Congenital and Developmental Anomalies of the Hip and Pelvis
Congenital and developmental dysplasia of the hip (DDH) represents a complex spectrum of anatomical abnormalities ranging from mild capsular laxity and acetabular dysplasia to frank, irreducible dislocation of the femoral head from the true acetabulum. The management of DDH requires a profound understanding of pediatric hip biomechanics, meticulous clinical examination, and age-specific surgical algorithms.
In a newborn with true congenital dislocation of the hip, the femoral head can often be dislocated and reduced into and out of the true acetabulum. However, if left untreated, the femoral head remains dislocated in the older child, leading to irreversible secondary adaptive changes in both the femoral head and the acetabulum.
Epidemiology and Pathogenesis
Historically, the incidence of congenital dysplasia of the hip has been estimated to be approximately 1 in 1,000 live births. However, modern screening has refined these numbers. Lehmann et al., in a comprehensive meta-analysis, estimated the incidence of DDH revealed by physical examination done by pediatricians to be 8.6 per 1,000; for orthopaedic screening, 11.5 per 1,000; and for ultrasound examination, 25 per 1,000.
Bialik et al. reported that ultrasound screening of 18,060 hips detected 1,001 that deviated from normal (an incidence of 55.1 per 1,000). Crucially, only 90 hips remained abnormal at repeat examinations at 2 and 6 weeks, yielding a true DDH incidence of 5 per 1,000. None of the other hips with transient "sonographic DDH" developed true DDH during a 12-month follow-up, highlighting the importance of distinguishing between physiological neonatal laxity and true dysplasia.
Clinical Pearl: The left hip is more commonly involved than the right, and bilateral involvement is more common than involvement of the right hip alone. This is largely attributed to the common intrauterine position (left occiput anterior), which forces the left hip into adduction against the maternal lumbosacral spine.
Risk Factors and Etiology
Several risk factors must arouse immediate suspicion of DDH:
* Sex: The disorder is significantly more common in girls than in boys (odds ratio 4:1).
* Breech Presentation: Breech deliveries constitute 3% to 4% of all deliveries, but the incidence of DDH is exponentially increased in this population (odds ratio 5:5). MacEwen and Ramsey found that the combination of female sex and breech presentation results in DDH in 1 out of 35 such births.
* Genetics: A positive family history increases the likelihood of DDH to approximately 10% (odds ratio 1:7). Ortolani reported a 70% incidence of a positive family history in his cohorts. Wynne-Davies described a familial occurrence of a "shallow" acetabulum, defined as a "dysplasia trait."
* Mechanical Factors: Postnatal mechanical forces play a critical role. Cultures that place infants in swaddling clothes with the hips in constant extension and adduction exhibit a high incidence of DDH (e.g., Navajo Indians), whereas cultures carrying infants in a flexed/abducted position (e.g., Chinese) have a relatively low incidence.
* Associated Conditions: A strong association exists between DDH and other "packaging" disorders. Carney and Vanek found DDH in 16% of children requiring surgery for clubfoot. Tien et al. found a 17% coexistence rate of congenital muscular torticollis and DDH.
Diagnosis and Clinical Presentation
The clinical presentation of DDH is highly age-dependent. A dynamic, evolving approach to physical examination is mandatory.
The Newborn (Birth to 6 Months)
In newborns, radiographs are notoriously unreliable due to the unossified cartilaginous nature of the femoral head and acetabulum. Diagnosis relies heavily on dynamic clinical testing and ultrasonography.
Routine clinical screening must include the Ortolani test and the provocative maneuver of Barlow.
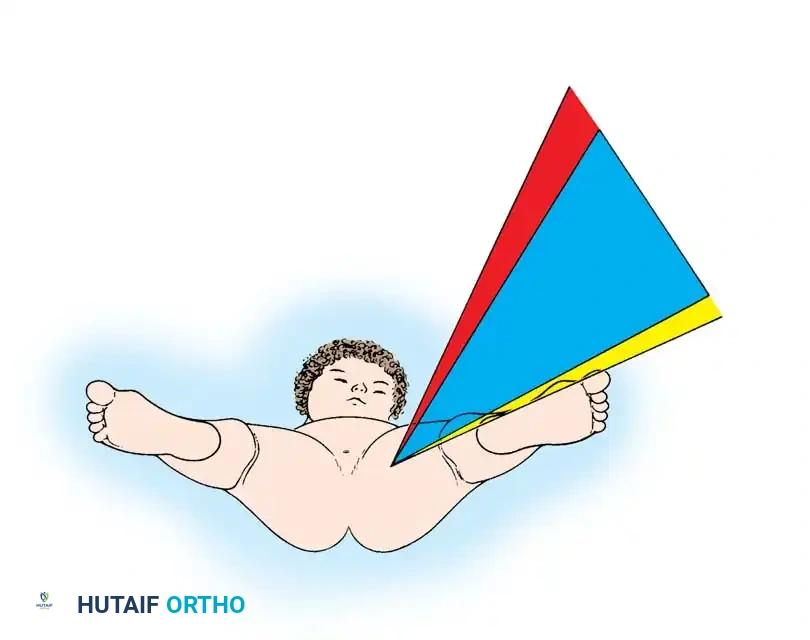
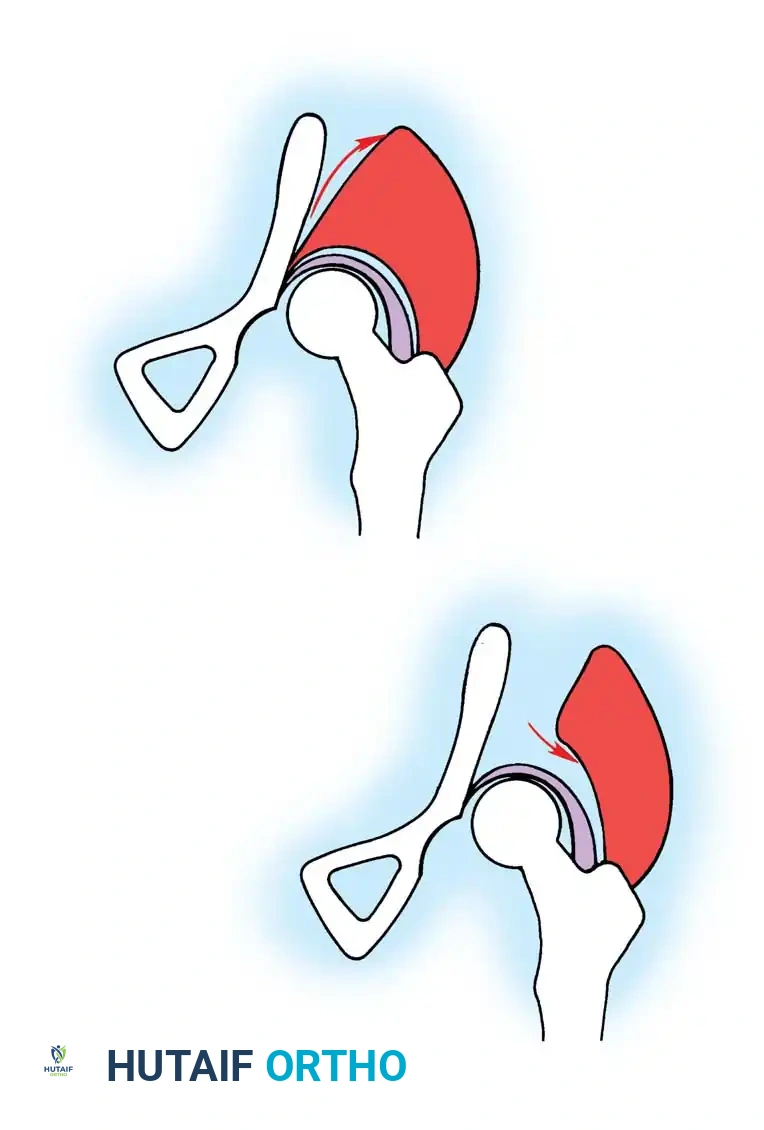
* Ortolani Maneuver: Performed by gently abducting and elevating the flexed hip to detect the reduction of a dislocated femoral head into the true acetabulum. A palpable "clunk" indicates a positive test.
* Barlow Maneuver: Detects potential subluxation or posterior dislocation by applying direct posterior pressure on the longitudinal axis of the femur while the hip is in adduction.

Fig 27-1: Ortolani maneuver for routine screening. The examiner stabilizes the pelvis, places the index and middle fingers over the greater trochanter, and gently abducts the hip.
Surgical Warning: Both tests require a relaxed, pacified child. Forceful maneuvers must be strictly avoided, as they can damage the delicate infantile articular cartilage or cause iatrogenic instability.
The Infant (6 to 18 Months)
As the child ages, capsular laxity decreases, and soft-tissue contractures develop. The Ortolani and Barlow signs disappear, replaced by secondary signs of dislocation:
1. Limitation of Abduction: The most reliable clinical sign in this age group, caused by contracture of the adductor longus.
2. Galeazzi Sign: Apparent shortening of the femur on the affected side due to proximal and lateral displacement of the femoral head.
3. Asymmetrical Skin Folds: While commonly cited, this is less specific. However, Ando and Gotoh found that abnormally long or deep inguinal folds are strong indicators for further evaluation.
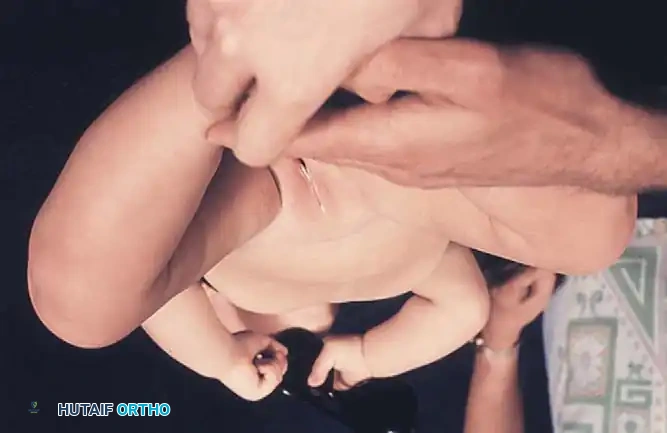

Fig 27-2: Clinical signs of DDH in an older infant. Note the profound decrease in abduction (A) and the positive Galeazzi sign (B).
Imaging Modalities
Ultrasonography: The gold standard for infants under 6 months. Graf's ultrasonographic classification evaluates the alpha angle (bony roof) and beta angle (cartilaginous roof). While highly sensitive, it is observer-dependent.
Radiography: Becomes reliable after 4 to 6 months as the ossific nucleus of the femoral head appears. Key radiographic parameters include:
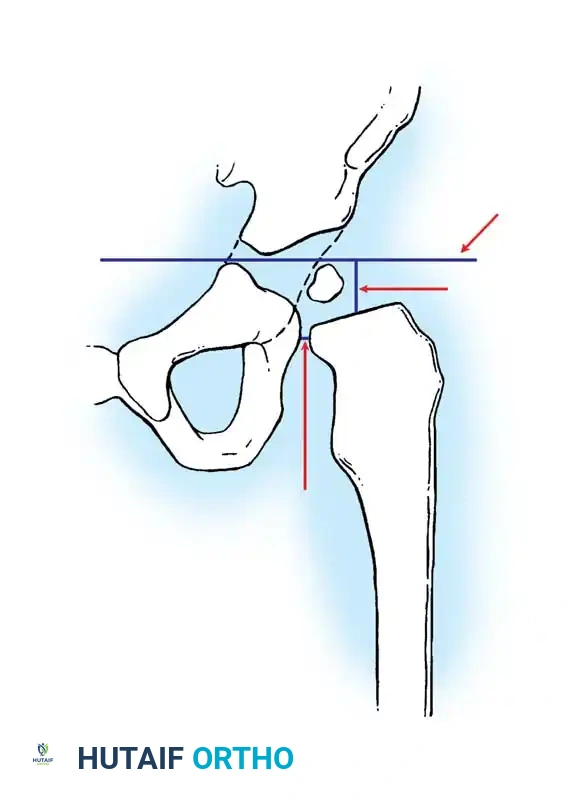
* Hilgenreiner's Line: A horizontal line through the triradiate cartilages.
* Perkins' Line: A vertical line dropped from the lateral margin of the acetabulum, perpendicular to Hilgenreiner's line.
* Shenton's Line: A continuous arc drawn from the medial border of the femoral neck to the superior border of the obturator foramen. Disruption indicates proximal migration.
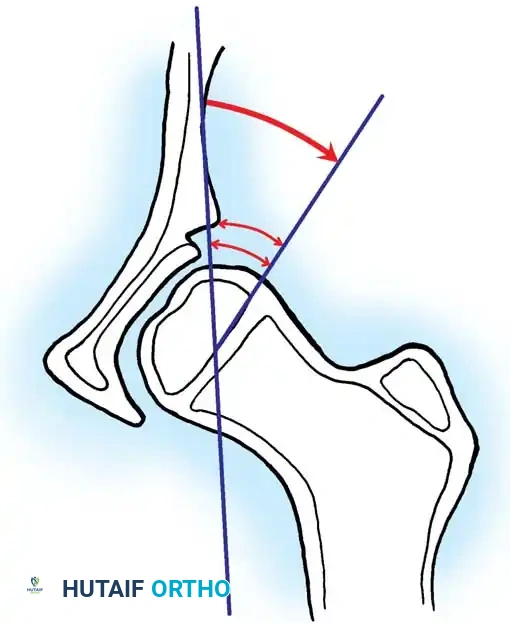
* Acetabular Index: The angle between Hilgenreiner's line and a line drawn from the triradiate cartilage to the lateral edge of the acetabulum. Normal is <30 degrees in newborns; >35 degrees is highly suspicious for dysplasia.

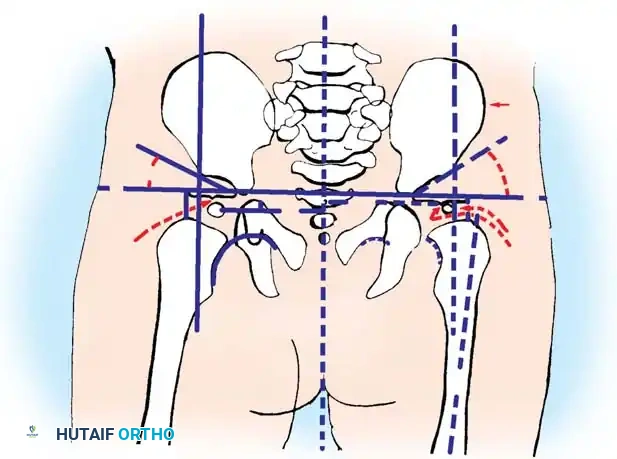
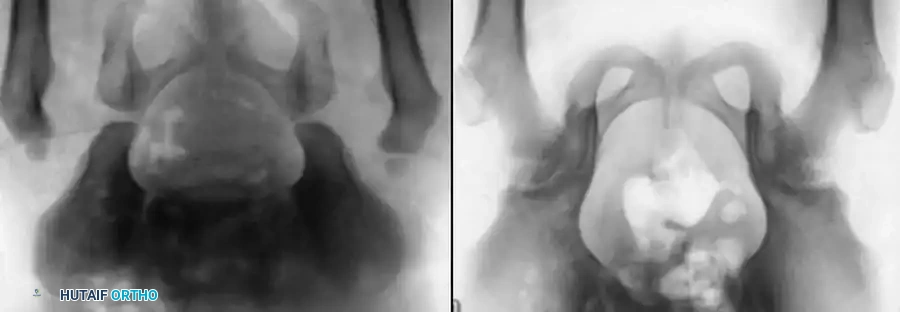
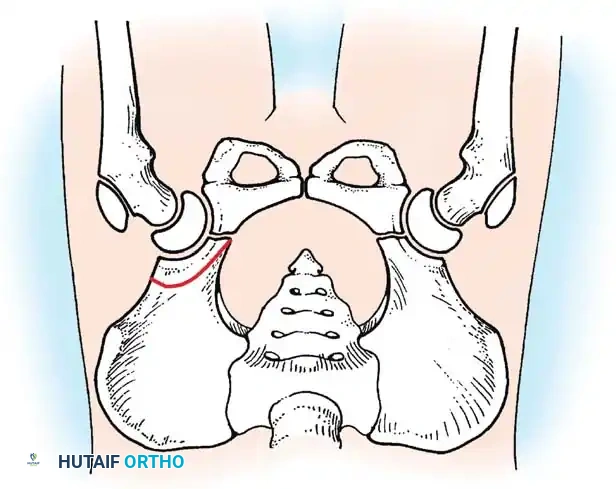
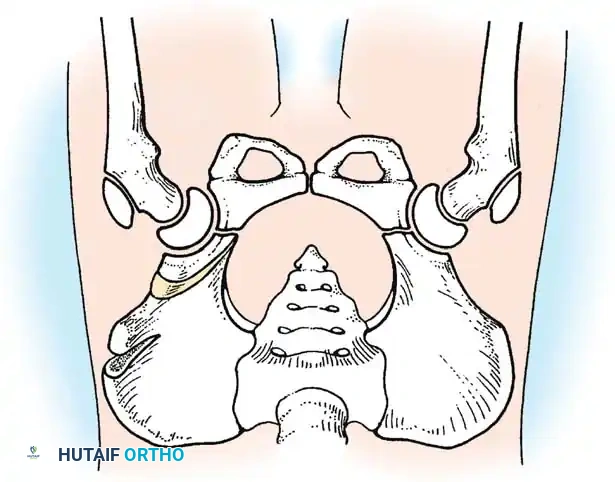
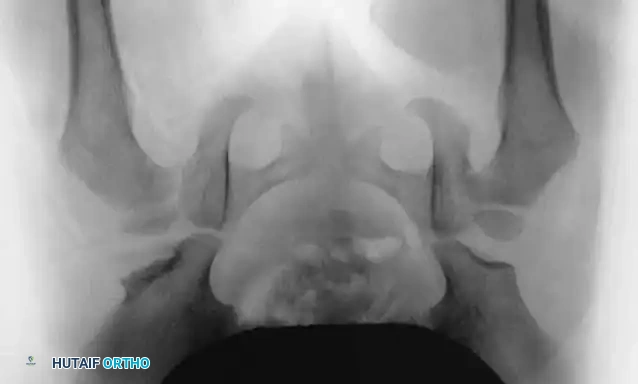
Radiographic evaluation: Normal hip anatomy (left) versus Dysplastic hip anatomy (right) demonstrating disruption of Shenton's line and an increased acetabular index.
Treatment Algorithms by Age Group
The treatment of DDH is strictly age-related, tailored to the specific pathological anatomy, and aims to achieve and maintain a concentric reduction to stimulate normal acetabular development.
Newborn (Birth to 6 Months): Dynamic Orthosis
Treatment is directed at stabilizing the reducible hip (positive Ortolani) or reducing the subluxated hip. The Pavlik Harness is the gold standard.
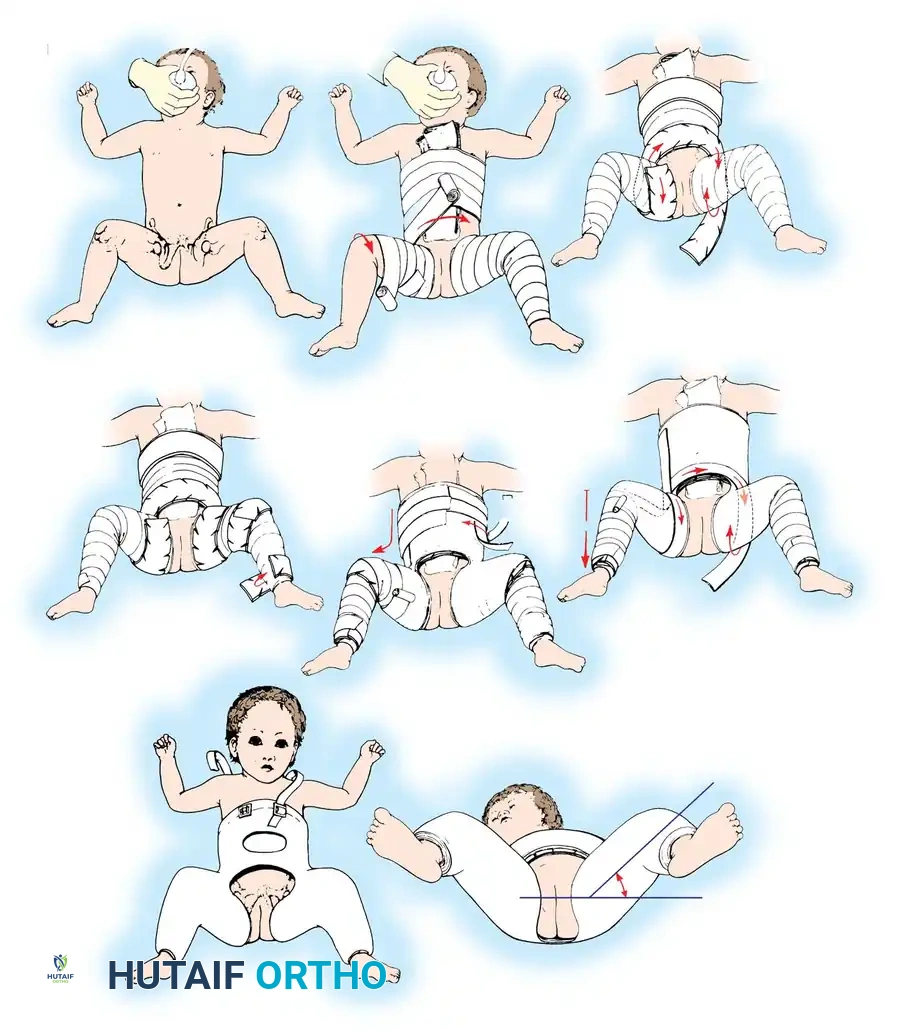
Biomechanics of the Pavlik Harness:
The harness functions as a dynamic flexion-abduction orthosis.
* Anterior straps are adjusted to maintain hip flexion at 100 to 110 degrees. This redirects the femoral head toward the triradiate cartilage.
* Posterior straps prevent adduction but must not force abduction. Forced abduction is the primary cause of iatrogenic avascular necrosis (AVN).
Efficacy and Complications:
A success rate of 85% to 95% is reported. Grill et al., in a multicenter European Paediatric Orthopaedic Society study of 3,611 hips, reported a 95% reduction rate in dysplastic hips. Cashman et al. found osteonecrosis in only 1% of hips treated with the harness.
Pitfall: The Pavlik harness is contraindicated in teratologic dislocations (e.g., arthrogryposis, spina bifida) and in infants with severe soft-tissue contractures. Failure to achieve reduction within 3 to 4 weeks is an indication to abandon the harness to prevent "Pavlik harness disease" (posterior acetabular wear).

Infant (6 to 18 Months): Closed Reduction and Spica Casting
As soft-tissue contractures develop, the Pavlik harness loses efficacy. The treatment of choice shifts to closed reduction under general anesthesia, often preceded by an arthrogram and adductor tenotomy.
Surgical Steps for Closed Reduction:
1. Examination under Anesthesia (EUA): Assess the "safe zone of Ramsey"—the arc between maximum abduction and the point of dislocation in adduction. A safe zone of at least 20 degrees is required.
2. Percutaneous Adductor Tenotomy: If the safe zone is narrow or abduction is <60 degrees, a percutaneous release of the adductor longus is performed to widen the safe zone and decompress the joint, drastically reducing the risk of AVN.
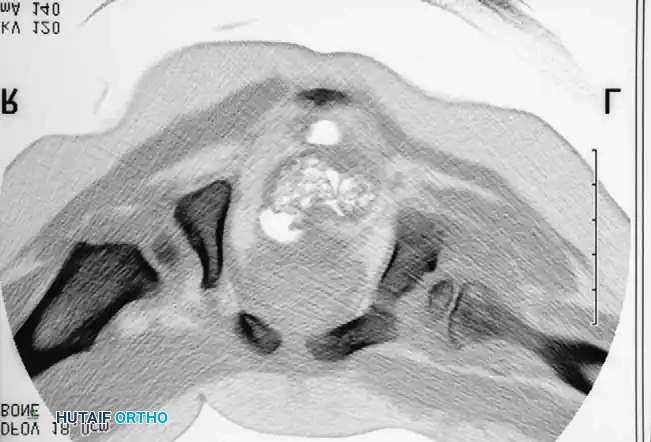
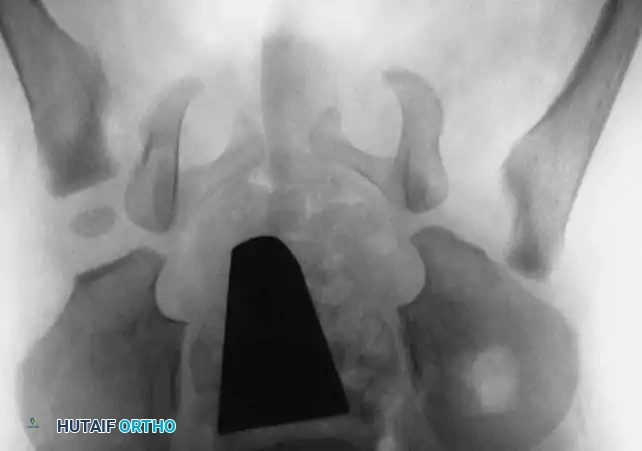
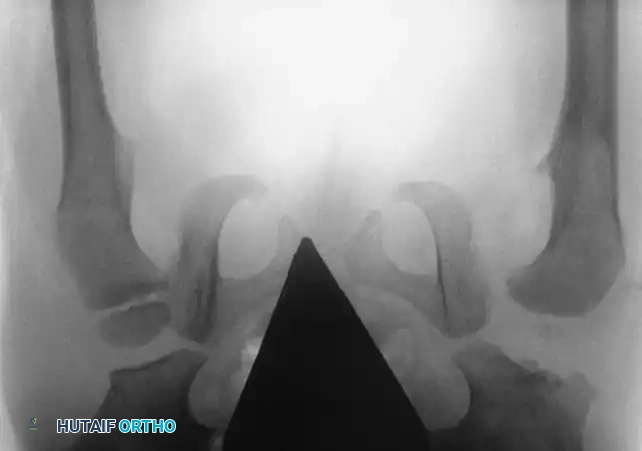
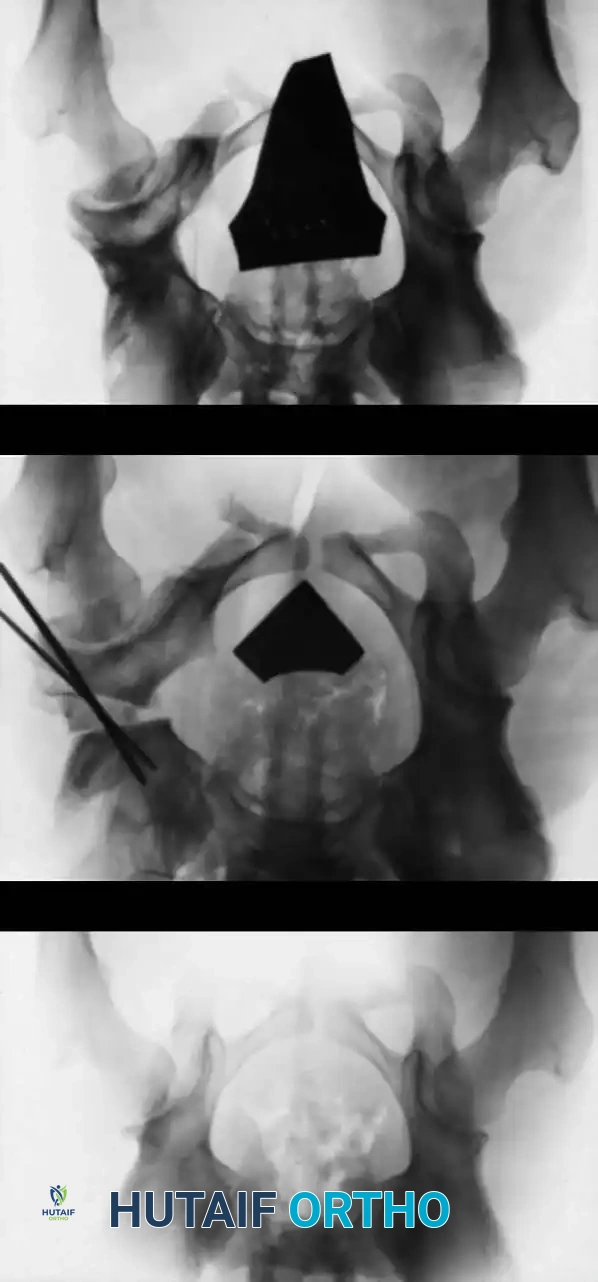
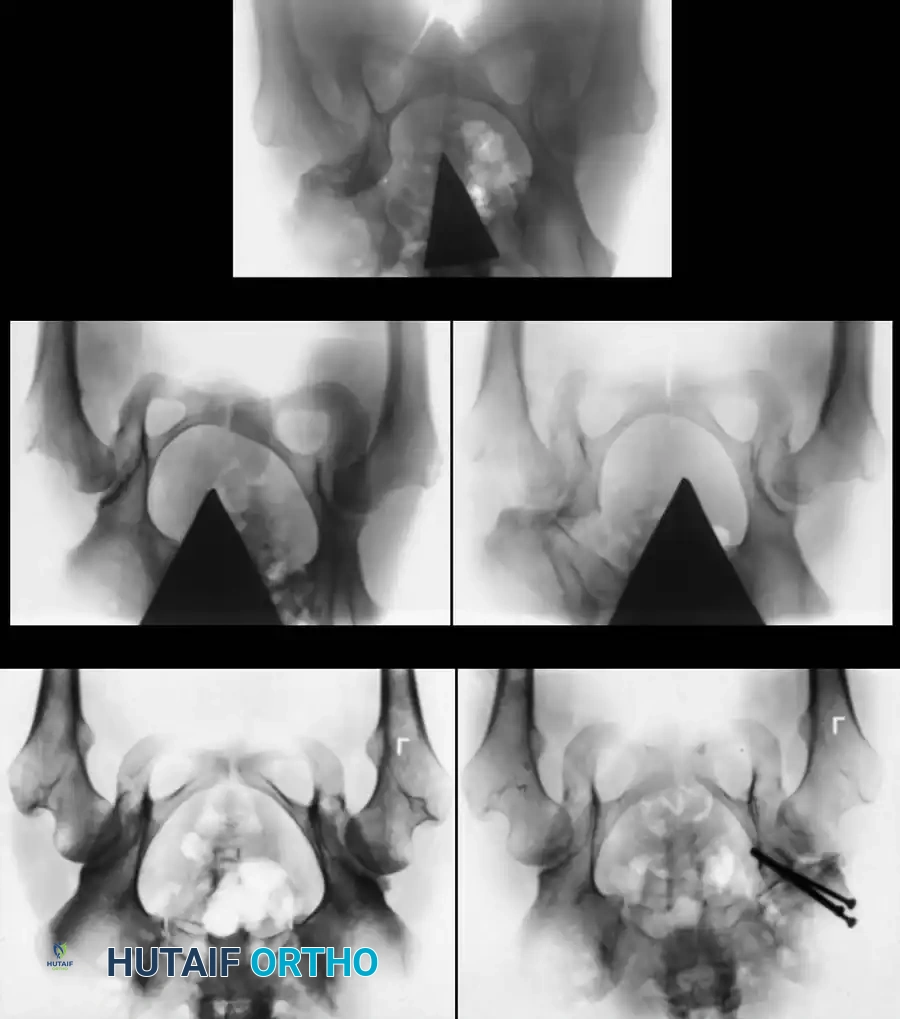
3. Arthrogram: Dye is injected to visualize the cartilaginous profile. Look for the "rose thorn" sign (limbus), the transverse acetabular ligament, and the ligamentum teres. Pooling of dye medially indicates an interposed pulvinar or inverted limbus preventing concentric reduction.
4. Spica Casting: The hip is immobilized in the "human position"—90 to 100 degrees of flexion and 40 to 50 degrees of abduction. Extreme "frog-leg" positions must be avoided to prevent vascular compromise to the femoral head.

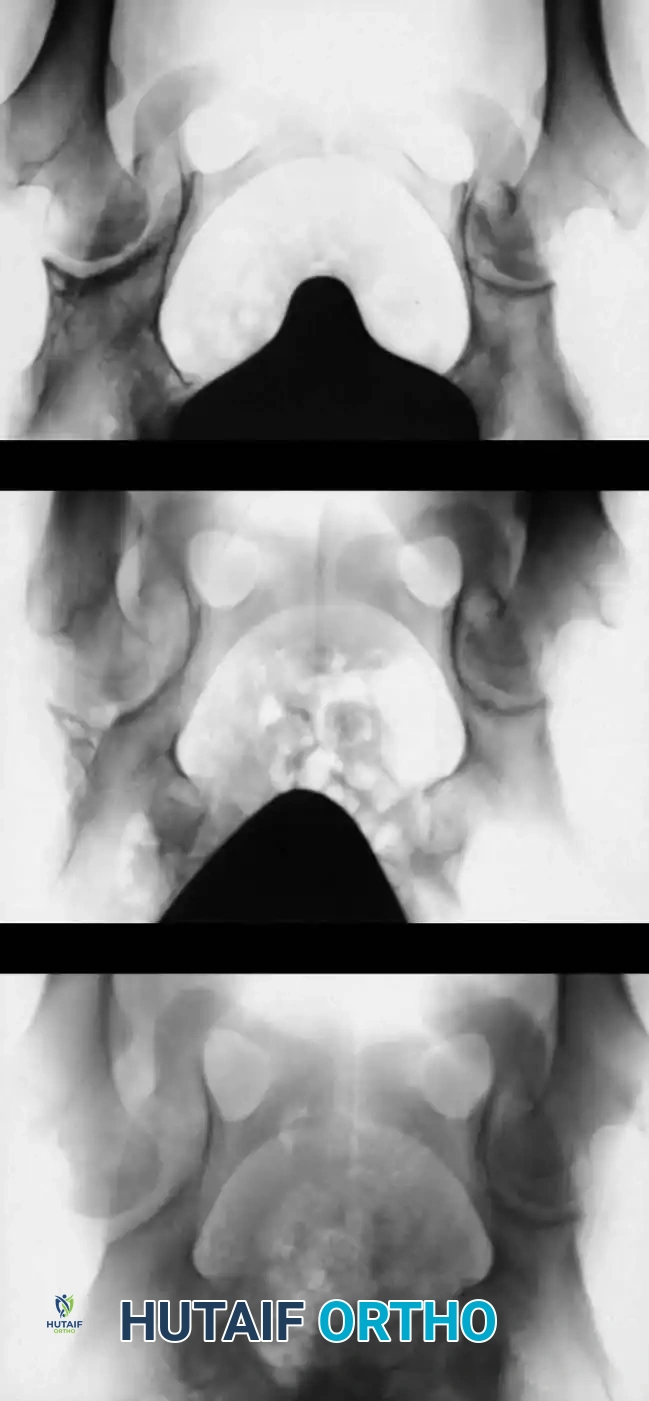
Intraoperative arthrogram demonstrating the cartilaginous contours of the femoral head and acetabulum during closed reduction.
Toddler (18 to 36 Months): Open Reduction
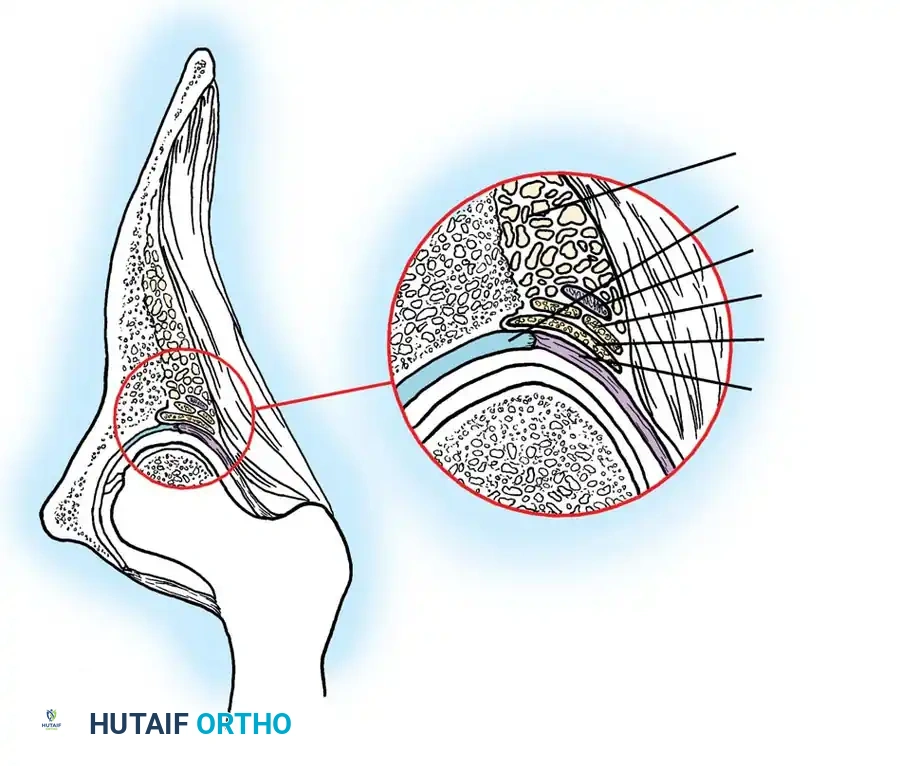
If closed reduction fails, or if the child presents late with severe contractures and anatomical blocks to reduction, open reduction is mandated. The blocks to reduction typically include:
* Constricted capsule (hourglass deformity)
* Hypertrophied ligamentum teres
* Inverted acetabular labrum (limbus)
* Contracted transverse acetabular ligament
* Fibrofatty pulvinar filling the acetabulum
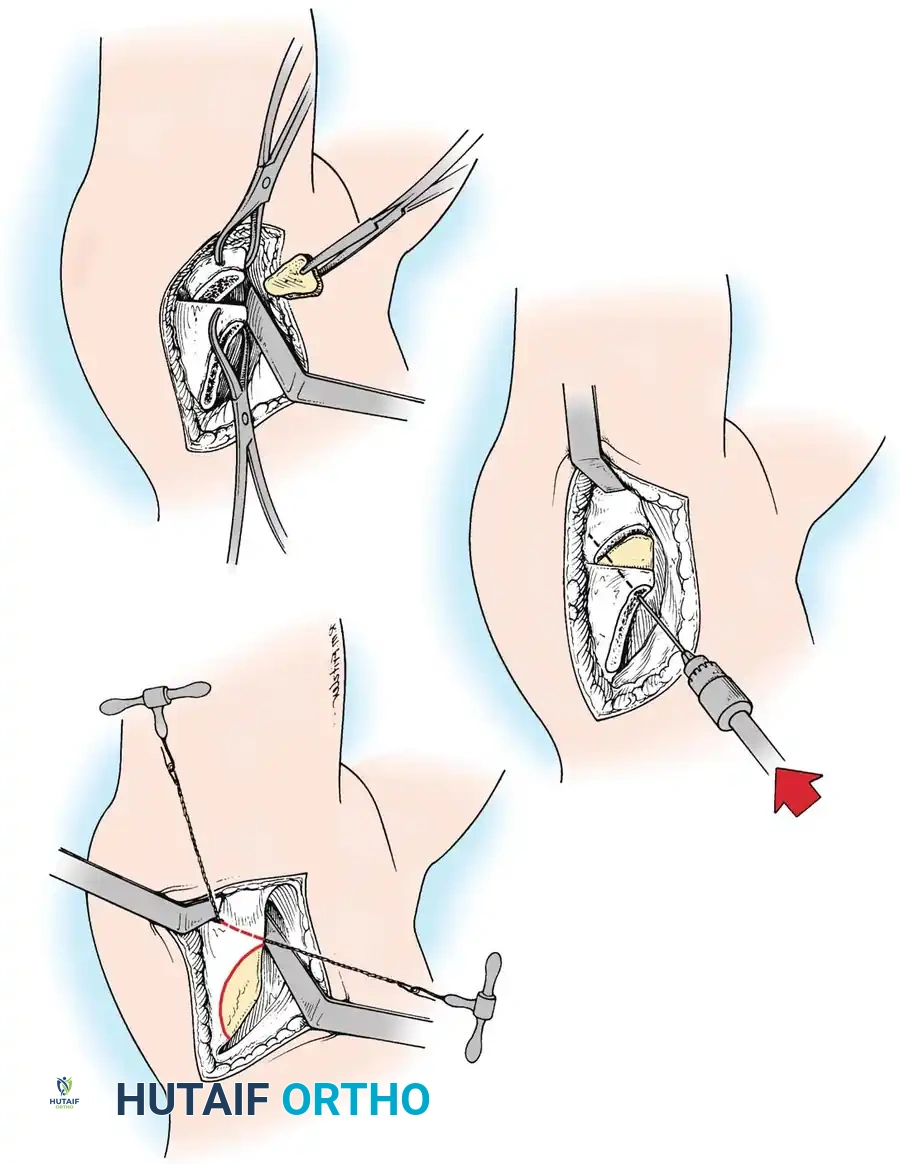
Anterior Approach (Smith-Petersen):
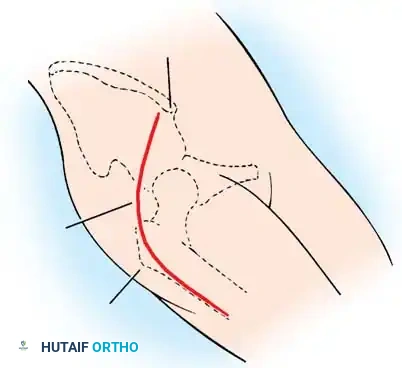
1. Incision: "Bikini" incision below the iliac crest.
2. Interval: Develop the plane between the tensor fasciae latae (superior gluteal nerve) and the sartorius (femoral nerve).
3. Deep Dissection: Detach the rectus femoris from the AIIS. Isolate and release the iliopsoas tendon at the pelvic brim to relieve the hourglass constriction of the capsule.
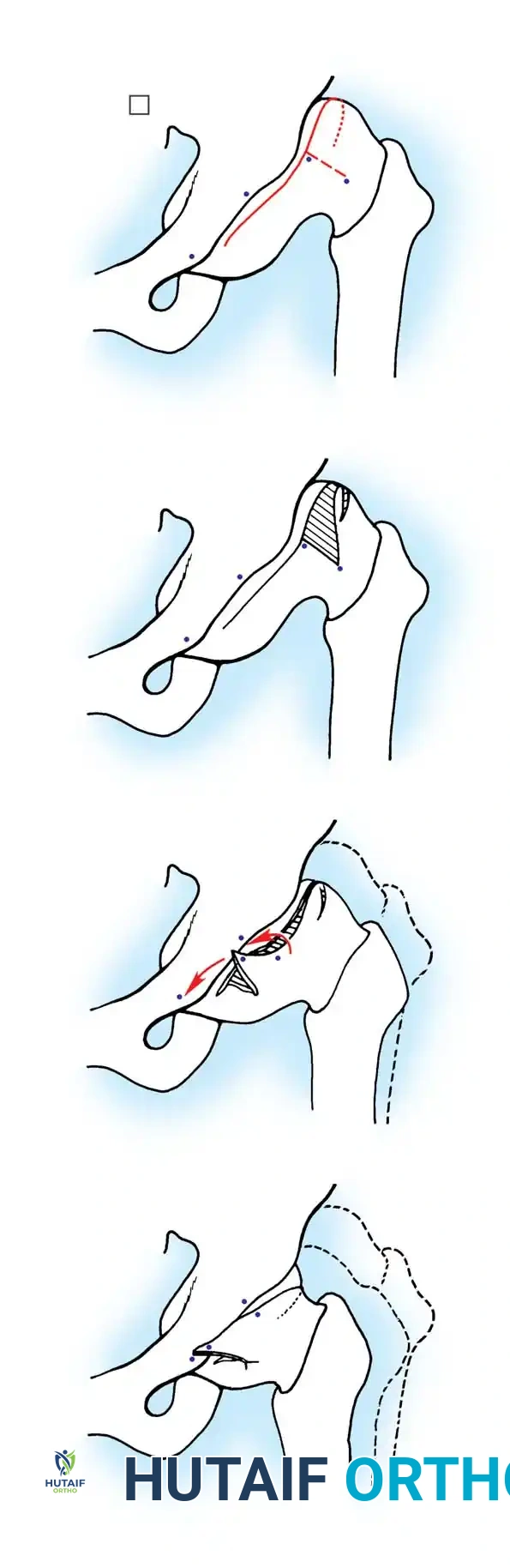
4. Capsulotomy: A T-shaped or I-shaped capsulotomy is performed parallel to the acetabular margin.
5. Joint Clearance: Excise the ligamentum teres, clear the pulvinar, and incise the transverse acetabular ligament inferiorly. Never excise the limbus, as it is critical for future acetabular growth; radial incisions may be made if it is severely inverted.
6. Capsulorrhaphy: Following concentric reduction, the redundant capsule is advanced superiorly and laterally to stabilize the joint.

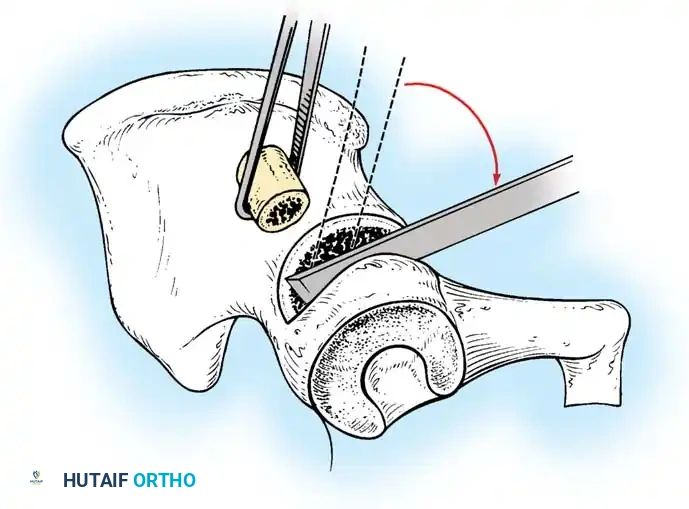
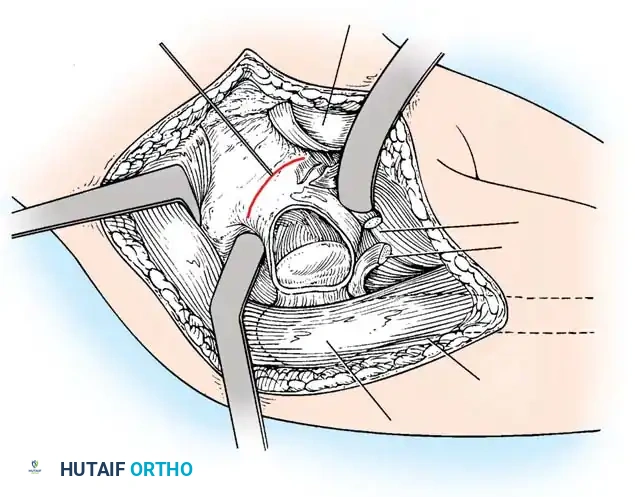
Intraoperative view of the anterior approach to the hip, demonstrating capsulotomy and exposure of the dysplastic joint.
Child (3 to 8 Years): Pelvic and Femoral Osteotomies
In older children, the remodeling potential of the acetabulum diminishes rapidly. Open reduction alone is insufficient; it must be combined with bony procedures to provide mechanical stability and stimulate remodeling.
Femoral Shortening Osteotomy:
In high dislocations, pulling the femur down to the acetabulum creates massive compressive forces, leading to AVN. A subtrochanteric shortening and derotation osteotomy decompresses the joint, allowing reduction without tension.
Pelvic Osteotomies:
Pelvic osteotomies are broadly categorized into redirectional (e.g., Salter, Triple) and reshaping/volume-reducing (e.g., Pemberton, Dega).
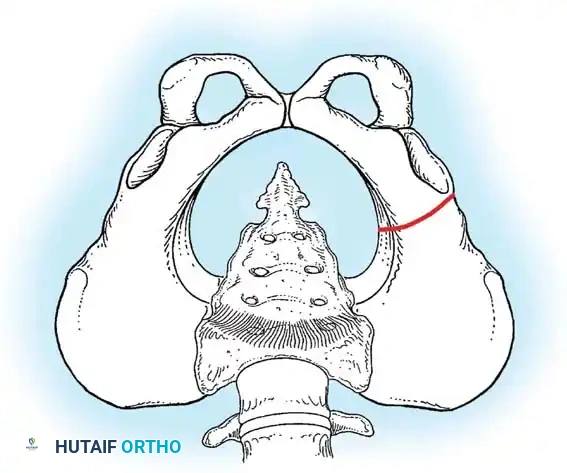
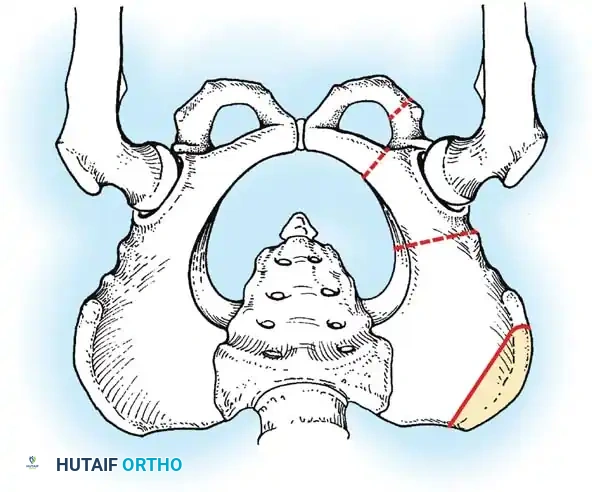
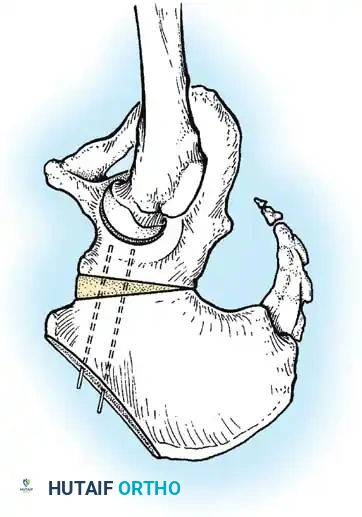
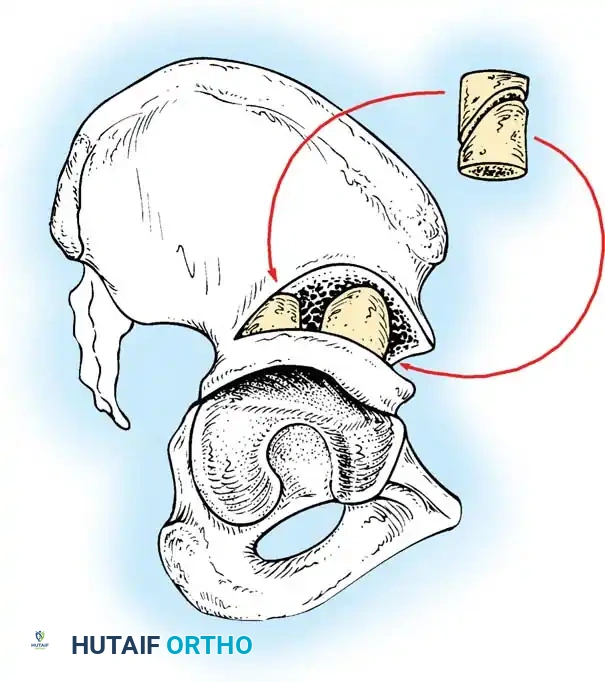
- Salter Innominate Osteotomy:
- Indications: Children aged 18 months to 6 years with a congruous joint but anterolateral acetabular deficiency.
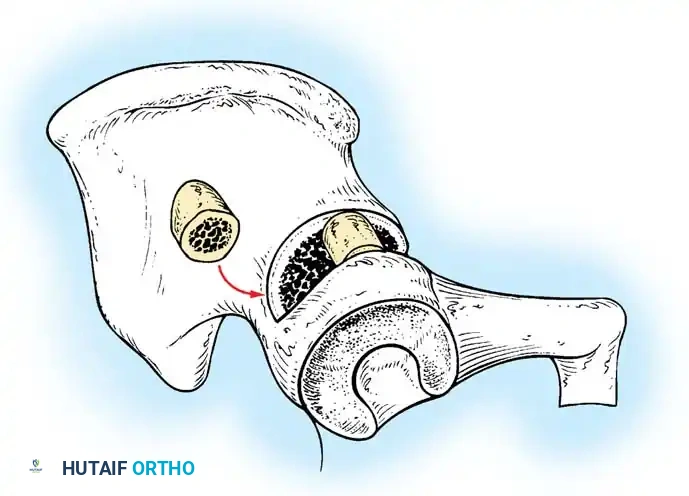
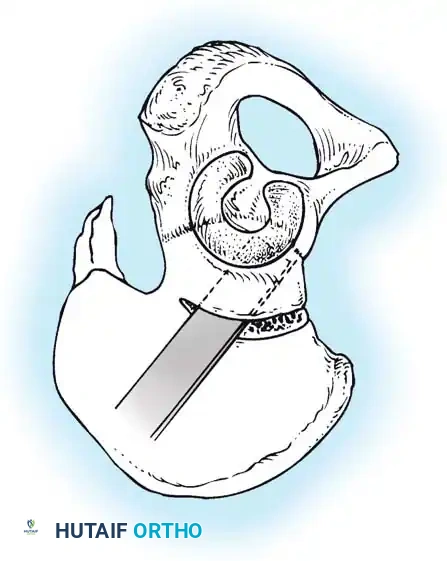
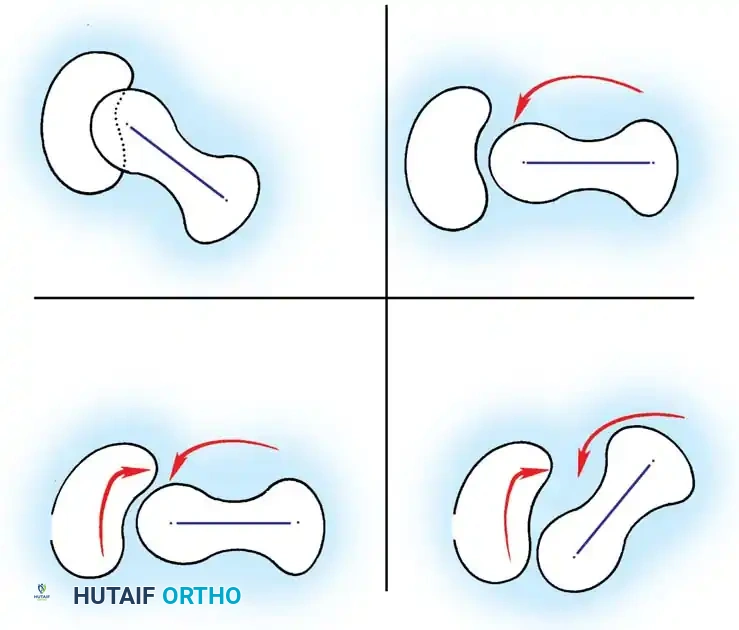
- Biomechanics: A complete transverse cut is made through the ilium just above the acetabulum to the sciatic notch. The entire acetabulum is rotated anteriorly and laterally, hinging on the pubic symphysis.
- Fixation: A triangular bone graft (harvested from the iliac crest) is placed in the osteotomy site, and the construct is stabilized with threaded Kirschner wires.
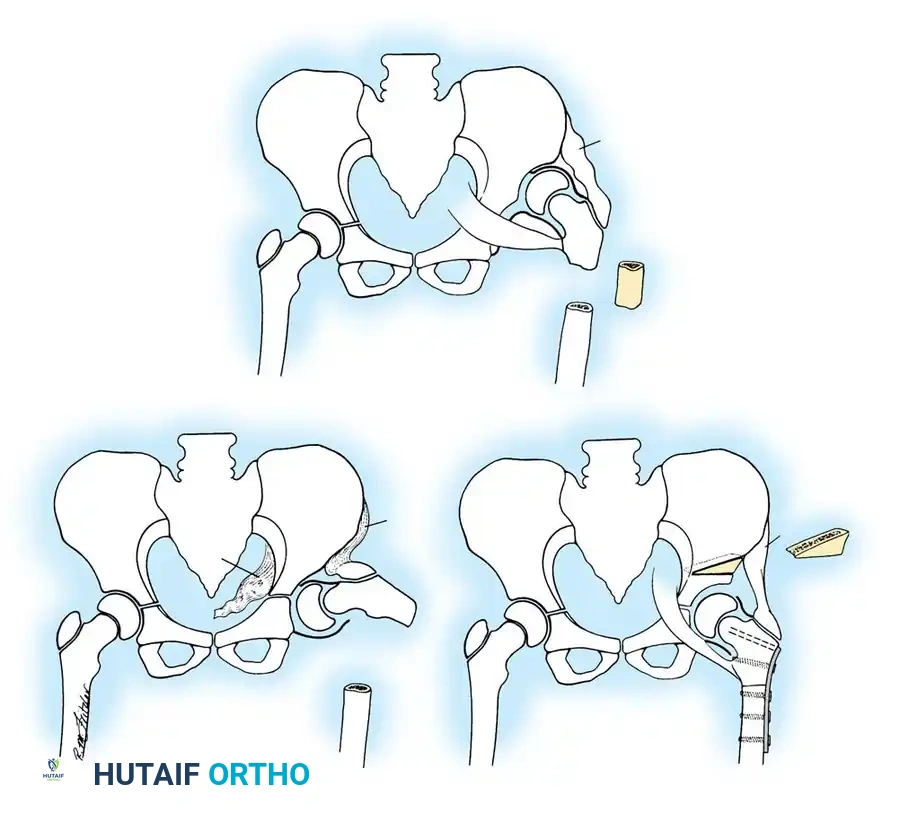
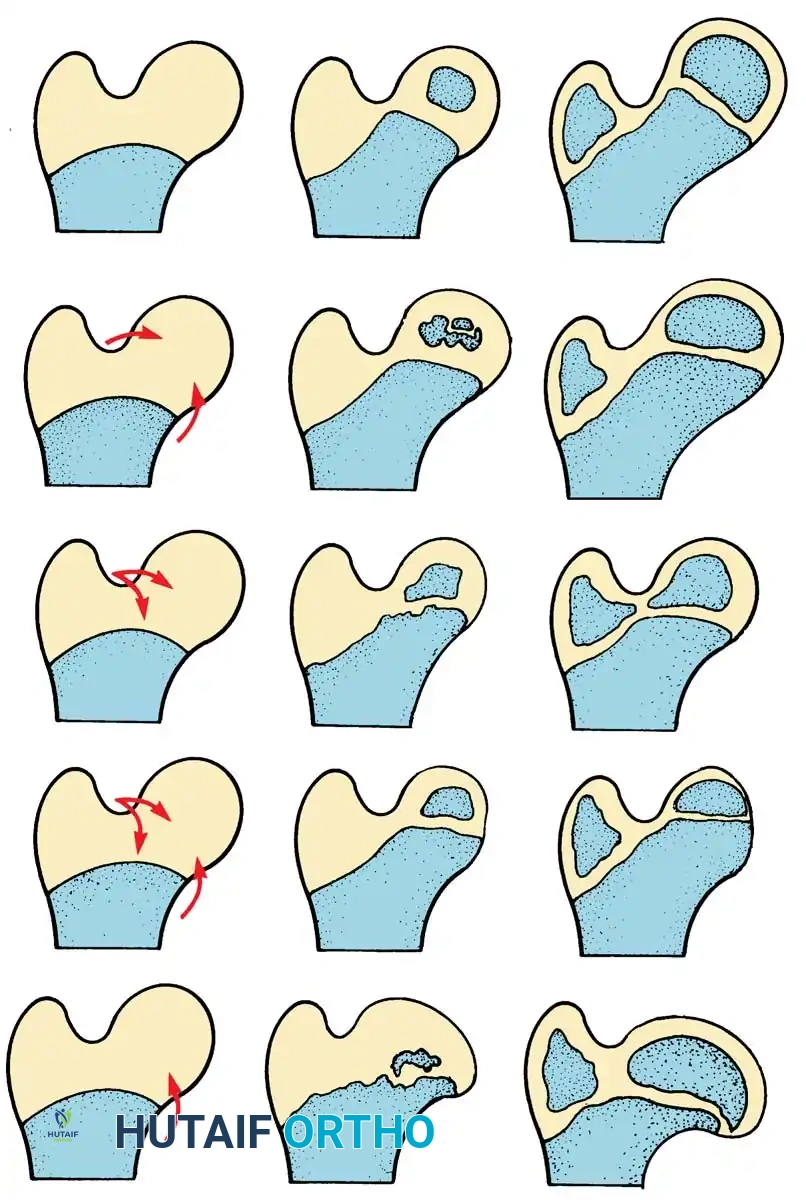
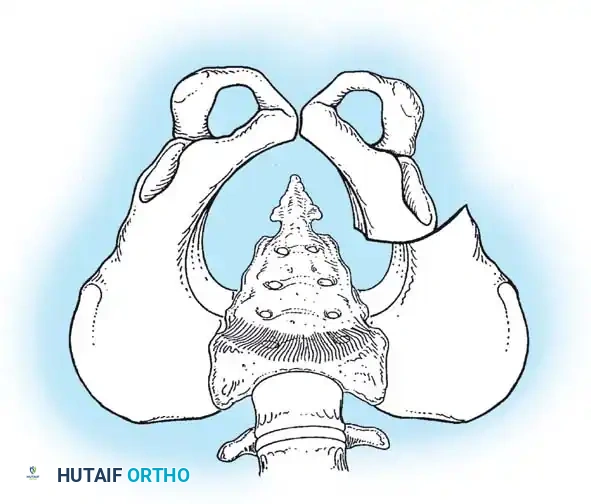
Diagrammatic representation of the Salter Innominate Osteotomy. Note the complete iliac cut and the placement of the triangular bone graft to redirect the acetabulum.
- Pemberton Pericapsular Osteotomy:
- Indications: Severe dysplasia with a capacious acetabulum.
- Biomechanics: An incomplete cut is made through the ilium, curving down to the triradiate cartilage, which acts as a hinge. This reshapes the acetabular roof, reducing its volume and improving anterolateral coverage.
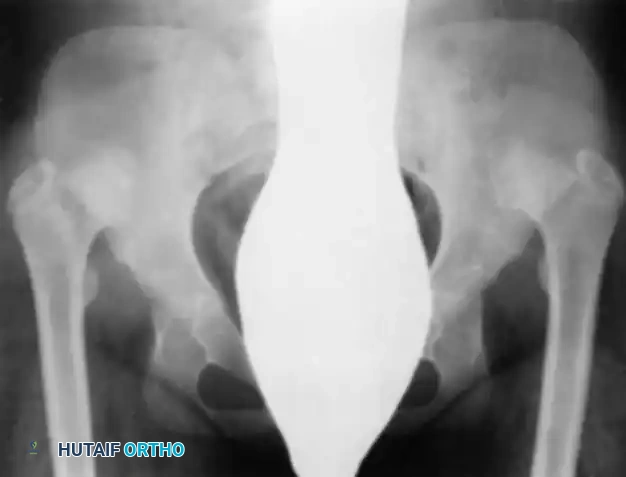
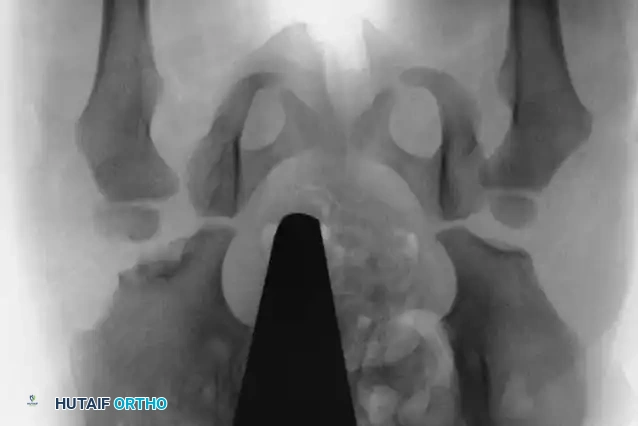
Radiographic appearance following a complex pelvic osteotomy with internal fixation, demonstrating improved center-edge angle and acetabular coverage.
Postoperative Protocols and Complications
Immobilization:
Following open reduction and osteotomy, patients are placed in a 1.5 spica cast for 6 to 8 weeks. Upon cast removal, an abduction orthosis may be utilized at night to maintain the reduction while allowing daytime mobilization and physical therapy.
Avascular Necrosis (AVN):
The most devastating complication of DDH treatment is iatrogenic AVN of the femoral head. It is caused by vascular compromise to the medial circumflex femoral artery, usually due to extreme abduction in a cast/harness or excessive compressive forces during reduction.
* Prevention: Adherence to the safe zone of Ramsey, liberal use of adductor tenotomies, avoidance of the frog-leg position, and utilization of femoral shortening osteotomies in older children.
* Management: If AVN occurs, treatment is supportive, aiming to maintain range of motion and contain the femoral head within the acetabulum during the fragmentation and reossification phases to prevent coxa magna and hinge abduction.
Conclusion
The management of Congenital and Developmental Dysplasia of the Hip demands a rigorous, evidence-based approach. From the meticulous
Associated Surgical & Radiographic Imaging