INTRODUCTION TO CONGENITAL FOREARM ANOMALIES
Congenital anomalies of the forearm, specifically congenital pseudarthrosis of the ulna and congenital radioulnar synostosis, represent profound disruptions in the embryological development and biomechanical integrity of the upper extremity. These conditions challenge the orthopedic surgeon with complex three-dimensional deformities, soft tissue contractures, and unpredictable biological healing potentials. Successful management requires a rigorous understanding of pediatric bone biology, the tethering effects of dysplastic bone, and the compensatory kinematics of the adjacent shoulder and wrist joints.
This comprehensive academic guide delineates the pathoanatomy, clinical evaluation, and step-by-step surgical management of these rare but debilitating conditions, providing evidence-based protocols for orthopedic residents, fellows, and practicing consultants.
CONGENITAL PSEUDARTHROSIS OF THE ULNA
Congenital pseudarthrosis of the ulna is an exceptionally rare clinical entity, frequently—though not exclusively—associated with neurofibromatosis type 1 (NF1). The underlying pathophysiology involves a localized dysplasia of the periosteum and bone, leading to spontaneous fracture and subsequent failure of osteogenesis.
In a landmark review of the English literature, Witoonchart et al. identified 60 patients with congenital forearm pseudarthrosis: 29 presented with ulnar pseudarthrosis, 17 with radial pseudarthrosis, and 14 with pseudarthrosis of both bones. Crucially, of these 60 patients, only 16 (27%) had no clinical signs or family history of neurofibromatosis, underscoring the necessity of a thorough genetic and systemic evaluation in these children.
Pathoanatomy and Biomechanical Consequences
The ulna serves as the stable, non-rotating axis of the forearm around which the radius articulates. When a pseudarthrosis develops in the ulna, this critical stabilizing strut is lost. The biomechanical consequences are predictable and progressive:
* Ulnar Shortening: The dysplastic ulnar segment fails to grow longitudinally.
* Radial Bowing: The intact radius continues to grow but is tethered by the shortened ulna and the interosseous membrane, resulting in significant secondary bowing.
* Radiocapitellar Dislocation: As the radius outgrows the ulna, the proximal migration and bowing force the radial head to dislocate from the capitellum, severely compromising elbow mechanics and stability.
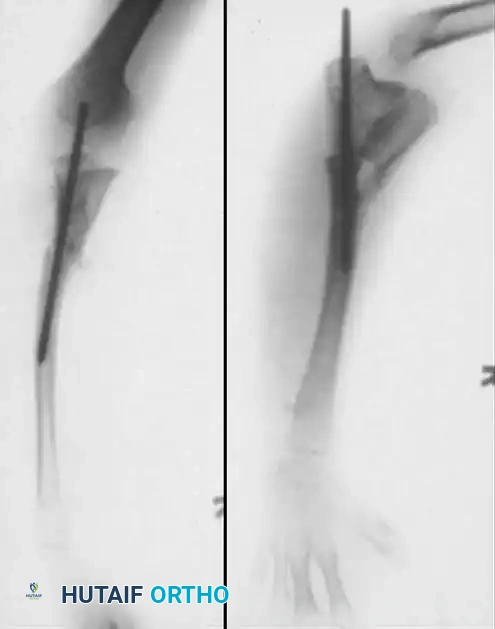
Clinical Radiograph: Preoperative anteroposterior and lateral views demonstrating congenital pseudarthrosis of the ulna with severe radial bowing and secondary dislocation of the radial head.
CLINICAL PEARL:
Early surgical intervention is paramount in congenital ulnar pseudarthrosis. Delaying treatment allows the tethering effect of the pseudarthrosis to cause irreversible plastic deformation of the radius and permanent radiocapitellar dislocation.
Surgical Management Strategies
Various treatment modalities have been described, reflecting the biological recalcitrance of the pseudarthrosis site. Standard nonvascularized bone grafting, with or without internal fixation, has historically yielded high failure rates due to the inherently poor osteogenic potential of the dysplastic periosteum.
1. Early Cystic Lesion Management
If the pseudarthrosis is identified early in its evolution—specifically when it presents as a cystic lesion prior to frank fracture and tapering—aggressive early intervention is warranted.
* Technique: Meticulous curettage of the cyst, robust internal fixation (typically with intramedullary devices), and autogenous cancellous bone grafting. This early intervention carries the highest success rate for preserving native ulnar anatomy.
2. Management of Established Pseudarthrosis
In established cases characterized by atrophic, tapered bone ends and significant radial bowing, the primary goal shifts from achieving ulnar union to preventing further radial deformity.
* Tether Release: The distal ulna should be excised early to relieve its tethering effect on the radius. Following excision, the forearm is supported with a custom-molded orthosis to maintain alignment during growth.
3. Creation of a One-Bone Forearm (Synostosis)
When the radial head has already dislocated and the ulnar defect is insurmountable, the creation of a radioulnar synostosis (a "one-bone forearm") is the salvage procedure of choice. This provides a stable, albeit rotationally fixed, forearm strut.
- Surgical Steps:
- Radial Head Excision: The dislocated, dysplastic radial head is excised to relieve impingement at the elbow.
- Preparation of Synostosis Site: The proximal radius and the distal ulnar stump are decorticated to expose bleeding, healthy cancellous bone.
- Alignment: The forearm is positioned in a functional degree of rotation (typically 10 to 20 degrees of pronation for the dominant arm).
- Internal Fixation: A stout intramedullary nail is passed from the distal radius, across the synostosis site, and into the proximal ulna to provide rigid stabilization.
- Bone Grafting: Autogenous iliac crest bone graft is packed circumferentially around the synostosis site.
Surgical Radiograph: Postoperative view following excision of the radial head, creation of a synostosis between the proximal radius and ulna, and rigid fixation with an intramedullary nail.

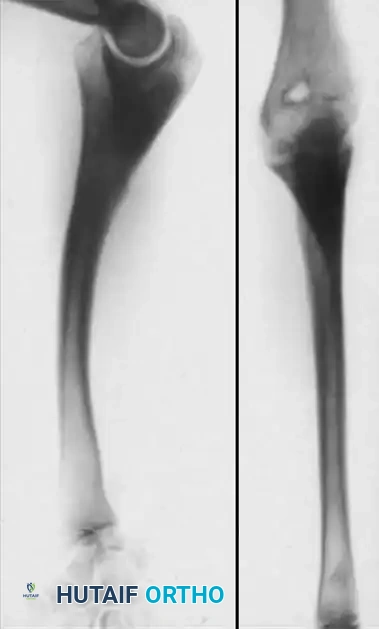
Final Radiograph: Long-term follow-up demonstrating the final appearance and solid consolidation of the one-bone forearm.
4. Advanced Reconstructive Techniques
For patients with small pseudarthrosis "gaps" and acceptable bone quality, the Ilizarov compression-distraction technique has been utilized to achieve union while simultaneously correcting length and angular deformities.
Alternatively, free vascularized fibular grafting represents the pinnacle of biological reconstruction. Bae et al. reported successful outcomes in four children utilizing this technique. Notably, in two very young children (ages 3 and 5), the proximal fibular epiphysis was included in the microvascular transfer. This technically demanding procedure allowed for continued longitudinal growth of the reconstructed ulna, documented at 3 and 6 years postoperatively.
CONGENITAL RADIOULNAR SYNOSTOSIS
Congenital radioulnar synostosis is a failure of longitudinal segmentation between the radius and ulna during the seventh week of gestation. It typically involves the proximal metaphyses of the bones, rigidly fixing the forearm in varying degrees of pronation.
Epidemiologically, the condition is more often bilateral than unilateral. A strong familial predisposition exists, with the deformity frequently transmitted via an autosomal dominant pattern on the paternal side of the family.
The Wilkie Classification System
Wilkie classically categorized congenital radioulnar synostosis into two distinct morphological types, which dictate the complexity of the deformity:
- Type I: The medullary canals of the proximal radius and ulna are seamlessly joined. The proximal radius is malformed and fused to the ulna over a distance of several centimeters. The radius is typically longer and more robust than the ulna, and its diaphysis arches anteriorly more than normal.
- Type II: The radius is morphologically fairly normal, but its proximal end is dislocated (either anteriorly or posteriorly) and fused to the proximal ulnar shaft. The fusion mass is neither as extensive nor as intimately medullary as in Type I. Wilkie noted that Type II is more frequently unilateral and may be associated with other congenital anomalies, such as syndactyly, supernumerary digits, or thumb aplasia.
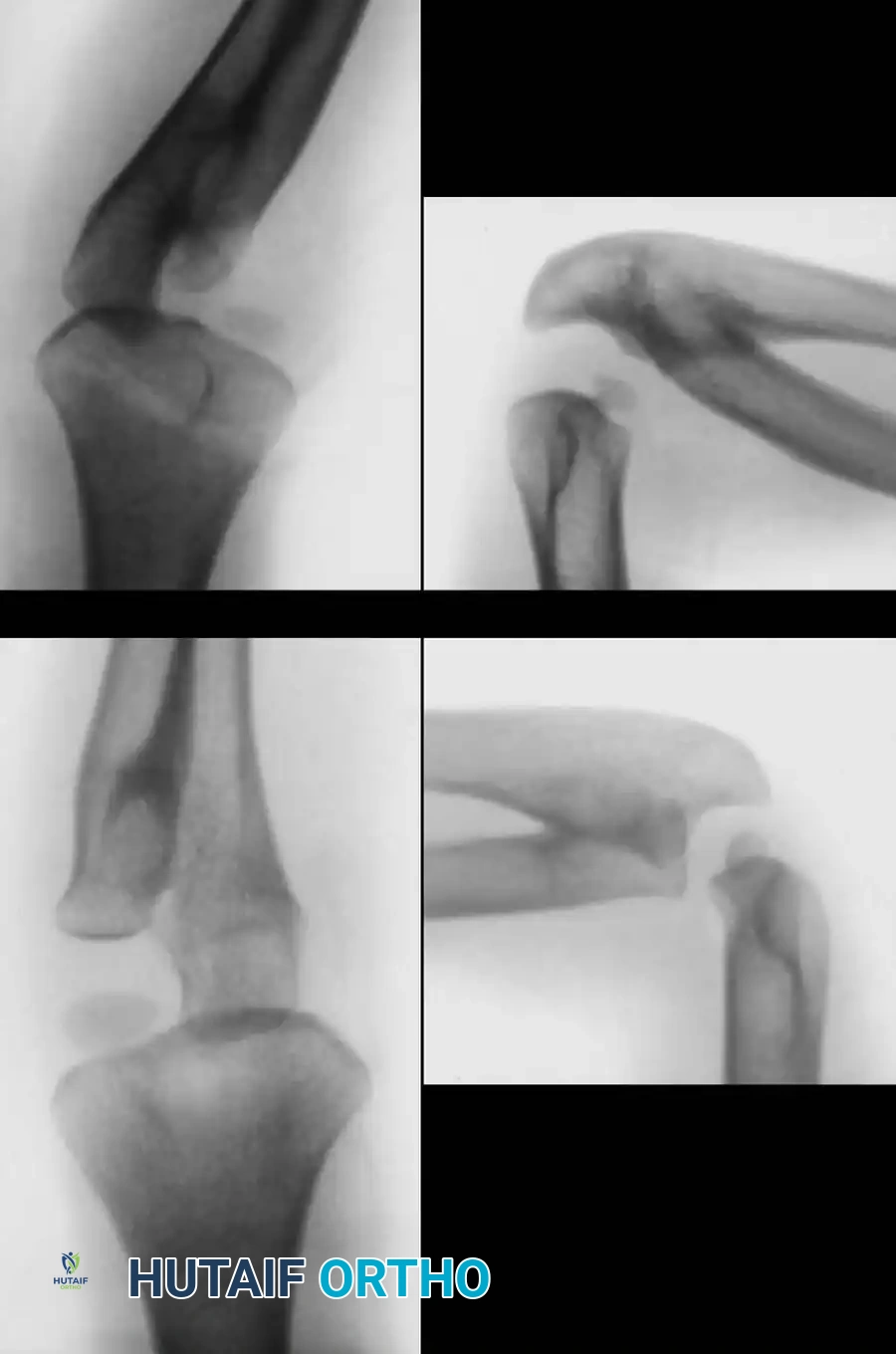
Wilkie Classification of Congenital Radioulnar Synostosis. A and B: Type I, demonstrating proximal fusion for several centimeters with an enlarged, bowed radius. C and D: Type II, demonstrating posterior and lateral dislocation of the proximal radius with a more focal fusion mass.
Clinical Presentation and Compensatory Mechanics
Patients present with an absolute loss of forearm pronation and supination. However, the functional deficit is often masked by profound compensatory kinematics. Children seamlessly utilize glenohumeral rotation, elbow flexion/extension, and radiocarpal hypermobility to position the hand in space.
SURGICAL WARNING:
Simply excising the fused portion of the radius in an attempt to restore rotation universally fails. The surrounding fascial tissues are contracted, the interosseous membrane is narrow and fibrotic, and the supinator musculature is often dysplastic or entirely absent. It is highly inadvisable to perform any operation with the primary hope of obtaining active pronation and supination.
Indications for Surgical Intervention
Because compensatory shoulder motion (especially with the elbow extended) is highly effective, most patients are not disabled enough to justify extensive surgical intervention. Surgery is strictly indicated for:
1. Severe, disabling pronation or supination deformities that prevent activities of daily living (e.g., bringing food to the mouth, perineal hygiene).
2. Bilateral hyperpronation, where the patient cannot compensate effectively with either limb.
The goal of surgery is not to restore motion, but to reposition the fixed forearm into a more functional arc. Generally, the dominant extremity is positioned in 10 to 20 degrees of pronation (for writing and keyboard use), while the nondominant extremity is placed in neutral to 20 degrees of supination (to assist in holding objects and hygiene).
Surgical Techniques for Derotational Osteotomy
Derotational osteotomies can be performed at the synostosis site, the diaphyseal level, or the distal metaphysis.
The Two-Stage Percutaneous Drill-Assisted Osteotomy (Lin et al.)
Lin et al. described a highly effective, minimally invasive two-stage technique for correcting severe forearm rotational deformities. This approach minimizes the risk of neurovascular compromise and compartment syndrome, which are significant risks in acute, single-stage derotations.
Preoperative Preparation:
* Ensure the patient is positioned supine with a radiolucent hand table.
* Fluoroscopy must be available to confirm osteotomy sites.
* A sterile tourniquet is applied to the proximal arm.
Stage 1: Percutaneous Osteoclasis
1. Radial Approach: Under tourniquet control, make a 1- to 2-cm longitudinal incision over the dorsolateral ridge of the distal third of the radius.
2. Subperiosteal Exposure: Carefully elevate the periosteum to protect the superficial branch of the radial nerve and extensor tendons.
3. Drill-Assisted Weakening: Mark the osteotomy site with several fine drill holes (e.g., 1.5 mm or 2.0 mm drill bit) penetrating both the near and far cortices in a linear fashion.
4. Ulnar Approach: Make a second small incision over the subcutaneous border of the proximal third of the ulna. Similarly expose the bone subperiosteally and drill the cortex.
5. Osteotomy Completion: Use a sharp, narrow osteotome to carefully complete the division of the radius, followed by the ulna.
6. CRITICAL STEP: Make no attempt at this point to change the rotational position of the arm. Acute correction at this stage risks severe neurovascular traction injuries.
7. Closure: Deflate the tourniquet, obtain meticulous hemostasis, irrigate, and close the wounds with subcuticular sutures. Apply a well-padded, long-arm cast over sterile dressings in the in situ deformity position.
Stage 2: Manipulation and Casting (10 Days Post-Op)
1. Anesthesia: Ten days later, return the patient to the operating room. Remove the cast under general anesthesia.
2. Manipulation: Gently manipulate the forearm, supinating or pronating the callus-forming osteotomy sites into the pre-planned functional position. The early callus acts as a biological hinge, providing stability while allowing plastic deformation.
3. Radiographic Confirmation: Obtain anteroposterior and lateral fluoroscopic views to confirm acceptable bony apposition and alignment.
4. Neurovascular Check: Carefully check distal pulses and capillary refill after manipulation. Monitor the extremity closely in the recovery room to detect any signs of delayed compartment syndrome.
5. Immobilization: Apply a new, well-molded long-arm cast. This is worn for an additional 6 to 8 weeks to allow for complete bony consolidation.
Outcomes and Complications of Osteotomy
Lin et al. reported functional improvement in 25 of 26 forearms treated with this method, including all 12 forearms with congenital radioulnar synostosis. While the total arc of motion remains unchanged, shifting the arc into a functional zone dramatically improves patient independence.
However, surgeons must be vigilant regarding nonunion. Dalton et al. evaluated 69 extremities treated with this method and noted delayed union or nonunion in 21 (30%) of the ulnar osteotomies.
* Risk Factors for Nonunion: Increased patient age, the use of percutaneous techniques (which may cause thermal necrosis if drilling is not irrigated), and placing the osteotomy site in the dense cortical bone of the proximal ulna.
* Note: Patients with congenital radioulnar synostosis actually demonstrated a significantly higher union rate compared to those undergoing the procedure for brachial plexus palsy contractures.
Advanced Mobilization Techniques
While traditional teaching dictates that restoring motion is impossible, Kanaya and Ibaraki described a novel technique utilizing a free vascularized fascia-fat graft to prevent recurrent ankylosis after synostosis takedown.
* The graft is harvested from the lateral aspect of the ipsilateral arm, minimizing donor site morbidity.
* The authors found that combining the synostosis excision with a radial osteotomy prevented postoperative dislocation of the radial head and significantly increased the arc of motion (averaging 83 degrees of motion with osteotomy versus 40 degrees without).
* While promising, this represents a highly specialized microsurgical intervention and is generally reserved for centers with extensive pediatric hand and microvascular expertise.
CONCLUSION
The management of congenital pseudarthrosis of the ulna and radioulnar synostosis requires a masterful understanding of pediatric forearm biomechanics. Whether executing a complex one-bone forearm reconstruction to salvage a tethered radiocapitellar joint, or performing a staged percutaneous osteoclasis to reposition a synostotic limb, the orthopedic surgeon must prioritize functional utility over anatomical perfection. Strict adherence to evidence-based indications, meticulous surgical technique, and respect for the compromised biology of these anomalies are the cornerstones of successful patient outcomes.
📚 Medical References
- Bauer M, Jonsson K: Congenital radioulnar synostosis: radiological characteristics and hand function—case reports, Scand J Plast Reconstr Surg Hand Surg 22:251, 1988.
- Dal Monte A, Andrisano A, Bungaro P, et al: Congenital proximal radio-ulnar synostosis: clinical and anatomical features, Ital J Orthop Traumatol 13:201, 1987.
- Dal Monte A, Andrisano A, Mignani G, et al: A critical review of the surgical treatment of congenital proximal radio-ulnar synostosis, Ital J Orthop Traumatol 13:181, 1987.
- Dalton JF 4th, Manske PR, Walter JC, et al: Ulnar nounion after osteoclasis for rotational deformities of the forearm, J Hand Surg 31A:973, 2006.
- Fujimoto M, Kato H, Minami A: Rotational osteotomy at the diaphysis of the radius in the treatment of congenital radioulnar synostosis, J Pediatr Orthop 25:676, 2005.
- Griffet J, Berard J, Michel CR, et al: Les synostoses congenitales radio-cubitales superieures: a propos de 43 cas, Int Orthop 10:265, 1986.
- Hankin FM, Smith PA, Kling TF Jr, et al:
