacarpal.
* Type VI: Complete duplication of the metacarpal and phalanges.
The surgical approach described by Lamb, Marks, and Bayne serves as the foundational technique for addressing these complex duplications. The procedure emphasizes the preservation of vital tendinous and ligamentous structures from the excised digit to augment the retained thumb.
Preoperative Considerations and Biomechanics
Careful clinical and radiographic evaluation is mandatory. The surgeon must identify the dominant digit—typically the ulnar thumb, which often possesses better collateral ligament stability and a more functional articulation with the trapezium. The radialmost digit is usually the most hypoplastic and is therefore selected for excision. However, the intrinsic musculature (specifically the abductor pollicis brevis) often inserts aberrantly into the radial digit and must be meticulously preserved and transferred.
💡 Clinical Pearl
Always assess the tracking of the flexor pollicis longus (FPL) and extensor pollicis longus (EPL) preoperatively. Eccentric insertions of these tendons are the primary drivers of late "zig-zag" deformities following reconstruction. Centralization of the tendinous pull is just as critical as osseous alignment.
Surgical Technique (Lamb, Marks, and Bayne)
1. Positioning and Exposure
* The procedure is performed under general anesthesia with the use of a pneumatic tourniquet and loupe magnification.
* Design a racquet-shaped incision over the most hypoplastic thumb (usually the radialmost digit). The incision should be planned to leave a generous, well-vascularized skin flap that can be utilized to close the defect or augment the first web space.
* If the ulnar thumb is paradoxically more affected and selected for excision, the incision is mirrored accordingly.
2. Intrinsic Muscle Preservation
* Through the radial incision, carefully dissect and expose the abductor pollicis brevis (APB) tendon as it inserts into the proximal phalanx of the radialmost thumb.
* Detach the APB with a small sleeve of periosteum to ensure a robust repair later. Carefully preserve this tendon.
* Surgical Variation: If the ulnar thumb is to be excised, the adductor pollicis must be identified, detached, and meticulously preserved for transfer to the retained radial digit.
3. Collateral Ligament Management
* Identify the collateral ligament shared between the two digits or connecting the excised digit to the metacarpal.
* Detach the collateral ligament distally from the phalanx that is to be excised.
* Strip the collateral ligament proximally off the metacarpal or phalanx, taking a contiguous strip of periosteum. This periosteal sleeve is critical; it provides a strong, vascularized tissue layer that allows for adequate exposure of the joint and ensures a secure, bone-to-bone healing environment upon reattachment.
4. Excision and Joint Remodeling
* Excise the supernumerary digit.
* Attention must now be turned to the articular surface of the metacarpal (or proximal phalanx in Type III). The articular surface is typically broadened or bifid.
* Using a scalpel (in infants) or an oscillating saw, shave the prominent articular cartilage and bone of the metacarpal head so that it matches the width of the articular base of the retained phalanx. Failure to narrow the joint will result in a cosmetically unacceptable, bulbous joint and mechanical impingement.
5. Centralization and Ligamentous Reconstruction
* Centralize the remaining digit over the newly remodeled articular surface.
* Advance the previously preserved collateral ligament and the intrinsic tendon (APB or Adductor) to the base of the retained phalanx.
* Suture these structures securely to the periosteum and capsule of the retained phalanx using non-absorbable or slowly absorbable sutures (e.g., 4-0 or 5-0 PDS).
6. Osseous Fixation
* Secure the centralized alignment by driving a longitudinal Kirschner wire (0.035- or 0.045-inch, depending on patient size) retrograde across the interphalangeal and metacarpophalangeal joints.
* Ensure the K-wire is placed centrally to avoid physeal injury.
7. Tendon Realignment and Closure
* Critically evaluate the alignment of the extensor and flexor tendons. They must track centrally along the longitudinal axis of the digit.
* If the tendons pull eccentrically, partial resection of the tendon sheath, pulley reconstruction, or formal tendon transfer may be required to achieve a central line of pull.
* Close the skin with simple interrupted absorbable sutures (e.g., 5-0 chromic gut or fast-absorbing plain gut).
* If the skin is inadequate along the ulnar border for a tension-free closure, or if the first web space is contracted, a Z-plasty or local rotation flap must be incorporated.
Postoperative Rehabilitation Protocol
The thumb is immobilized in a well-padded, long-arm thumb spica cast for approximately 4 weeks. At the 4-week mark, the cast and the longitudinal K-wire are removed in the clinic. The hand is then mobilized under the guidance of a pediatric hand therapist. A custom-molded thermoplastic protective splint is fabricated and worn full-time (except for hygiene and exercises) for an additional 3 to 4 weeks to protect the ligamentous reconstruction from stretching.
THE TRIPHALANGEAL THUMB: PATHOANATOMY AND CLASSIFICATION
As the nomenclature implies, the triphalangeal thumb is characterized by the presence of three phalanges instead of the normal two. This is an uncommon congenital anomaly that can be inherited as an autosomal dominant trait. Genetically, it is frequently associated with point mutations in the ZRS (Zone of Polarizing Activity Regulatory Sequence), a long-range enhancer of the Sonic Hedgehog (SHH) gene. Historically, it has also been associated with the maternal use of thalidomide.
Etiology and Associated Syndromes
The triphalangeal thumb rarely presents in isolation. The most common hand anomaly associated with a triphalangeal thumb is a bifid thumb (radial polydactyly). Systemic and syndromic associations are significant and warrant a comprehensive pediatric evaluation. These include:
* Cleft foot and tibial hemimelia.
* Congenital heart disease (e.g., Holt-Oram syndrome).
* Fanconi anemia (requiring chromosomal breakage studies).
* Anomalies of the gastrointestinal tract (e.g., imperforate anus).
* Various chromosomal anomalies.
Morphological Classification
Triphalangeal thumbs are broadly classified based on the morphology of the extra phalanx and the functional status of the first web space.
Type I Deformities (Delta Phalanx)
In Type I deformities, the extra ossicle is small and wedge-shaped, commonly referred to as a "delta phalanx" or a longitudinally bracketed epiphysis. This wedge shape causes a severe angular deformity (clinodactyly), typically deviating the thumb ulnarward at the interphalangeal joint level. Crucially, this extra ossicle does not significantly increase the overall length of the thumb.

Radiographic appearance demonstrating a transitional/delta phalanx causing angular deformity.
Type II Deformities (Five-Fingered Hand)
In Type II deformities, the extra phalanx is rectangular and normal or nearly normal in size. This creates a thumb that is significantly longer than normal, lying in the same plane as the other fingers, effectively creating the appearance of a five-fingered hand.

Clinical appearance of a Type II triphalangeal thumb (five-fingered hand) associated with duplication (Wassel type VII).
Patients with Type II deformities typically possess extra skin creases overlying the additional interphalangeal joint. Functionally, these thumbs are nonopposable. Patients are unable to oppose the thumb to the other digits and are forced to rely on weak side-to-side (key) prehension. Hypoplasia of the thenar muscles is almost universally associated with Type II deformities, further hindering opposition. Furthermore, 60% of these patients have significant first web space contractures.
Transitional Type (Buck-Gramcko)
Buck-Gramcko described a transitional variant in which a trapezoidal extra phalanx causes both an increase in thumb length and a marked angular deformity.
SURGICAL MANAGEMENT OF THE TRIPHALANGEAL THUMB
Indications and Timing of Surgery
While nonoperative treatment (e.g., splinting) cannot correct the osseous deformity, operative intervention is not strictly mandatory for all children, particularly those with very mild Type I deformities without functional impairment. However, for the vast majority, surgery is indicated.
The primary goals of operative treatment are:
1. Correction of angular deformity.
2. Restoration of normal thumb length.
3. Correction of first web space contracture.
4. Improvement of opposition and pinch kinematics.
Treatment of Type I Deformities (Delta Phalanx)
Historically, removal of the abnormal delta phalanx along with reconstruction of the collateral ligament was advocated during the first year of life. The rationale was that early excision allows remodeling of the joint surfaces and provides adequate stability. However, long-term follow-up studies have demonstrated an unacceptably high rate of late joint instability and recurrent angular deformity following simple excision and ligamentous reconstruction.
To mitigate this risk, the Peimer Reduction Osteotomy is now the preferred technique. This procedure corrects the angulation deformity by resecting the abnormal physis and creating a closing wedge, thereby realigning the digit with a significantly lower chance of ligamentous instability.
🚨 Surgical Warning
The Peimer osteotomy is highly dependent on physeal visualization. It is best performed when the child is 24 to 30 months old, at which point the physis of the delta phalanx is clearly visible and ossified on standard radiographs, allowing for precise surgical targeting.
Peimer Reduction Osteotomy: Step-by-Step Technique
Step A: Surgical Exposure
Make a dorsal longitudinal or slightly curved incision over the affected interphalangeal joint to expose the extensor mechanism and the underlying delta phalanx.

Step B: Narrowing of the Distal Phalanx
Carefully dissect the extensor mechanism. Identify the broad, abnormal articulation. Use a scalpel or fine osteotome to narrow the base of the distal phalanx, matching its width to the proximal articular surface to prevent postoperative joint prominence.

Step C: Excision of the Distal Epiphysis
Identify the abnormal, bracketed epiphysis of the delta phalanx. Carefully excise this distal epiphysis to arrest the asymmetric growth that drives the progressive clinodactyly.

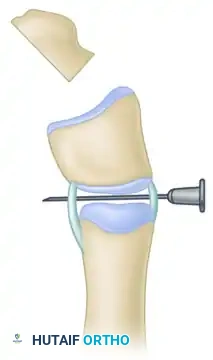
Step D: Orientation for Osteotomy
Place a hypodermic needle (e.g., 22-gauge) transversely across the interphalangeal joint. This serves as a critical visual and radiographic marker to orient the subsequent transverse osteotomy parallel to the joint line.
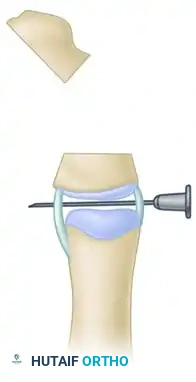
Step E: Completion of the Osteotomy
Using a fine oscillating saw or sharp osteotome, complete the transverse osteotomy through the delta phalanx, utilizing the needle as a guide to ensure the cut is perfectly parallel to the joint surface.
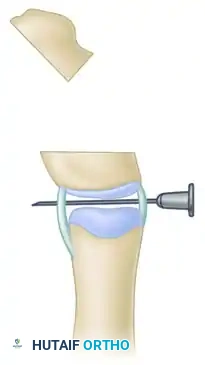
Step F: Closing Wedge Formation
The combined osteotomies (the initial physeal excision and the transverse cut) effectively form a closing wedge. Reduce the osteotomy by closing the wedge; this simultaneously shortens the abnormally long segment and realigns the longitudinal axis of the thumb.
Step G: Osseous Fixation
Secure the realigned bone ends with one or two smooth longitudinal Kirschner wires driven across the osteotomy site and the adjacent joint. These wires are typically left in place for 4 to 6 weeks until radiographic union is achieved.

Late Instability: If a patient presents late with severe instability following a previous failed excision, arthrodesis of the interphalangeal joint is the salvage procedure of choice, providing a stable post for pinch.
Treatment of Type II Deformities (Five-Fingered Hand)
The Type II deformity represents a profound functional deficit due to the lack of opposition and the presence of a severe first web space contracture. The treatment of choice is formal pollicization of the radialmost digit, as popularized by Buck-Gramcko.
Pollicization involves:
1. Shortening: Resection of the extra phalanx or metacarpal shortening to achieve normal thumb length.
2. Rotation: Pronating the digit 120 to 160 degrees to face the pulp of the index and middle fingers.
3. Abduction: Positioning the digit in 40 degrees of palmar abduction.
4. Muscle Stabilization: Reconstructing the intrinsic musculature to stabilize the new basal joint and provide active opposition.
Addressing Web Space and Thenar Hypoplasia
* Web Space Release: Contracture of the first web space is ubiquitous. Mild to moderate contractures may be released with a four-part Z-plasty (Woolf and Broadbent). Severe contractures require a dorsal rotation flap (Strauch and Spinner) to recruit adequate skin
📚 Medical References
- triphalangeal thumb, J Hand Surg 3:436, 1978.
- Buck-Gramcko D: Pollicization of the index fi nger: method and results in aplasia and hypoplasia of the thumb, J Bone Joint Surg 53A:1605, 1971.
- El-Karef E: The non-opposable triphalangeal thumb: a new technique for management, J Hand Surg 29B:544, 2004.
- Ezaki M: Radial polydactyly, Hand Clin 6:577, 1990.
- Lamb DW: The practice of hand surgery, 2nd ed, Oxford, 1989, Blackwell Scientifi c. Milch H: Triphalangeal thumb, J Bone Joint Surg 33A:692, 1951.
- Miura T: Triphalangeal thumb, Plast Reconstr Surg 58:587, 1976.
- Peimer CA: Combined
