PATHOMECHANICS AND CLINICAL EVALUATION OF SEVERE DEFORMITY
The correction of a severe hammer toe deformity represents a complex biomechanical challenge in forefoot reconstruction. By definition, a severe deformity is characterized by a rigid, fixed extension contracture at the metatarsophalangeal (MTP) joint coupled with a fixed flexion contracture at the proximal interphalangeal (PIP) joint. Because the deformity is fixed at both centers of rotation, isolated procedures at the PIP joint (such as arthrodesis or resection arthroplasty) will fail to correct the global alignment of the digit. Both joints require systematic, sequential correction to restore a plantigrade, functional forefoot.
The pathoanatomy is driven by a dynamic imbalance between the intrinsic and extrinsic musculature. As the intrinsic muscles (lumbricals and interossei) fail or are overpowered, the extensor digitorum longus (EDL) exerts an unopposed extension force on the proximal phalanx via the extensor sling. Over time, this chronic hyperextension leads to attenuation and eventual rupture of the plantar plate, collateral ligament contracture, and dorsal subluxation or frank dislocation of the MTP joint. Concurrently, the flexor digitorum longus (FDL) and flexor digitorum brevis (FDB) pull the PIP joint into rigid flexion.
💡 Clinical Pearl: The Sequential Release
The cornerstone of correcting severe MTP joint extension contractures is the sequential soft tissue release. The surgeon must reassess the resting posture of the toe after each anatomic structure is released. Over-releasing can lead to a destabilized "floating toe," while under-releasing guarantees recurrence.
SURGICAL ANATOMY AND PREOPERATIVE PLANNING
A thorough understanding of the dorsal extensor apparatus is mandatory. The extensor digitorum brevis (EDB) tendon lies slightly fibular and deep to the EDL tendon. The EDB joins the EDL and the extensor expansion at the level of the metatarsal neck. Recognizing this confluence is critical, as the EDB must be addressed prior to lengthening the EDL to achieve adequate excursion.
The MTP joint capsule itself may present highly variable pathology. In chronic deformities with recurrent synovial inflammatory episodes (often seen in rheumatoid arthritis or severe degenerative joint disease), the capsule transforms from a thin, pliable synovial layer into a dense, thick, fibrous encapsulation that rigidly tethers the joint in extension.
Indications for Surgery
- Fixed extension contracture of the MTP joint (>20 degrees) unresponsive to conservative care.
- Fixed flexion contracture of the PIP joint with overlying painful adventitial bursitis or ulceration.
- Dorsal subluxation or dislocation of the MTP joint.
- Intractable plantar keratosis (IPK) beneath the affected metatarsal head due to retrograde plantarflexion forces from the dislocated proximal phalanx.
SURGICAL TECHNIQUE: STEP-BY-STEP CORRECTION
1. Incision and Exposure
Begin the procedure at the metatarsophalangeal joint. The approach must provide extensile exposure to the extensor apparatus and the dorsal MTP joint capsule without compromising the vascular supply to the dorsal skin flaps.
Make a straight or slightly angled longitudinal incision centered over the fibular aspect of the metatarsophalangeal joint.

Diagrammatic representation of the incision placement over the fibular aspect of the MTP joint.

Clinical photograph demonstrating the planned surgical incision.
Carefully deepen the incision through the dermis. You will encounter branches of the dorsal venous arch returning from the toe. These must be meticulously cauterized or gently retracted to expose the underlying extensor tendons. Failure to control these vessels will result in a bloody surgical field that obscures the delicate extensor expansion.
2. Extensor Tendon Management
Identify the extensor digitorum longus (EDL) and the extensor digitorum brevis (EDB). The EDB is located slightly fibular and deep to the EDL. Trace both tendons distally to the neck of the metatarsal, where the EDB joins the EDL and the extensor expansion.
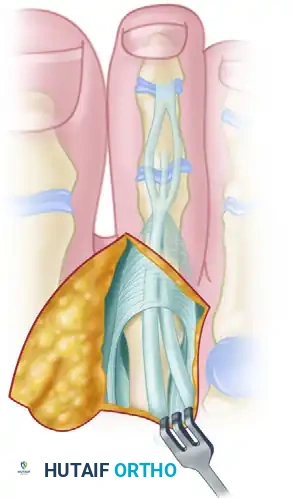
Diagram illustrating the anatomic relationship between the EDB (fibular/deep) and the EDL.

Clinical exposure of the extensor tendons prior to surgical lengthening.
Before this confluence, dissect the EDB away from the EDL. Perform a tenectomy by removing a 2- to 3-mm segment of the extensor digitorum brevis. This eliminates the secondary deforming extension force.
🔪 Surgical Technique: EDL Z-Plasty Lengthening
- Perform a Z-plasty lengthening of the extensor digitorum longus. The use of a small, precise blade (such as a No. 67 Beaver blade or a similar fine cutting edge) is highly recommended to avoid fraying the tendon.
- From the proximal part of the skin incision, make a longitudinal split down the center of the EDL tendon, continuing distally until the EDL joins with the extensor expansion.
- Exit the longitudinal incision at a right angle at the distal junction (extensor expansion).
- Sever the tendon proximally at a right angle in the opposite direction to complete the "Z".
- Lift the tendon away from any remaining soft tissue attachments. This maneuver effectively lengthens the EDL by 8 to 12 mm.
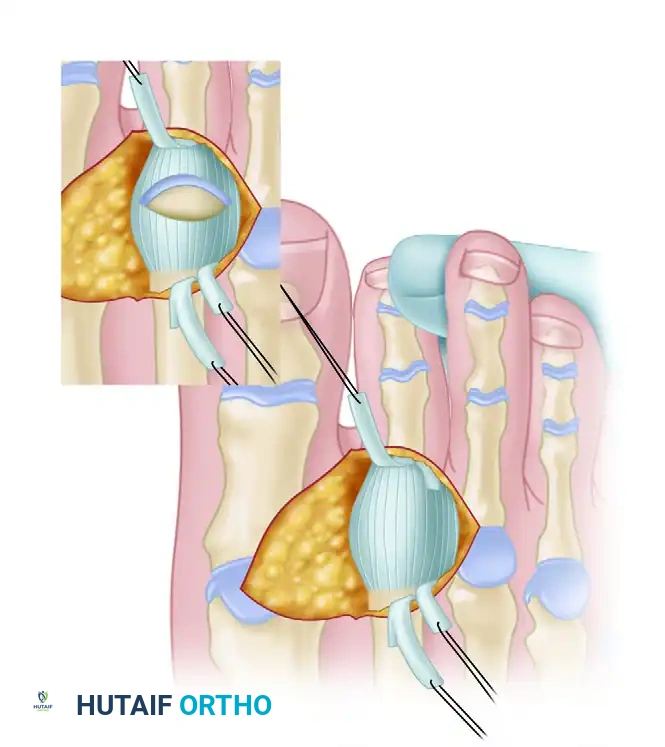
Diagram of the Z-plasty lengthening of the extensor digitorum longus.
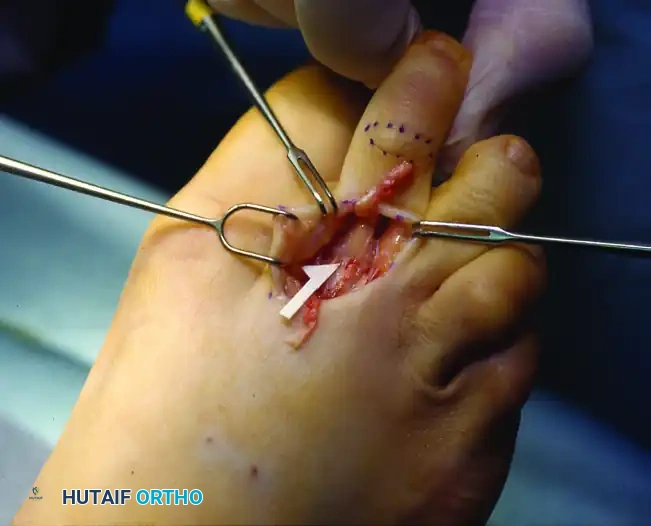
Clinical execution of the EDL Z-plasty, demonstrating the achieved length.
3. Intraoperative Assessment and Sequential Release
Once the EDL is lengthened, the surgeon must assess the degree of remaining contracture.
Scenario A: Mild Residual Contracture
If the extension contracture is now less than 20 to 30 degrees, and there is absolutely no dorsal subluxation of the proximal phalanx on the metatarsal head, firmly flex the toe 30 to 40 degrees. Load the foot by holding the ankle at 90 degrees (neutral). If the toe rests in a neutral position at the MTP joint, no further capsular release is required. The EDL will be sutured in its lengthened position (using 3-0 or 4-0 absorbable suture) only after the PIP joint deformity has been fully corrected.
Scenario B: Moderate Residual Contracture (The Dorsal Capsulotomy)
If the toe still rests in 10 to 20 degrees of extension after the Z-plasty, a dorsal capsulotomy is indicated.
1. Firmly flex the toe 40 to 50 degrees. This acute flexion pulls the extensor expansion distally, providing superior exposure of the dorsal capsule.
2. Perform a transverse dorsal capsulotomy.
3. Return the ankle to 90 degrees and observe the resting posture. If the posture is acceptable (neutral to 10 degrees of MTP extension), proceed to PIP correction and subsequent EDL repair.

Clinical photograph demonstrating the transverse dorsal capsulotomy performed with the toe in acute flexion.
Scenario C: Severe Residual Contracture (Collateral Ligament Release)
If the toe still exhibits an unacceptable extension posture despite the capsulotomy, the collateral ligaments are acting as the primary tethers.
1. Acutely flex the toe to place the collateral ligaments under tension.
2. Using a small blade, carefully incise the collateral ligaments on both the medial and lateral sides of the metatarsal head.
3. Surgical Warning: Carry the incision down to, but not through, the plantar plate of the metatarsophalangeal joint. Transecting the plantar plate will lead to catastrophic dorsal instability.
4. This release should allow the toe to assume a neutral to slightly flexed position at the MTP joint, even in cases of prior dorsal subluxation.
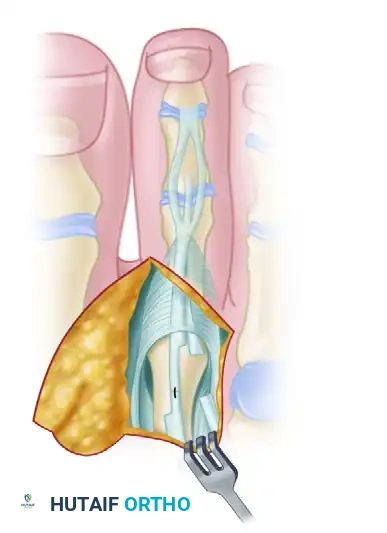
Diagram showing the release of the collateral ligaments down to the plantar plate.
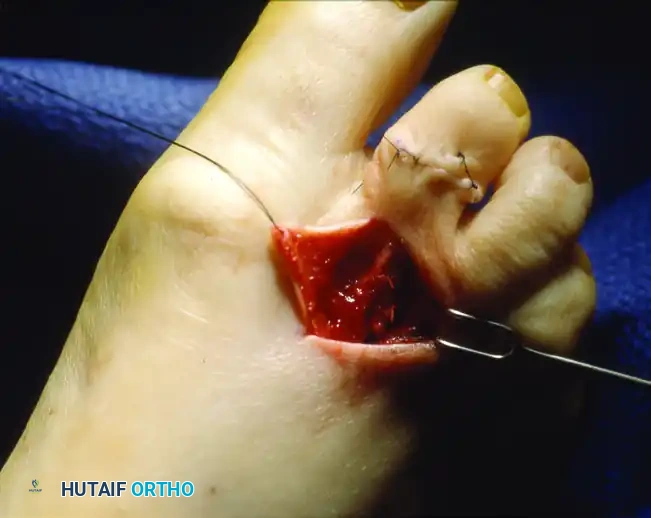
Clinical photograph of the collateral ligament release, allowing for complete reduction of the MTP joint.
CORRECTION OF SEVERE DEFORMITY WITH DISLOCATION OF THE MTP JOINT
Severe deformity accompanied by frank dislocation of the metatarsophalangeal joint is notoriously difficult to correct and maintain. The soft tissue envelope is severely contracted dorsally and attenuated plantarly.
All of the aforementioned sequential steps are strictly applicable and must be performed:
1. Extensor digitorum brevis tenotomy.
2. Extensor digitorum longus Z-plasty lengthening.
3. Transverse dorsal capsulotomy.
4. Bilateral collateral ligament release.
However, in the presence of a chronic dislocation, soft tissue release alone is insufficient. The joint space has contracted, and attempting to force the proximal phalanx back over the metatarsal head will result in excessive joint pressure, stiffness, and inevitable recurrence. Decompression of the metatarsophalangeal joint is absolutely required.
Osseous Decompression Strategies
Decompression can theoretically be performed on either the phalangeal or the metatarsal side of the joint.
🚨 Surgical Pitfall: Resection of the Proximal Phalanx Base
Resecting the base of the proximal phalanx is not preferred and should generally be avoided. Removing the base of the phalanx destroys the insertion of the intrinsic musculature and the plantar plate (the windlass mechanism). This makes it exceedingly difficult to maintain the position of the toe, even with prolonged K-wire fixation. Furthermore, it highly increases the probability of a transfer lesion, specifically a metatarsal head plantar callus developing laterally due to the loss of the toe's weight-bearing function.
Instead, decompression must be achieved on the metatarsal side of the joint. This is accomplished via:
1. Metatarsophalangeal Joint Arthroplasty / Metatarsal Head Contouring: Reshaping the metatarsal head to reduce its dorsal-plantar and medial-lateral dimensions, allowing the phalanx to reduce without tension.
2. Shortening (Weil) Osteotomy: A distal oblique osteotomy of the metatarsal neck/head parallel to the plantar surface. This allows the metatarsal head to slide proximally, effectively shortening the bone and decompressing the joint without altering the plantar pressure mechanics negatively.

Diagram demonstrating the initial assessment for metatarsal head contouring in a dislocated MTP joint.

Diagram showing the completed resection and contouring of the metatarsal head, allowing for tension-free reduction of the proximal phalanx.
FINAL CLOSURE AND POSTOPERATIVE PROTOCOL
Once the MTP joint is fully reduced and decompressed, attention is turned to the PIP joint (typically addressed via a resection arthroplasty or arthrodesis, depending on surgeon preference and deformity rigidity).
Only after the PIP joint is stabilized should the EDL be repaired. Suture the EDL in its new, lengthened position using a 3-0 or 4-0 absorbable suture. Ensure the ankle is held at 90 degrees during this repair to set the appropriate resting tension.
Fixation and Postoperative Care
- Pinning: The reduced MTP joint and corrected PIP joint are typically stabilized with a smooth 0.045-inch or 0.062-inch Kirschner wire driven retrograde from the tip of the toe, across the PIP and MTP joints, and into the metatarsal shaft.
- Dressing: A compressive forefoot dressing is applied to maintain alignment and control postoperative edema.
- Weight-Bearing: Patients are generally allowed heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe.
- Pin Removal: The K-wire is typically removed in the clinic at 4 to 6 weeks postoperatively, provided clinical alignment is maintained and any osseous procedures (like a Weil osteotomy) show early signs of consolidation.
-
Rehabilitation: Following pin removal, aggressive passive and active plantarflexion exercises of the MTP joint are initiated to prevent dorsal contracture recurrence and stiffness. Taping the toe in slight plantarflexion for an additional 4 to 6 weeks is highly recommended to allow the plantar plate to scar in a shortened position.
