Introduction & Epidemiology
Coronoid fractures, frequently underestimated and often missed in the initial evaluation of elbow trauma, represent critical injuries that significantly compromise elbow stability. While historically considered minor avulsions, a deeper understanding of elbow biomechanics has revealed the profound role of the coronoid process as a primary anterior and varus/valgus stabilizer, alongside its contribution to resisting posterior subluxation. Consequently, missed or inadequately treated coronoid fractures are a leading cause of chronic elbow instability, stiffness, and post-traumatic arthrosis.
These fractures rarely occur in isolation, typically presenting as part of more complex injury patterns such as:
*
Terrible Triad Injuries (TTI):
Characterized by elbow dislocation, radial head fracture, and coronoid process fracture. The coronoid fracture is the "unstable" component, dictating the need for surgical stabilization to restore concentric reduction.
*
Trans-olecranon Fracture-Dislocations:
Involving an olecranon fracture, often with an associated coronoid fracture and anterior displacement of the forearm relative to the humerus.
*
Posteromedial Rotatory Instability:
Often linked to anteromedial coronoid facet fractures, particularly those involving the sublime tubercle, which is the insertion site of the anterior bundle of the medial collateral ligament (MCL).
*
Varus Posteromedial Rotatory Instability (VPMRI):
A specific pattern involving an anteromedial coronoid fracture, disruption of the lateral ulnar collateral ligament (LUCL) complex, and posteromedial displacement of the ulna.
Epidemiologically, elbow dislocations account for 10-25% of all elbow injuries. Coronoid fractures are identified in approximately 2-10% of all elbow fractures and are present in up to 50% of elbow dislocations. The true incidence is likely higher due to underdiagnosis on plain radiographs. Advanced imaging, particularly computed tomography (CT) scans with 3D reconstructions, has significantly improved detection rates, highlighting their common presence in complex elbow trauma. The clinical significance of coronoid fractures is directly proportional to their size, location, and involvement of the anteromedial facet or the sublime tubercle.
Surgical Anatomy & Biomechanics
The coronoid process of the ulna is a critical osteoarticular structure forming the anterior beak of the semilunar notch, articulating with the trochlea of the humerus. Its intricate anatomy and ligamentous attachments are pivotal for elbow stability.
Anatomical Subdivisions
The coronoid process can be anatomically divided into three primary facets or regions, each with distinct biomechanical implications:
1.
Tip (Regan-Morrey Type I):
The most anterior and superior aspect, primarily providing anterior stability and attachment for the brachialis muscle. Fractures here are typically small avulsions.
2.
Anterolateral Facet:
Located lateral to the tip, contributing to the trochlear articulation.
3.
Anteromedial Facet (Regan-Morrey Type II/III, O'Driscoll Classification):
This is the most biomechanically significant portion. It encompasses the sublime tubercle, the primary attachment site for the anterior bundle of the medial collateral ligament (MCL). Fractures involving this facet are highly destabilizing, particularly against valgus and posteromedial rotatory forces. The anteromedial facet resists direct posterior translation and provides buttressing against varus and valgus stress.
Ligamentous and Muscular Attachments
- Brachialis Muscle: Inserts broadly onto the anterior aspect of the coronoid process, including the coronoid fossa. Its tendon provides dynamic anterior stability.
- Anterior Capsule: Attaches to the superior margin of the coronoid, reinforcing anterior stability.
- Medial Collateral Ligament (MCL): The anterior bundle of the MCL originates from the medial epicondyle and inserts firmly onto the sublime tubercle of the anteromedial coronoid. This ligament is the primary static stabilizer against valgus stress and a significant contributor to posteromedial rotatory stability.
- Lateral Collateral Ligament (LCL) Complex: While not directly attaching to the coronoid, its integrity, especially the lateral ulnar collateral ligament (LUCL), is crucial for posterolateral rotatory stability. Injury to the LUCL often coexists with coronoid fractures in terrible triad injuries, making comprehensive repair essential.
Biomechanical Role
The coronoid process acts as a crucial anterior buttress against posterior displacement of the ulna on the trochlea, particularly during axial loading and valgus stress. Its contribution to stability is directly proportional to its height and integrity.
*
Anterior Stability:
The coronoid prevents posterior subluxation of the ulna relative to the trochlea, especially during elbow flexion. Fractures that reduce the effective height of the coronoid render the elbow susceptible to recurrent posterior instability.
*
Varus/Valgus Stability:
The anteromedial facet, through its attachment to the MCL, is critical in resisting valgus stress. Fractures of the sublime tubercle or the anteromedial coronoid destabilize the elbow against valgus loads and posteromedial rotation.
*
Rotational Stability:
The interaction of the coronoid's shape with the trochlea, along with the MCL, resists excessive pronation and supination at certain degrees of flexion.
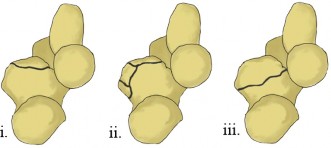
The Regan-Morrey classification, while widely used, has limitations as it primarily describes the size of the coronoid fracture, not necessarily its location or biomechanical significance.
*
Type I:
Avulsion of the tip.
*
Type II:
Fracture involving less than 50% of the coronoid height.
*
Type III:
Fracture involving more than 50% of the coronoid height.
The O'Driscoll classification is more specific, focusing on the location of the fracture and its implications for instability, especially the anteromedial facet fractures:
*
Type 1 (Tip):
Avulsion or small fragments.
*
Type 2 (Anteromedial facet):
Fractures involving the sublime tubercle or the entire anteromedial facet, highly associated with VPMRI.
*
Type 3 (Basal):
Larger fractures involving the entire base of the coronoid, often associated with trans-olecranon fracture-dislocations.
Understanding these anatomical and biomechanical principles is paramount for accurate diagnosis, appropriate treatment planning, and effective restoration of elbow stability.
Indications & Contraindications
The decision for operative versus non-operative management of coronoid fractures hinges on several factors: the stability of the elbow, the size and location of the fracture fragment, and the presence of associated injuries. The overarching goal is to restore a stable, concentrically reduced, and functional elbow joint.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management (Open Reduction Internal Fixation - ORIF) | Non-Operative Management (Conservative) |
|---|---|---|
| Elbow Stability | * Gross Elbow Instability: After initial reduction, the elbow remains unstable through a functional arc of motion (e.g., terrible triad injuries, VPMRI). | * Stable Elbow: After initial reduction, the elbow remains concentrically reduced and stable through a functional arc of motion (e.g., 30-130 degrees of flexion with no signs of subluxation). |
| Fracture Size | * Regan-Morrey Type II & III: Fractures involving >10-15% of the coronoid height, especially if displaced. | * Regan-Morrey Type I: Small avulsion of the coronoid tip (<10% height), non-displaced. |
| Fracture Location | * Anteromedial Facet Fractures: Especially those involving the sublime tubercle, regardless of size, due to MCL attachment and high risk of VPMRI. | * Isolated tip fractures not involving critical ligamentous attachments. |
| Displacement | * Displaced coronoid fragments that are amenable to fixation. | * Non-displaced or minimally displaced fragments (<2mm). |
| Associated Injuries | * Terrible Triad: Coronoid fracture requires fixation in conjunction with radial head fixation/replacement and LCL repair. | * Rarely an isolated injury; if associated injuries are managed non-operatively (e.g., stable radial head fracture), the coronoid may also be observed. |
| * Trans-olecranon Fracture-Dislocations: Requiring anterior buttress restoration. | ||
| * Open Fractures: Necessitating debridement and stabilization. | ||
| Patient Factors | * Younger, active patients requiring full elbow function. | * Elderly, low-demand patients with significant comorbidities, where risks of surgery outweigh benefits, provided stability is maintained. |
| * Patients with no significant contraindications to surgery. | * Patients medically unfit for surgery. |
Contraindications for Operative Management
Absolute contraindications are rare and typically relate to the patient's overall medical status rather than the fracture itself:
*
Severe Medical Comorbidities:
Patients with prohibitive surgical risks (e.g., severe cardiopulmonary disease, uncontrolled diabetes, active systemic infection).
*
Active Infection:
In the vicinity of the elbow, requiring initial treatment before elective surgery.
*
Severely Comminuted Coronoid Fragments:
Not amenable to stable fixation. In such cases, alternative strategies (e.g., radial head replacement to improve stability, external fixation, or hinged external fixator) may be considered, but direct coronoid reconstruction may be futile.
*
Severe Soft Tissue Compromise:
Precluding safe surgical access or increasing infection risk.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial for successful outcomes in complex coronoid fractures, allowing the surgeon to anticipate challenges and select the optimal approach and fixation strategy.
Pre-Operative Assessment & Imaging
- Clinical Evaluation: A detailed history of the injury mechanism, assessment for associated neurovascular compromise, and evaluation of elbow stability after initial reduction (if dislocated).
- Radiographic Series: Standard AP and lateral radiographs of the elbow are essential for initial diagnosis. However, coronoid fractures are often subtle or obscured by other bony injuries.
-
Computed Tomography (CT) Scan:
This is indispensable.
CT with thin cuts and 3D reconstructions provides invaluable information regarding:
- Fracture Morphology: Precise size, displacement, comminution, and number of fragments.
- Location: Identification of anteromedial facet involvement, especially the sublime tubercle.
- Associated Fractures: Radial head/neck, olecranon, humeral condyles.
- Implant Templating: Allows for selection of appropriate screw lengths, plate types, and radial head implants (if needed).
- Surgical Approach Planning: Determines the most appropriate approach (medial, lateral, or combined).
-
- MRI (Less common for acute fracture planning): May be considered if there is suspicion of significant ligamentous or soft tissue injury not clearly visualized on CT, especially in chronic instability or if occult LCL/MCL tears are suspected.
Pre-Operative Considerations
- Timing of Surgery: Ideally, surgery should be performed once swelling has subsided and the patient's medical condition is optimized, typically within 7-14 days. Early intervention is favored for unstable injuries to prevent progressive soft tissue contracture.
- Anesthesia: General anesthesia is standard. Regional blocks (e.g., interscalene block) can be a useful adjunct for post-operative pain management.
- Antibiotics: Pre-operative prophylactic antibiotics are administered.
- Tourniquet: A pneumatic tourniquet on the upper arm is routinely used for a bloodless field, typically inflated to 250-300 mmHg.
Patient Positioning
The optimal patient position depends on the planned surgical approach and associated injuries.
1.
Lateral Decubitus Position:
*
Advantages:
Allows access to both medial and lateral aspects of the elbow without repositioning. The arm can be freely draped over a padded arm support (e.g., chest roll or commercially available elbow positioner). Provides excellent visualization for combined approaches (e.g., terrible triad).
*
Setup:
Patient positioned with the affected arm superior, supported by an arm holder allowing for full flexion and extension. Axillary roll for neurovascular protection.
2.
Supine Position:
*
Advantages:
May be preferred for some medial approaches or if the patient's comorbidities preclude lateral positioning.
*
Setup:
Arm draped across the chest on a sterile arm board or supported by a hand table, allowing for manipulation. Access to the posterior elbow for olecranon fractures might be more difficult.
*

Regardless of positioning, careful padding of bony prominences and protection of neurovascular structures are paramount. A sterile tourniquet may be applied to the upper arm.
Detailed Surgical Approach / Technique
The choice of surgical approach for coronoid fractures is dictated by the fracture morphology (especially anteromedial facet involvement), the presence of associated injuries (radial head, olecranon, ligamentous), and surgeon familiarity. Often, a combination of approaches or extensile exposure is necessary.
General Principles of Coronoid Fixation
- Adequate Exposure: Obtain clear visualization of the fracture and associated soft tissue injuries.
- Identification of Associated Injuries: Address radial head fractures, olecranon fractures, and collateral ligament tears first, as their stabilization contributes to overall elbow stability and can aid in coronoid reduction.
- Fragment Mobilization: Carefully free the coronoid fragment(s) from soft tissue attachments, particularly the brachialis, while preserving any remaining periosteal or capsular attachments that might assist in reduction.
- Reduction: Restore anatomical alignment of the coronoid process to the ulna. This often requires direct visualization and gentle manipulation. Provisional K-wire fixation is frequently used.
- Stable Fixation: Employ appropriate fixation methods to achieve rigid internal fixation that can withstand early protected motion.
- Ligament Repair: Repair of the MCL and LCL is essential for restoring comprehensive stability.
Common Surgical Approaches
1. Medial Approach (Henry or Hotchkiss Modification)
This is the most common approach for anteromedial coronoid fractures, often combined with an olecranon osteotomy for extensive visualization.
- Incision: A curvilinear or straight incision is made between the medial epicondyle and the olecranon, extending proximally along the medial supracondylar ridge and distally along the ulnar border.
- Ulnar Nerve Identification & Protection: The ulnar nerve is identified posteriorly to the medial epicondyle, released from the cubital tunnel, and gently mobilized. It is then transposed anteriorly or protected posteriorly with a vessel loop throughout the procedure. Prophylactic anterior transposition is often performed to prevent post-operative irritation.
-
Internervous Plane:
- The flexor-pronator mass (originating from the medial epicondyle) is carefully elevated off the medial epicondyle and anterior capsule.
- Alternatively, the interval between the flexor carpi ulnaris (FCU) and the other flexors (flexor digitorum superficialis, FDS) can be developed.
- Deep dissection proceeds between the brachialis anteriorly and the pronator teres/FDS posteriorly.
- Capsular Exposure: The anterior capsule is visualized and incised if necessary, exposing the coronoid process. The MCL attachments (especially to the sublime tubercle) should be carefully assessed for avulsion or disruption.
- Coronoid Fracture Exposure: The brachialis muscle must be elevated or split to fully expose the coronoid fragments. Care is taken to preserve remaining soft tissue attachments to the fragments.
2. Lateral Approach (Kocher or Modified Kocher)
Primarily used for associated radial head fractures, this approach can provide limited access to the anterolateral coronoid but is not ideal for anteromedial fragments. It is often combined with a medial approach for terrible triad injuries.
- Incision: A longitudinal incision centered over the lateral epicondyle, extending proximally along the lateral supracondylar ridge and distally along the forearm.
- Internervous Plane: Dissection proceeds between the anconeus (posteriorly, innervated by radial nerve) and the extensor carpi ulnaris (ECU) or extensor digitorum communis (EDC) anteriorly (both innervated by the posterior interosseous nerve, PIN, a deep branch of the radial nerve).
- Capsular Exposure: The lateral collateral ligament complex is incised or elevated, exposing the radial head and capitellum. This approach can be extended to visualize the LUCL and its humeral origin.
3. Direct Anterior Approach (Limited Utility)
Generally avoided due to significant risk to neurovascular structures (brachial artery, median nerve, radial nerve). Rarely indicated for very specific, isolated coronoid tip fractures that cannot be accessed otherwise.
Reduction and Fixation Techniques
The goal is stable, anatomical reduction and fixation.
A. Suture Fixation / Suture Lasso Techniques
- Indications: Small avulsion fragments (Regan-Morrey Type I), highly comminuted fragments, or when screw/plate fixation is not feasible. Often used for anteromedial facet fractures involving the sublime tubercle where the MCL is avulsed with a small bone fragment.
-
Technique:
- A non-absorbable suture is passed through the fragment or around it (lasso technique).
- Drill holes are made in the ulna distal to the fracture (often through the ulna from posterior to anterior, or anteriorly with suture anchors).
- The sutures are then passed through these drill holes and tied over the posterior cortex of the ulna or secured to anterior suture anchors. This effectively pulls the fragment back into place.
- This technique is particularly useful for avulsion fractures of the sublime tubercle where the MCL remains attached to the fragment, providing stability through ligamentotaxis.
B. Screw Fixation (Lag Screws / Headless Compression Screws)
- Indications: Larger, non-comminuted fragments (Regan-Morrey Type II/III) that can be anatomically reduced and provide sufficient bone stock for screw purchase.
-
Technique (often from posterior to anterior):
- The coronoid fragment is reduced and provisionally stabilized with K-wires.
- A guidewire is drilled from the posterior cortex of the ulna, through the ulnar shaft, across the fracture site, and into the coronoid fragment.
- Careful trajectory is essential to avoid joint penetration and to achieve good purchase in the fragment. Fluoroscopy in multiple planes is critical.
- The appropriate length lag screw or headless compression screw is then inserted, compressing the fragment to the ulna.
- Multiple screws may be used depending on fragment size and geometry.
- Considerations: Requires adequate fragment size and bone quality. Potential for screw prominence into the joint if not properly countersunk or if headless screws are not fully buried.
C. Plate Fixation
- Indications: Larger, more complex, or comminuted coronoid fractures (Regan-Morrey Type II/III, O'Driscoll Type 2 & 3), especially those involving a significant portion of the base of the coronoid or anteromedial facet. Provides robust fixation and buttressing.
-
Technique:
- The fracture fragment(s) are reduced and provisionally fixed with K-wires.
- Mini-fragment plates (1.5mm or 2.0mm) or specifically designed coronoid plates (e.g., anteromedial coronoid plates) are contoured to the anatomy.
- The plate is applied to the anterior or anteromedial surface of the coronoid and secured with screws into the fragment and the ulnar shaft. Locking plates can be advantageous in osteoporotic bone or comminuted fractures.
- Plates act as a buttress, preventing posterior subluxation of the coronoid fragment.
- Considerations: Requires adequate exposure, meticulous plate contouring to prevent impingement, and careful screw placement to avoid neurovascular structures (especially with anterior plating) or joint penetration.
Addressing Associated Injuries
- Radial Head Fracture: Fixation with headless compression screws, plate fixation, or radial head replacement (arthroplasty) is performed.
- Olecranon Fracture: ORIF with tension band wiring or plate fixation. An olecranon osteotomy may be performed to improve exposure to the coronoid, which is then re-fixed.
- Medial Collateral Ligament (MCL) Repair: If the MCL is avulsed from the medial epicondyle or if a large capsular tear is present, it is repaired with suture anchors or direct sutures. If an anteromedial coronoid fracture involving the sublime tubercle is fixated, the MCL is indirectly stabilized.
- Lateral Collateral Ligament (LCL) Repair: Especially the LUCL, is crucial in terrible triad injuries. It is typically repaired with suture anchors to the lateral epicondyle or transosseous sutures.
Final Assessment
After fixation of all bony and ligamentous structures, the elbow stability is rigorously assessed.
*
Range of Motion:
Passively move the elbow through a full, stable arc of motion.
*
Stress Testing:
Apply gentle varus and valgus stress in full extension and at 30 degrees of flexion, as well as posterolateral rotatory stress, to confirm stability.
*
Imaging:
Intraoperative fluoroscopy confirms satisfactory reduction and hardware placement.
The goal is to achieve a stable, concentric reduction through the full arc of motion, ideally allowing for early protected rehabilitation.
Complications & Management
Coronoid fractures, especially when part of complex elbow instability patterns, are associated with a significant rate of complications. Proactive recognition and management are key to optimizing outcomes.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Description | Salvage Strategy / Management |
|---|---|---|---|
| Elbow Stiffness / Contracture | 20-50% (often requiring further intervention) | Limited range of motion (flexion/extension, pronation/supination) due to soft tissue contracture, heterotopic ossification, articular incongruity, or malunion. Common in complex elbow trauma. | * Aggressive Rehabilitation: Early and consistent, often with dynamic splinting. |
| * Manipulation Under Anesthesia (MUA): For severe cases where ROM plateaus, cautiously performed 3-6 months post-op. | |||
| * Surgical Release / Capsulectomy: Open or arthroscopic débridement of adhesions, release of contractures, excision of heterotopic ossification (if mature). | |||
| Persistent Instability | 10-30% (re-dislocation, subluxation) | Failure to restore adequate bony and ligamentous stability, often due to inadequate coronoid fixation, missed associated ligamentous injuries (MCL/LCL), or continued radial head instability. | * Revision Surgery: Re-evaluate CT/MRI. Address unaddressed components (e.g., redo coronoid fixation, radial head arthroplasty, primary or secondary ligament reconstruction, or use of a hinged external fixator). |
| * Hinged External Fixator: Provides temporary stability while soft tissues heal and may aid in motion. | |||
| Heterotopic Ossification (HO) | 10-40% (clinically significant in 5-10%) | Aberrant bone formation in periarticular soft tissues, leading to pain and severely restricted motion. Higher risk with severe trauma, head injury, prolonged immobilization. | * Prophylaxis: Indomethacin (NSAID) or low-dose radiation post-op, especially for high-risk patients. |
| * Excision: Surgical removal of mature HO, typically after 6-12 months when bone scan indicates quiescent HO. Often combined with capsular release. | |||
| Post-Traumatic Arthrosis | 10-25% (often long-term sequela) | Degenerative joint disease due to articular cartilage damage, incongruity, persistent instability, or malunion. Progressive pain, stiffness, and crepitus. | * Symptomatic Management: NSAIDs, physical therapy, activity modification. |
| * Débridement / Arthroscopy: For mechanical symptoms, loose bodies. | |||
| * Interposition Arthroplasty / Total Elbow Arthroplasty (TEA): For severe, debilitating end-stage arthritis in low-demand patients. | |||
| Nonunion / Malunion | <5% for coronoid; higher for associated radial head or olecranon fractures | Failure of the coronoid fracture to heal, or healing in an unanatomical position leading to instability or impingement. | * Nonunion: Revision ORIF with bone grafting. If chronic and asymptomatic, observation. |
| * Malunion: Corrective osteotomy (if causing impingement or instability) or débridement. If leading to significant arthrosis, consider arthroplasty. | |||
| Nerve Injury | 5-15% (most commonly ulnar nerve) | Ulnar nerve contusion/neuropraxia (iatrogenic or related to initial injury), median nerve injury, radial nerve injury. Can result in sensory deficits, motor weakness, or pain. | * Conservative Management: Observation for neuropraxia (most resolve spontaneously). |
| * Neurolysis / Release: If symptoms persist or worsen, especially for ulnar nerve compression (e.g., within cubital tunnel or due to hardware prominence). Anterior transposition may be performed. | |||
| Infection | 1-5% (superficial or deep) | Surgical site infection. Higher risk in open fractures, prolonged surgery, or immunocompromised patients. | * Superficial: Oral antibiotics, local wound care. |
| * Deep: Surgical irrigation and débridement (I&D), intravenous antibiotics, potential hardware removal (once fracture healed), or staged reconstruction. | |||
| Hardware Related Complications | 5-10% (prominence, breakage) | Screw or plate prominence causing pain, irritation, or impingement; implant breakage. | * Hardware Removal: If symptomatic after fracture healing. |
| * Revision Fixation: If hardware failure leads to loss of reduction and symptomatic nonunion. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgery itself for optimizing functional outcomes and preventing complications such as stiffness or recurrent instability. The protocol is tailored to the stability achieved intraoperatively and the specific fixation performed.
General Principles
- Protection of Fixation: The primary goal in the early phase is to protect the surgical repair while initiating motion.
- Gradual Progression: Rehabilitation progresses through phases, increasing demands on the healing tissues as strength and stability improve.
- Pain Management: Adequate pain control is essential to facilitate patient participation in therapy.
- Patient Education: Patients must understand the importance of adherence to the protocol and activity restrictions.
Phased Rehabilitation Protocol
Phase I: Early Protected Motion (Weeks 0-6)
- Goals: Reduce pain and swelling, protect surgical repair, initiate controlled range of motion (ROM) to prevent stiffness.
-
Immobilization:
- Initially, a posterior splint or hinged elbow brace may be used for comfort and to protect the repair, particularly for the first 1-2 weeks. The brace is typically locked or limited to a safe arc of motion (e.g., 30-90 degrees flexion, no forearm rotation if LCL repaired).
- For highly stable repairs, a sling for comfort may be sufficient, with immediate active/passive ROM as tolerated.
-
Therapeutic Exercises:
- Passive Range of Motion (PROM): Gentle, pain-free flexion and extension, pronation and supination, within the protected arc. Assisted by a therapist or with continuous passive motion (CPM) device if indicated.
- Active-Assisted Range of Motion (AAROM): Patient assists the movement.
- Active Range of Motion (AROM): As pain and stability allow, within the protected arc.
- Shoulder & Hand Exercises: Gentle active ROM for shoulder, wrist, and hand to prevent stiffness in adjacent joints.
-
Restrictions:
- No active lifting or carrying with the affected arm.
- No resisted exercises.
- Avoid sudden or forceful movements.
- Avoid varus/valgus stress, especially if MCL/LCL repaired.
Phase II: Moderate Strengthening & Increased Motion (Weeks 6-12)
- Goals: Gradually increase ROM, initiate gentle strengthening, improve neuromuscular control.
- Brace Weaning: The hinged elbow brace is progressively unlocked to allow greater ROM, and then weaned as stability improves. May be continued for protection during sleep or risky activities.
-
Therapeutic Exercises:
- Full AROM & PROM: Work towards achieving full, pain-free ROM in all planes.
- Gentle Strengthening: Isometrics (e.g., biceps, triceps, forearm flexors/extensors), then progress to light resistance bands or very light weights.
- Eccentric Exercises: May be introduced carefully.
- Joint Mobilization: Therapist-assisted techniques to improve joint play.
-
Restrictions:
- Still avoid heavy lifting, pushing, pulling.
- No impact activities.
Phase III: Advanced Strengthening & Return to Activity (Weeks 12-24+)
- Goals: Maximize strength, power, endurance, and functional capacity; prepare for return to sport or work-specific activities.
- Brace: Typically discontinued, unless specific activities warrant protection.
-
Therapeutic Exercises:
- Progressive Resistance Exercises (PREs): Increase weight and resistance for all muscle groups.
- Functional Exercises: Incorporate activities mimicking daily living, work, or sport.
- Proprioceptive Training: Balance and coordination drills.
- Sport-Specific Training: Gradually introduce sport-specific movements and drills.
-
Return to Activity:
- Gradual return to light duty work or low-impact activities as tolerated.
- Return to heavy manual labor or contact sports is typically cleared after 6 months to 1 year, depending on the complexity of the injury, fracture healing, and restoration of strength and stability.
Throughout all phases, close communication between the surgeon, physical therapist, and patient is essential. Radiographic assessment of fracture healing is typically performed at regular intervals, often at 6 weeks, 3 months, and 6 months post-operatively. Early intervention for any signs of stiffness or instability is critical.
Summary of Key Literature / Guidelines
The understanding and management of coronoid fractures have evolved significantly over recent decades, driven by advancements in imaging, surgical techniques, and biomechanical studies. Key literature provides the foundation for current best practices.
Classification Systems
- Regan-Morrey Classification (1992): The historical cornerstone, categorizing fractures by size (Type I: tip avulsion, Type II: <50% height, Type III: >50% height). While widely used for its simplicity, it lacks specificity regarding the fracture's location and its critical impact on elbow stability.
-
O'Driscoll Classification (2003):
This classification introduced the crucial concept of anteromedial coronoid facet fractures, recognizing their distinct destabilizing role.
- Type 1 (Tip Fractures): Small avulsions.
- Type 2 (Anteromedial Fractures): Fractures involving the sublime tubercle or the entire anteromedial facet, highly correlated with varus posteromedial rotatory instability (VPMRI).
-
Type 3 (Basal Fractures):
Larger fractures involving the entire base, often seen in trans-olecranon fracture-dislocations.
This system provides a more biomechanically relevant framework for surgical decision-making.
Biomechanical Principles
- Ring Concept of the Elbow (Hotchkiss, Morrey): Emphasizes the interconnectedness of bony (ulnohumeral, radiohumeral) and ligamentous (MCL, LCL) structures. Disruption of multiple components leads to instability.
- Coronoid as Primary Stabilizer: Numerous biomechanical studies (e.g., Morrey et al., O'Driscoll et al.) have demonstrated the coronoid's crucial role as an anterior buttress and a site for MCL attachment, vital for resisting posterior translation and valgus stress. Small coronoid fractures, particularly of the anteromedial facet, can lead to gross instability.
- "Terrible Triad" Biomechanics: Studies (e.g., Ring et al.) confirm that the coronoid fracture is the most critical bony component in terrible triad injuries. Its fixation, along with radial head and LCL repair, is paramount for stability.
Surgical Management Consensus
- Indications for ORIF: General consensus supports surgical fixation for displaced coronoid fractures, especially those involving >10-15% of the coronoid height (Regan-Morrey Type II/III), any anteromedial facet fracture (O'Driscoll Type 2), and nearly all coronoid fractures in the context of persistent elbow instability (e.g., terrible triad injuries).
- Approaches: The medial approach is preferred for anteromedial coronoid fractures. Olecranon osteotomy can be considered for extensive exposure in complex cases. Combined medial and lateral approaches are often necessary for terrible triad injuries.
-
Fixation Techniques:
- Suture Lasso/Anchors: Effective for small avulsions or comminuted fragments, especially of the sublime tubercle, promoting ligamentotaxis and MCL stability.
- Lag Screws/Headless Compression Screws: Suitable for larger, reducible fragments, often placed from posterior-to-anterior.
- Plates: Mini-fragment plates or anatomical anteromedial coronoid plates provide robust fixation, especially for larger basal or anteromedial facet fractures. Recent literature supports the use of these plates for their superior stability and buttressing effect.
- Associated Injuries: It is universally agreed that all components of complex elbow instability (radial head, LCL, MCL, coronoid) must be addressed to restore stability and achieve favorable outcomes. Neglecting any one component significantly increases the risk of failure.
Outcomes and Complications
- High-Yield Reviews: Studies by Doornberg et al. and Lindenhovius et al. highlight that while complex elbow injuries have good functional outcomes in a majority of patients after appropriate surgical management, a significant percentage still experiences complications such as stiffness, heterotopic ossification, and post-traumatic arthritis.
- Importance of Rehabilitation: Literature consistently emphasizes the critical role of early, protected range of motion protocols, individualized to the intraoperative stability, in preventing stiffness and promoting functional recovery.
In summary, current guidelines stress the importance of advanced imaging for accurate diagnosis, meticulous pre-operative planning, individualized surgical approaches and robust fixation tailored to the specific fracture pattern and associated injuries, and a dedicated post-operative rehabilitation program. The shift from simply identifying a coronoid fracture to understanding its specific type and biomechanical implications for elbow stability has revolutionized its management, leading to improved functional outcomes for patients with these challenging injuries.
Clinical & Radiographic Imaging

