DEFINITION
The thumb-in-palm deformity is a fixed adduction-flexion posture in the affected hand of the patient with spastic cerebral palsy. This influences both hand function and hygiene.
ANATOMY


FIG 1 • Thumb-in-palm deformity (A) demonstrating MCP laxity and hyperextension (B).
PATHOGENESIS
Cerebral palsy is permanent disorder of the development of movement and posture, causing activity limitation, attributed to a nonprogressive neurologic disturbance that occurred in the developing fetal or infant brain. Thedisorders of cerebral palsy are often accompanied by disturbances of sensation, perception, and cognition.11The musculoskeletal findings develop secondarily. Spasticity initially results in shortening of the myotendinous unit and ultimately secondary contractures.Paresis of muscles may contribute to greater deformity when spastic muscles are unopposed. The ultimate deformity depends on the overall imbalance.
NATURAL HISTORY
A supple thumb-in-palm posture is a normal finding in infants during the first year. Persistence of a tightly closed thumb in palm longer than 1 year is abnormal and should be evaluated.3The deformity is usually correctable at first and then progresses to a fixed deformity as myostatic contracture develops.A progressive and variable-size discrepancy of the involved limb may develop, resulting in a smaller thumb.1 The lack of thumb extension and abduction can impair hand grip, function, appearance, and hygiene.
PATIENT HISTORY AND PHYSICAL FINDINGS
A complete history and physical examination of a child with cerebral palsy should be done carefully and thoroughly.Input from other professionals such as neurologists and occupational therapists is often helpful.Associated deformities of the spastic upper extremity such as finger and wrist flexion, forearm pronation, elbow flexion, and shoulder adduction and internal rotation should also be evaluated. Surgical treatment of thumb-in-palm deformity may be only one part of surgical care of the involved extremity.Thumb muscle involvement, motion, and stability should be evaluated in the physical examination before organizing the treatment plan.Individual muscle involvement is detected by observing thumb position and palpating spastic or contracted muscles (Table 1). As spasticity is rate-dependent tone, slow gradual stretch should be able to overcome this force, unlike a contracture which is a fixed shortening of a muscle tendon unit or joint.Motion and stability are assessed by passive and active range of thumb abduction-adduction, flexion-extension, and palmar abduction and opposition.P.1362 Table 1 Grading of Thumb-in-Palm Deformity
CLASSIFICATION
DEGREE OF DEFORMITY
ILLUSTRATION
HOUSE TONKIN
(1981) (2001) DESCRIPTION





The pattern of voluntary grasp and release of large objects and manipulation of small objects should be determined by observing the child during functional activities.Sensory deficits impair function. Assessment of sensation should include stereognosis.Repeated observation or videotaping of the child during various activities can also be useful for accurate evaluation. This can be particularly valuable in detecting dystonia.Lower extremity function and need for intervention should be considered and coordinated appropriately.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Electrophysiologic testing and selective nerve blocks may help in localizing involved muscles and identifying muscles available for tendon transfers.Select nerve blocks may help differentiate between spastic, spared, and fibrotic muscles.Dynamic electromyography (EMG) with motion analysis may offer important information for planning tendon transfer surgery.5Radiographs may reveal thumb joint instability or growth disturbance.
DIFFERENTIAL DIAGNOSIS
Clasped thumb Distal arthrogryposisApparent absence of thumb extensor (faux extensor agenesis)
MANAGEMENT
The goals of treatment need to be clearly defined.No peripheral intervention will overcome the fundamental central nervous system etiology.P.1363For many patients, the goal will be to improve thumb position for function; however, there is a subset of highly involved patients for whom improved hygiene alone may the goal.
NONOPERATIVE MANAGEMENT
Use of tone-reducing medication such as botulinum toxin to the AP can soften the deformities and improve joint range of motion for nonoperative management.4In mild, nonrigid deformity, nonoperative treatment with orthoses may help in maintaining thumb abduction and improve hand function,13 but too-rigid splinting may result in limited thumb motion.
SURGICAL MANAGEMENT
The principles of surgery for thumb-in-palm deformity are the following2:Release of spastic muscles or contractures Augmentation of paretic muscles Stabilization of unstable thumb jointsRelease of contracture with or without augmentation of weak muscles aims to rebalance the thumb muscles, depending on the pattern of motor dysfunction of the thumb and the patient's degree of voluntary control.Release of spastic muscle or myostatic contractures can be performed by intrinsic muscle release of the AP, FPB, APB, and first dorsal interosseous.Extrinsic muscle release of the FPL may be considered if it is affected.Secondary skin and fascial contracture of the first web space need to be addressed by four-flap or double-opposing Z-plasty.Augmentation of paretic thumb abduction and extension can be accomplished by a combination of tenodesis and tendon rerouting or transfers and depends on the specific deficit, the muscles available, and the extent of voluntary control of selected muscles.Thumb MCP joint arthrodesis or sesamoid capsulodesis should be considered for stabilizing the thumb MCP joints when the joint remains unstable.2These joint stabilization procedures can also enhance tendon transfer procedures for extension-abduction.Thumb MCP joint arthrodesis is considered when tendon transfer fails to correct the deformities or when sesamoid capsulodesis cannot control the hyperextension of the MCP joint.1Thumb carpometacarpal (CMC) joint stabilization is indicated when metacarpal adduction cannot be controlled. CMC fusion, which preserves scaphotrapezial motion, is preferable to the rigid intermetacarpalfusion.2Thumb IP joint fusion is usually not necessary, but this procedure may be indicated when the IP joint flexion contracture is severe or in the rare event of an FPL rupture after lengthening.2Neurectomy may be an adjunct procedure for a clenched fist deformity in a hand with no active movement and difficulty with passive hand function including hygiene9; however, its role is limited.Table 2 lists surgical options for treating thumb-in-palm deformity.14 Table 2 Surgical Options for Correcting Thumb-in-Palm Deformity
RELEASES
Adductor release in palm Adductor tenotomyFirst dorsal interosseous release FPB releaseFPL slide First web skin and fascia release Augmentation of APL, EPL, EPB using Brachioradialis FDSPLEPL to EPB FCR or FCU ECRL
APL TENODESIS
Through radius to brachioradialis, ECRL, FCR through first dorsal compartment
JOINT STABILIZATION
CMC joint fusionMCP joint sesamoid capsulodesis MCP joint fusionIP joint fusionFPB, flexor pollicis brevis; FPL, flexor pollicis longus; APL, adductor pollicis longus; EPL, extensor pollicis longus; EPB, extensor pollicis brevis, FDS, flexor digitorum superficialis; PL, pollicis longus; FCR, flexor carpi radialis; FCU, flexor carpi ulnaris; ECRL, extensor carpi radialis longus; CMC, carpometacarpal; MCP, metacarpophalangeal; IP, interphalangeal. (Adapted from Tonkin MA. Thumb deformity in the spastic hand: classification and surgical techniques. Tech Hand Up Extrem Surg 2003;7:18-25.)
PREOPERATIVE PLANNING
Comprehensive evaluation is necessary with a multispecialty approach.Surgery should be done when the central nervous system has matured and the child is old enough to cooperate with postoperative therapy—usually at least 5 to 6 years old.6Associated abnormalities (eg, seizures, mental status problems) should be assessed and the management optimized before surgery is contemplated.Patient understanding and emotional readiness as well as family and social support should be addressedbefore surgery.Physical examination under anesthesia is crucial. This can differentiate spastic from myostatic conditions and can accurately evaluate the stability of thumb joints.
POSITIONING
The patient is placed in the supine position, and surgery is performed under general anesthesia and tourniquet control.
APPROACH
Surgical approaches for thumb-in-palm deformity depend on the objectives.Release of static or long-standing intrinsic contracture is usually performed through a curved incision located over the line of the thenar crease to release the origin of the AP with or without the origin of the FPB.8Release of a simple intrinsic contracture may be performed through the first web space approach to release the AP and the first dorsal interosseous muscle, combined with four-flapor double-opposing Z-plasty to release the secondary web space contracture.2P.1364A surgical approach by a small incision over the volar aspect of the distal forearm is used for extrinsic release of the FPL tendon, if necessary.A dorsal approach to the thumb and a dorsoradial approach over the wrist is used for augmentation of thumb extensors, with a volar-radial approach being used for augmentation of the thumb abductor.
TECHNIQUE
Release of Contractures
RELEASE OF CONTRACTURES
RELEASE OF STATIC INTRINSIC CONTRACTURE



TECH FIG 1 • Intrinsic release. A. A curved incision is made over the thenar crease. B. Thenar release showing motor branch. C,D. Thumb intrinsics are released. The FPB origin at the transverse carpal ligament and trapezium may also be released if this muscle limits abduction and extension of the thumb ray.The first dorsal interosseous may be released at the distal portion of the muscle from the ulnar aspect of the first metacarpal if needed to obtain adequate passive abduction and extension of the thumb.
RELEASE OF SIMPLE INTRINSIC CONTRACTURE


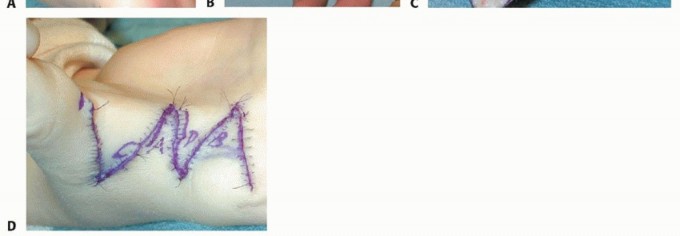
TECH FIG 2 • Four-flap Z-plasty over first web space. A,B. Skin markings. C. Elevation of flaps and adductor exposure. D. After rotation of skin flaps.
RELEASE OF EXTRINSIC CONTRACTURE
A small longitudinal incision over the distal-volar aspect of the forearm is performed. The FPL tendon is exposed and incised over the musculotendinous portion.The thumb IP joint is hyperextended until 1 cm of distal sliding of the FPL tendon is identified.The FPL may be lengthened by Z-lengthening of the FPL tendon, with 0.5 mm of lengthening for each degree of correction.11. Augmentation of Weak Muscles
ABDUCTOR POLLICIS LONGUS AUGMENTATION

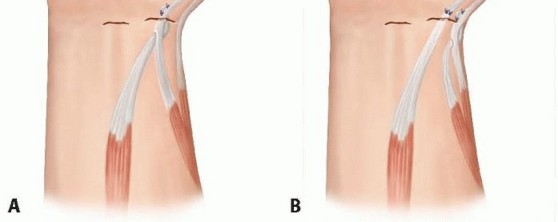
TECH FIG 3 • A. Transfer of PL to translocated APL by end-to-side anastomosis. B. APL augmentation by rerouting of the distal segment and anastomosis with end-to-end pollicis longus or end-to-side FCR. Thumb MCP joint extension is augmented by anastomosis of the proximal segment of APL with end-to-side EPB. P.1366
EXTENSOR POLLICIS LONGUS REROUTING
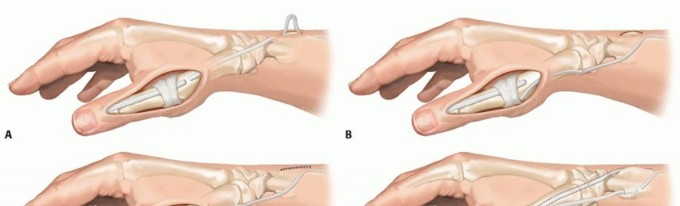
TECH FIG 4 • EPL rerouting. A. EPL tendon is divided distally and mobilized. B. The tendon is rerouted to the radial aspect of the Lister tubercle and passed subcutaneously around the APL and EPB tendon. C. The rerouted EPL is sutured back to the extensor mechanism. D. Modified EPL rerouting technique. The EPL tendon is divided proximal to the Lister tubercle, rerouted to the first extensor compartment, and sutured back to the proximal stump. E,F. EPL routing to the retinaculum. E. The EPL tendon is released from the third extensor compartment and rerouted radially. F. The new pulley for the rerouted EPL is created from the extensor retinaculum. The thumb is set in appropriate abduction and IP extension. The rerouted EPL is sutured back to the extensor mechanism 10 mm distal to the defect.The rerouted EPL may be reinforced by the transfer of the PL, FCR, or brachioradialis.The EPL may be divided proximal to the Lister tubercle, leaving the tendon attached to its insertion. Rerouting is then performed from distal to proximal (TECH FIG 4D).10The EPL may be rerouted to the new pulley created from the extensor retinaculum (TECH FIG 4E,F).12. Stabilization of Thumb Metacarpophalangeal Joint
THUMB METACARPOPHALANGEAL JOINT ARTHRODESIS
A dorsoulnar incision is made over the thumb MCP joint.The extensor mechanism is split longitudinally, and the ulnar collateral ligament is then detached from the metacarpal head to expose the joint (TECH FIG 5A).The articular cartilage of the metacarpal head is removed with a scalpel, and the proximal phalanx epiphysis is shaved until the secondary center of ossification is exposed (TECH FIG 5B). This allows fusion of the epiphyses and preserves the physis.The joint is set in 10 degrees of flexion, 10 degrees of abduction, and slight pronation,12 and a small (1 mm in diameter), smooth Kirschner wire is passed through the joint centrally to minimize epiphyseal damage (TECH FIG 5C).
SESAMOID CAPSULODESIS
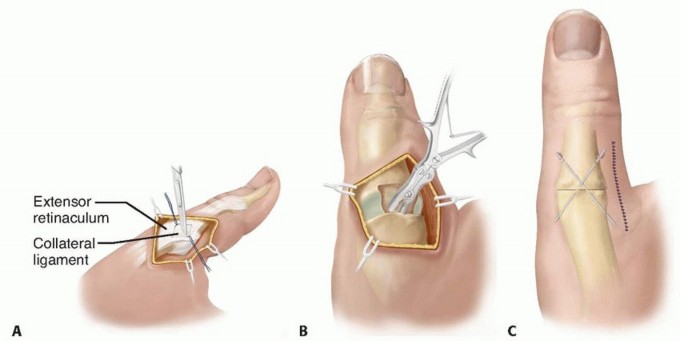
TECH FIG 5 • Thumb MCP arthrodesis. A. After the extensor mechanism over the MCP joint is split longitudinally, the ulnar collateral ligament is detached from the metacarpal head. B. The articular cartilage of the metacarpal head is removed. The epiphyseal plate of the proximal phalanx is preserved. C. After the joint is set, smooth Kirschner wires are used to maintain the joint position.
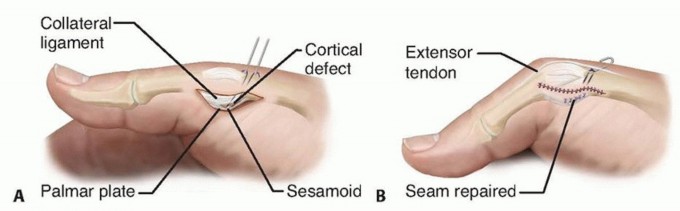
TECH FIG 6 • Sesamoid capsulodesis. The volar plate is mobilized to expose the radial sesamoid. The articular cartilage of the sesamoid is denuded corresponding with the cortical defect created at the head-neck junction of the metacarpal. A. The suture is passed through the sesamoid-volar plate and metacarpal defect. B. The intraosseous suture is tied over the dorsal surface of the metacarpal under the extensor tendons. A Kirschner wire is used to maintain the joint position. The MCP joint is set to 30 degrees of flexion. The intraosseous suture is then tied over the dorsal surface of the metacarpal under the extensor tendons to secure the sesamoid to the metacarpal neck.A Kirschner wire is passed through the joint to maintain the joint position for 6 weeks (TECH FIG 6B).
PEARLS AND PITFALLS
Generalapproach1. A comprehensive history and physical examination, including appropriateinvestigations with other professionals, should be done for accurate diagnosis and treatment planning.Patient selection1. Voluntary control of the selected muscle, which indicates the potential activeuse of the hand postoperatively, is important for selection of surgical candidates.Procedureselection1. The procedures must be individualized because of variation in deformities ineach patient.Release ofspastic muscle and contractures1. Selective release of the deforming forces is performed in sequential order toobtain adequate, functional thumb positions.2. Adjacent neurovascular structures must be protected with care.Augmentation ofparetic muscles1. The muscle selected for transfer depends on the availability and the extentof voluntary control.2. The stability of the MCP joint is evaluated before performing any augmentation procedures across it.Joint stabilization1. Joint stabilization is the key to success of rebalancing the thumb-deformingforces.2. The epiphyseal plate of the proximal phalanx must be preserved with care.P.1368
POSTOPERATIVE CARE
Postoperative care for contracture releases includes immobilization in a short-arm thumb spica cast maintaining full thumb radial abduction and 20 degrees of palmar abduction for 4 weeks.Removable splinting is then continued for another 4 to 6 weeks.If tendon transfer has been done, immobilization should be extended to 6 weeks, followed by additional splinting for 6 weeks. Dynamic splinting may be considered.Immobilization of the MCP arthrodesis with a thumb spica cast should be continued until radiographic healing is detected.
OUTCOMES
The functional outcome of thumb-in-palm deformity should be assessed before and after surgery by the physician, therapist, parent, and patient.House et al2 demonstrated improved functional grade in all 56 patients postoperatively. Half of patients improved three or more grades.Tonkin et al16 found good results in 32 patients after surgical correction of thumb-in-palm deformity. The average follow-up was 32 months (range, 10 to 88 months).The thumb was maintained out of palm in 29 of 32 patients (30 of 33 thumbs). Patients could perform lateral pinch in 26 of 33 thumbs.Many patients improved function, but no patient improved from dependent to independent functioning.
COMPLICATIONS
Inadequate release of contracted or fibrotic muscle may result in insufficient release of the thumb out of the palm.Adhesions along the transferred tendon may cause loss of excursion postoperatively.Improper techniques such as overlengthening and an incorrect vector of transfer may result in limited active abduction and extension of the thumb.Untreated or inadequate treatment of an unstable MCP joint may result in failed tendon transfer.Avoiding neurovascular injury is crucial. Care should be taken to properly identify and protect neurovascular bundles throughout surgery.An improper rehabilitation program and social support may result in failed treatment.
REFERENCES
- Goldner JL, Koman LA, Gelberman R, et al. Arthrodesis of the metacarpophalangeal joint of the thumb in children and adults. Adjunctive treatment of thumb-in-palm deformity in cerebral palsy. Clin Orthop Relat Res 1990;(253):75-89.
- House JH, Gwathmey FW, Fidler MO. A dynamic approach to the thumb-in-palm deformity in cerebral palsy. J Bone Joint Surg Am 1981;63(2):216-225.
- Jaffe M, Tal Y, Dabbah H, et al. Infants with a thumb-in-fist posture. Pediatrics 2000;105(3):E41.
- Koman LA, Mooney JF III, Smith B, et al. Management of cerebral palsy with botulinum A toxin: preliminary investigation. J Pediatr Orthop 1993;13:489-495.
- Kozin SH, Keenan MA. Using dynamic electromyography to guide surgical treatment of the spastic upper extremity in the brain-injured patient. Clin Orthop Relat Res 1993;(288):109-117.
- Lawson RD, Tonkin MA. Surgical management of the thumb in cerebral palsy. Hand Clin 2003;19:667-677.
- Manske PR. Redirection of extensor pollicis longus in the treatment of spastic thumb-in-palm deformity. J Hand Surg Am 1985;10(4): 553-560.
- Matev IB. Surgical treatment of flexion-adduction contracture of the thumb in cerebral palsy. Acta Orthop Scand 1970;41:439-445.
- Pappas N, Baldwin K, Keenan MA. Efficacy of median nerve recurrent branch neurectomy as an adjunct to ulnar motor nerve neurectomy and wrist arthrodesis at the time of superficialis to profundus transfer in prevention of intrinsic spastic thumb-in-palm deformity. J Hand Surg Am 2010;35(8):1310-1316.
- Rayan GM, Saccone PG. Treatment of spastic thumb-in-palm deformity: a modified extensor pollicis longus tendon rerouting. J Hand Surg Am 1996;21(5):834-839.
- Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl 2007;109:8-14.
- Swanson AB. Surgery of the hand in cerebral palsy. In: Flynn JE, ed. Hand Surgery. Baltimore: Williams & Wilkins, 1982:476-488.
- Ten Berge SR, Boonstra AM, Dijkstra PU, et al. A systematic evaluation of the effect of thumb opponens splints on hand function in children with unilateral spastic cerebral palsy. Clin Rehabil 2012;26(4): 362-371.
- Tonkin MA. Thumb deformity in the spastic hand: classification and surgical techniques. Tech Hand Up Extrem Surg 2003;7:18-25.
- Tonkin MA, Beard AJ, Kemp SJ, et al. Sesamoid arthrodesis for hyperextension of the thumb metacarpophalangeal joint. J Hand Surg Am 1995;20(2):334-338.
- Tonkin MA, Hatrick NC, Eckersley JR, et al. Surgery for cerebral palsy part 3: classification and operative procedures for thumb deformity. J Hand Surg Br 2001;26(5):465-470.
- Zancolli EA, Zancolli E Jr. Surgical rehabilitation of the spastic upper limb in cerebral palsy. In: Lamb DW, ed. The Paralyzed Hand. Edinburgh: Churchill Livingstone, 1987:153-168.
