Introduction & Epidemiology
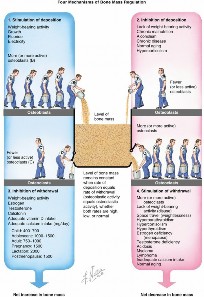
Bone mass homeostasis is a dynamic process meticulously regulated by the continuous interplay between osteoblastic bone deposition and osteoclastic bone withdrawal. This intricate balance ensures skeletal integrity and adaptability, maintaining bone strength against physiological loads. Disruptions in this equilibrium lead to a spectrum of bone mineral density (BMD) conditions, with osteoporosis being the most prevalent and clinically significant.
Osteoporosis is characterized by an age-related decrease in bone mass, coupled with microarchitectural deterioration of bone tissue, leading to increased bone fragility and susceptibility to fracture. While it can affect individuals of any age, it is typically associated with estrogen loss in postmenopausal women, accelerating bone turnover and resorption. Critically, osteoporosis represents a quantitative defect in bone mass, not a qualitative one; the remaining bone matrix is normally mineralized.
The World Health Organization (WHO) provides diagnostic criteria based on bone densitometry using Dual-energy X-ray Absorptiometry (DEXA) scans. Specifically, osteoporosis is defined by a lumbar spine (L2–L4), femoral neck, or total hip BMD T-score of -2.5 or more standard deviations below the mean peak bone mass of a healthy 25-year-old reference population. The precursor condition, osteopenia, is diagnosed when the T-score ranges from -1.0 to -2.5 standard deviations below this mean peak bone mass.
The epidemiological impact of osteoporosis is profound. It is responsible for more than 1 million fragility fractures annually in the United States alone. Fractures of the vertebral body are the most common osteoporotic fractures, often presenting insidiously with chronic back pain or progressive kyphosis. A history of osteoporotic vertebral compression fractures (VCFs) is a powerful predictor of subsequent vertebral fracture, with the risk for a second VCF increasing by approximately 20% after an initial event. Beyond morbidity, VCFs are independently associated with a significant increase in mortality rate, underscoring the systemic implications of skeletal fragility. Other common fragility fractures include those of the proximal femur (hip), distal radius, and proximal humerus, all carrying substantial burdens of pain, disability, and healthcare costs. Beyond osteoporosis, other conditions affecting BMD and bone quality, such as osteomalacia, Paget's disease, hyperparathyroidism, long-term corticosteroid use, and metastatic disease, significantly influence surgical strategy and outcomes in the orthopedic realm.
Surgical Anatomy & Biomechanics
The anatomical and biomechanical consequences of compromised BMD are central to understanding fragility fractures and their surgical management. Normal bone comprises a robust cortical shell and an intricate trabecular network, both contributing to structural integrity. In osteoporotic bone, the microarchitecture undergoes significant deterioration. This involves thinning of the cortical bone, reduction in trabecular bone volume, thinning of individual trabeculae, and most critically, a loss of trabecular connectivity. This loss transforms a strong, interconnected lattice into a sparse, discontinuous framework, drastically reducing bone's ability to withstand stress and strain.

The biomechanical implication is a disproportionate reduction in bone strength relative to the decrease in BMD. Fragility fractures, by definition, occur from low-energy trauma that would not typically cause a fracture in healthy bone. The characteristic patterns of these fractures are often dictated by areas of high trabecular content and stress concentration, such as the vertebral bodies, femoral neck and intertrochanteric region, distal radius metaphysis, and proximal humeral metaphysis.
Specific anatomical considerations for common fragility fractures include:
*
Vertebral Bodies:
The vertebral endplates and central vertebral body are rich in trabecular bone, making them vulnerable to axial compression. The typical wedge or biconcave deformities seen in VCFs reflect this collapse. Loss of vertebral height and progressive kyphosis alter spinal mechanics, potentially leading to adjacent segment disease or further fractures.
*
Proximal Femur:
This region, including the femoral neck and intertrochanteric area, is critical for weight-bearing. The femoral neck, with its relatively thin cortex and high proportion of trabecular bone, is susceptible to shear and bending forces. Intertrochanteric fractures involve both cortical and cancellous bone, often with comminution due to weakened cancellous architecture. The ability of implants to achieve stable fixation in this region is severely challenged by poor bone quality.
*
Distal Radius:
The metaphysis of the distal radius is primarily cancellous. In osteoporosis, the weakened cancellous bone combined with relatively thin cortical bone leads to typical Colles' or Smith's fracture patterns, often with significant dorsal comminution and metaphyseal collapse.
*
Proximal Humerus:
The humeral head and metaphysis are largely cancellous. Fractures here often present as two-, three-, or four-part patterns, with comminution of the greater and lesser tuberosities and valgus or varus impaction of the head, making stable reduction and fixation challenging.

From a surgical perspective, bone quality—beyond mere density—is paramount. The reduced mechanical properties of osteoporotic bone directly impact implant anchorage, pullout strength, and the risk of cutout. Traditional non-locking fixation may fail due to micromotion at the bone-implant interface, leading to screw loosening or cutout. Even locking plate constructs, designed to create a fixed-angle construct independent of plate-bone compression, can suffer from screw pullout if the underlying bone stock is insufficient. This necessitates careful consideration of implant design, fixation augmentation, and load-sharing principles in operative planning.
Indications & Contraindications
The decision to proceed with operative or non-operative management for fractures in the setting of compromised BMD is multifaceted, balancing fracture characteristics, patient comorbidities, functional demands, and bone quality.
Non-Operative Indications
- Stable Fractures: Minimal displacement, inherently stable fracture patterns, or those that achieve stability with external immobilization (e.g., brace, cast).
- Minimal Displacement/Angulation: Fractures where the deformity is acceptable and unlikely to lead to long-term functional impairment or pain.
- Manageable Pain: Fractures whose pain can be adequately controlled with analgesics and immobilization, without resorting to surgery.
- High Surgical Risk: Patients with severe comorbidities (e.g., advanced cardiac disease, severe pulmonary dysfunction) where the risks of anesthesia and surgery outweigh the potential benefits, provided the fracture is stable and non-operative management is feasible.
- Functional Limitations: Patients with pre-existing severe functional limitations (e.g., non-ambulatory, severe dementia) where surgical intervention may not significantly improve their overall quality of life or function.
Operative Indications
- Unstable Fractures: Fractures prone to displacement, collapse, or those that cannot maintain reduction with non-operative means.
- Significant Displacement/Angulation: Fractures with unacceptable deformity that is likely to result in functional impairment, malunion, or persistent pain. This includes articular step-offs or incongruity.
- Neurological Deficit: Spinal fractures with evidence of spinal cord or nerve root compression requiring decompression and stabilization.
- Intractable Pain: Persistent, severe pain despite adequate non-operative measures, particularly for VCFs where vertebroplasty/kyphoplasty can provide rapid relief.
- Failed Non-Operative Treatment: Progression of deformity, loss of reduction, or worsening pain despite adherence to conservative protocols.
- Impending or Pathological Fractures: Due to metastatic disease or other primary bone tumors, often requiring prophylactic stabilization or resection/reconstruction.
-
Certain Fracture Types:
- Proximal Femur Fractures: Almost universally require surgical fixation or arthroplasty due to high rates of nonunion, avascular necrosis, and prolonged immobility with conservative management. Exceptions are rare, stable impacted femoral neck fractures in non-ambulatory patients with high surgical risk.
- Vertebral Compression Fractures (VCFs): While many are managed conservatively, indications for vertebroplasty or kyphoplasty include acute, painful VCFs unresponsive to conservative therapy, especially in the setting of persistent disability. Open surgical stabilization is reserved for progressive neurological deficit, significant spinal instability, or canal compromise.
- Displaced Distal Radius Fractures: Often require open reduction and internal fixation (ORIF) with volar locking plates to restore anatomical alignment and allow early motion.
- Displaced Proximal Humerus Fractures: Significant displacement, angulation, or head-split patterns, particularly in functionally active patients, warrant surgical intervention, ranging from ORIF to hemiarthroplasty or reverse shoulder arthroplasty.
Contraindications
- Severe Uncorrectable Comorbidities: Patients who are medically unstable or have a prohibitively high anesthetic risk that cannot be mitigated.
- Active Local or Systemic Infection: Surgery should be delayed until the infection is controlled to prevent implant contamination and septic complications.
- Non-Reconstructible Bone: Severely comminuted fractures or extremely poor bone stock where stable internal fixation is impossible, necessitating palliative care or alternative strategies (e.g., excision arthroplasty for complex humeral fractures in frail patients).
- Patient Refusal: Competent patients' refusal of surgical intervention.
Operative vs. Non-Operative Indications for Fragility Fractures
| Fracture Type | Primary Operative Indications | Primary Non-Operative Indications |
|---|---|---|
| Vertebral Body |
- Acute, painful VCFs refractory to conservative care (vertebroplasty/kyphoplasty)
- Neurological deficit (spinal cord/nerve root compression) - Progressive kyphosis or spinal deformity - Major spinal instability (e.g., burst fracture with canal compromise) |
- Stable VCFs with mild to moderate pain controlled by analgesics and bracing
- Chronic, asymptomatic VCFs - VCFs with minimal height loss and no neurological deficit - Medically unfit patients for spinal intervention |
| Proximal Femur |
- Displaced femoral neck fractures (ORIF, hemi/total arthroplasty)
- Intertrochanteric fractures (IM nailing) - Subtrochanteric fractures (IM nailing) - Impending pathological fractures |
- Extremely rare: Stable, impacted femoral neck fractures in non-ambulatory, very frail patients with prohibitive surgical risk (controversial and high failure rate)
- Certain stress fractures prior to completion (rarely applies to fragility fractures) |
| Distal Radius |
- Displaced intra-articular fractures (>2mm step-off)
- Unstable extra-articular fractures (e.g., dorsal comminution, significant volar/dorsal angulation, radial shortening) - Median nerve compression symptoms - Open fractures |
- Nondisplaced or minimally displaced stable fractures
- Displaced fractures amenable to closed reduction and cast immobilization with acceptable post-reduction parameters (age-dependent, less common in active patients with poor bone quality) - Patients with extremely high surgical risk and low functional demands (palliative approach) |
| Proximal Humerus |
- Significantly displaced anatomical neck fractures
- Displaced 3- or 4-part fractures (ORIF, hemi/reverse arthroplasty) - Glenoid articulation involvement - Neurological compromise (e.g., axillary nerve injury with brachial plexus involvement) |
- Nondisplaced or minimally displaced 1- or 2-part fractures
- Stable impacted valgus fractures - Frail, low-demand patients with acceptable deformity and pain controlled by sling immobilization |
| Other Long Bones |
- Unstable shaft fractures
- Articular involvement with significant displacement - Open fractures - Pathological fractures requiring stabilization - Failed non-operative treatment with nonunion/malunion |
- Nondisplaced or stable fractures amenable to cast/brace immobilization
- Certain stable stress fractures |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount in managing fragility fractures, given the systemic nature of osteoporosis and the inherent challenges of fixing osteoporotic bone.
Systemic Evaluation and Optimization
- Medical Comorbidity Assessment: Comprehensive review of cardiac, pulmonary, renal, and neurological status. Optimize pre-existing conditions (e.g., manage hypertension, diabetes, anemia, chronic obstructive pulmonary disease).
- Nutritional Status: Assess for malnutrition, vitamin D deficiency, and calcium insufficiency. Supplementation may be initiated pre-operatively if time permits, though immediate fracture management often precedes full optimization.
-
Medication Review:
- Anticoagulants/Antiplatelets: Meticulous management of perioperative anticoagulation, potentially bridging with agents like low molecular weight heparin (LMWH) if surgical delay is necessary.
- Bone-Active Agents: Bisphosphonates, denosumab, teriparatide, romosozumab. These agents impact bone remodeling and healing. While typically continued, there are specific considerations, e.g., temporary cessation of denosumab due to rebound bone resorption risk. The timing of surgery is rarely dictated by these medications unless there's a concern for atypical femoral fracture.
- Corticosteroids: Chronic corticosteroid use impairs bone healing and increases infection risk; appropriate stress dose steroids may be required.
- Anesthesia Consultation: Early involvement of anesthesiology to assess risk and plan anesthetic management, considering regional block options.
Radiographic Assessment
- Standard Radiographs: At least two orthogonal views are essential for initial fracture characterization. Specific views (e.g., Judet views for acetabular fractures, oblique views for distal radius) are obtained as needed.
-
Computed Tomography (CT):
- 3D Reconstructions: Invaluable for complex articular or highly comminuted fractures (e.g., proximal humerus, tibial plateau, acetabulum), aiding in understanding fracture morphology and planning reduction strategies.
- Bone Stock Assessment: CT can provide a qualitative assessment of bone density and delineate areas of cortical thinning or extensive comminution.
- Spinal Fractures: Essential for evaluating canal compromise, posterior element integrity, and planning pedicle screw trajectories.
- Magnetic Resonance Imaging (MRI): Primarily for spinal fractures to differentiate acute from chronic VCFs, assess ligamentous injury, and evaluate for spinal cord compression or edema. Less commonly used for appendicular fractures unless soft tissue injury (e.g., rotator cuff tear with proximal humerus fracture) or occult fracture is suspected.
- DEXA Scan: If not previously performed, a DEXA scan should be obtained post-operatively to diagnose osteoporosis and guide medical management to prevent future fractures. It is not typically part of acute pre-operative planning for fracture type.
Bone Quality Assessment & Implant Selection
- Beyond T-score: While DEXA provides BMD, it doesn't fully capture bone quality. Qualitative assessment from CT (e.g., cortical thickness, trabecular pattern) informs implant choice. Advanced techniques like finite element analysis (FEA) or quantitative CT (QCT) are research tools but hold promise for more precise pre-operative bone strength prediction.
-
Implant Strategy for Osteoporotic Bone:
- Cement Augmentation: Polymethy|methacrylate (PMMA) injection around screws (e.g., pedicle screws, locking plate screws) or within the fracture site (e.g., kyphoplasty, augmented femoral neck screws) significantly enhances pullout strength.
- Locking Plate Constructs: Provide fixed-angle stability independent of bone quality but still require adequate bone for screw purchase.
- Intramedullary Nailing: Load-sharing properties are advantageous, and newer designs incorporate increased screw options or augmentation.
- Arthroplasty: Often preferred for highly comminuted articular fractures (e.g., proximal humerus, femoral neck) in the elderly with poor bone quality, as it bypasses the need for fracture healing in compromised bone.
- Multiple Fixation Points: Spreading loads across more screws/pins.
- Larger Diameter Screws/Nails: Where anatomically feasible.
Informed Consent
Thorough discussion of specific risks associated with osteoporotic bone, including higher rates of implant pullout, loosening, nonunion, and malunion.
Patient Positioning
- Fracture-Specific: Dictated by the fracture location and planned surgical approach.
- Stability: Ensure the patient is safely secured to prevent intraoperative movement.
- Accessibility: Adequate exposure for the surgical field and C-arm fluoroscopy. For hip fractures, a fracture table is commonly used. For distal radius, hand table. For humerus, beach chair or supine with bolster.
-
Neurological Monitoring:
Consider somatosensory evoked potential (SSEP) monitoring for complex spinal or pelvic procedures.

Detailed Surgical Approach / Technique
Surgical intervention for fragility fractures demands meticulous technique, an understanding of osteoporotic bone's limitations, and an adaptive approach to achieve stable fixation and optimize outcomes. The core principles include gentle tissue handling, maximizing implant-bone interface strength, utilizing load-sharing constructs, and minimizing further soft tissue devitalization.
General Principles for Osteoporotic Bone Surgery
- Gentle Tissue Handling: Preserve periosteal blood supply and minimize soft tissue stripping to promote healing in already compromised bone.
- Indirect Reduction Techniques: Utilize ligamentotaxis and traction rather than aggressive direct manipulation to avoid further comminution.
- Maximal Fixation Points: Employ constructs that allow for a greater number of screws or pins, distributed appropriately.
-
Augmented Fixation:
- Cement Augmentation (PMMA): For screws in metaphyseal or cancellous bone (e.g., pedicle screws, locking plate screws in proximal humerus/femur), vertebroplasty, kyphoplasty.
- Locking Plates: Provide angular stability, crucial in osteoporotic bone by creating a fixed-angle construct that does not rely on plate-to-bone compression.
- Intramedullary Nailing: Offers central load sharing and can be less disruptive to periosteal blood supply, particularly for long bone diaphyseal/metaphyseal fractures.
- Load-Sharing Constructs: Design implant placement to share stress between the implant and the bone, rather than pure load bearing by the implant alone.
- Minimally Invasive Approaches: Where feasible, reduce surgical exposure to preserve vascularity and soft tissue envelope, potentially reducing infection rates and improving healing.
Vertebral Compression Fractures (VCFs)
For acute, painful VCFs refractory to conservative management:
1.
Vertebroplasty:
*
Patient Positioning:
Prone on a radiolucent table.
*
Approach:
Unilateral or bilateral transpedicular approach under fluoroscopic guidance. A bone biopsy needle or specialized cannula is advanced into the vertebral body.
*
Cement Injection:
Low-viscosity PMMA bone cement is injected under continuous fluoroscopic visualization. The goal is adequate fill without extravasation.
2.
Kyphoplasty:
*
Patient Positioning:
Prone.
*
Approach:
Similar transpedicular approach.
*
Balloon Inflation:
A balloon tamp is advanced into the vertebral body, inflated to create a cavity and potentially restore some vertebral height and correct kyphosis.
*
Cement Injection:
High-viscosity PMMA cement is then injected into the created cavity, reducing extravasation risk.
3.
Open Surgical Stabilization:
Reserved for VCFs with neurological deficits, significant canal compromise, or progressive spinal instability. This involves decompression (laminectomy), reduction, and instrumented fusion (pedicle screw fixation), potentially with anterior column support.
Proximal Femur Fractures
-
Intracapsular (Femoral Neck) Fractures:
- Non-displaced/Minimally Displaced (Garden I/II): ORIF with multiple cannulated screws (usually 3 parallel screws in an inverted triangle configuration). Careful reduction under fluoroscopy, screw length critical to avoid articular penetration. Cement augmentation of screws may be considered for severe osteoporosis.
-
Displaced (Garden III/IV):
- Hemiarthroplasty: Most common for elderly, low-demand patients. Bipolar or unipolar designs. Cemented stem preferred in osteoporotic bone.
- Total Hip Arthroplasty (THA): For active, higher-demand patients, or those with pre-existing symptomatic hip arthritis. Challenges include bone quality for acetabular component fixation.
-
Extracapsular (Intertrochanteric & Subtrochanteric) Fractures:
-
Intramedullary Nailing (IMN):
The gold standard. Load-sharing design.
- Patient Positioning: Supine on a fracture table or lateral decubitus.
- Approach: Small incision over the greater trochanter. Piriformis fossa or greater trochanteric entry point.
- Reduction: Critical for successful nailing. Traction, internal rotation, and adduction to reduce fracture. Use of lag screws, cerclage wires, or external manipulators for reduction assistance.
- Nail Insertion: Reaming to fit the nail, then careful insertion to avoid creating new fractures.
- Cephalic Screw(s): Single large lag screw or two smaller screws (e.g., helical blade, cancellous screws) inserted into the femoral head, aiming for central or inferocentral placement. Cement augmentation around these screws can improve stability.
- Distal Locking: Static or dynamic locking screws inserted distally to prevent rotation and shortening.
- Plate Fixation (e.g., Dynamic Hip Screw, Trochanteric Fixation Plate): Less commonly used for intertrochanteric fractures due to higher rates of fixation failure and peri-implant fractures in osteoporotic bone compared to IMN. May be considered for specific fracture patterns or revision cases.
-
Intramedullary Nailing (IMN):
The gold standard. Load-sharing design.
Distal Radius Fractures
For displaced, unstable fractures, particularly intra-articular:
1.
Volar Locking Plate Fixation:
*
Patient Positioning:
Supine with hand on a hand table, tourniquet.
*
Approach:
Volar Henry approach (flexor carpi radialis (FCR) tendon interval, retracting FCR ulnarly, radial artery radially). Pronator quadratus elevated or incised.
*
Reduction:
Direct visualization and manipulation, ligamentotaxis with external traction, or use of K-wires/small clamps. Restore radial length, volar tilt, and articular congruity.
*
Plate Application:
A fixed-angle volar locking plate is contoured and applied to the volar surface of the radius. The distal screws are directed to capture subchondral bone, providing angular stability. Proximal screws achieve diaphyseal purchase.
*
Screw Selection:
Locking screws are crucial. Biconcave plate designs or specific screw trajectories may be needed for severe metaphyseal comminution.
*
Soft Tissue Coverage:
Meticulous closure of pronator quadratus and superficial tissues to prevent tendon irritation.

Proximal Humerus Fractures
For displaced multi-part fractures in active patients:
1.
ORIF with Locking Plates (e.g., PHILOS plate):
*
Patient Positioning:
Beach chair or supine with a bolster under the ipsilateral scapula.
*
Approach:
Deltopectoral approach is standard, preserving deltoid insertion. Axillary nerve identified and protected.
*
Reduction:
Gentle traction and manipulation. Suture fixation of tuberosity fragments to the plate and bone is critical. Use of K-wires for temporary fixation.
*
Plate Application:
The plate is applied laterally, distal to the rotator cuff insertion. Screws are directed into the humeral head, aiming for adequate purchase in the subchondral bone. Locking screws are essential.
*
Suture Augmentation:
Non-absorbable sutures are passed through the rotator cuff tendons and plate holes to augment fixation of the tuberosities to the humeral shaft.
2.
Reverse Shoulder Arthroplasty (RSA):
Increasingly favored for complex 3- or 4-part proximal humerus fractures in elderly, osteoporotic patients with poor bone quality, particularly with rotator cuff compromise. Bypasses the need for fracture healing and provides predictable function.
*
Patient Positioning:
Beach chair.
*
Approach:
Deltopectoral.
*
Technique:
Excision of humeral head, reaming of glenoid for baseplate, fixation of glenosphere, and insertion of humeral stem (often cemented in osteoporotic bone) with polyethylene liner. Tuberosity repair around the prosthesis can improve function.

Complications & Management
Management of fragility fractures is fraught with challenges due to the underlying compromised bone quality and the frequent presence of multiple comorbidities in the patient population. Complications can be broadly categorized into general surgical complications and those specifically related to osteoporotic bone and its fixation.
General Complications
-
Infection:
Superficial or deep surgical site infection. Incidence varies by site (e.g., lower for vertebroplasty, higher for open long bone fixation).
- Management: Debridement, irrigation, antibiotics, implant retention vs. removal (based on infection severity, organism, implant stability).
-
Bleeding/Hematoma:
Can lead to wound complications, increased pain, or rarely, compartment syndrome.
- Management: Meticulous hemostasis, drains (if indicated), anti-coagulation management, observation, or evacuation.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
High risk in this population due to immobility and age.
- Management: Pharmacological (LMWH, direct oral anticoagulants) and mechanical (TED hose, intermittent pneumatic compression) prophylaxis. Early mobilization.
-
Nerve / Vascular Injury:
Iatrogenic injury during exposure or instrumentation.
- Management: Careful dissection, anatomical knowledge, intraoperative monitoring. Repair if feasible, or observation.
-
Anesthetic Complications:
Cardiac events, respiratory failure, stroke, delirium.
- Management: Pre-operative optimization, careful intraoperative monitoring, appropriate post-operative care.
Complications Specific to Osteoporotic Bone / Fixation
-
Implant Pullout / Loosening (Fixation Failure):
Due to inadequate bone stock, poor screw purchase, or cyclic loading exceeding implant-bone interface strength. Common in proximal humerus and intertrochanteric fractures.
- Incidence: Highly variable, 5-20% for some constructs in severe osteoporosis.
-
Salvage Strategies:
- Revision Surgery: Re-reduction and fixation with alternative implants (e.g., longer nails, different plate design), cement augmentation of screws, or conversion to arthroplasty (e.g., proximal humerus, hip).
- Bone Grafting/Substitutes: To enhance healing and provide structural support.
- Reduced Weight-Bearing: Prolonged protection may be necessary if fixation is marginal.
-
Nonunion / Malunion:
Delayed or failed fracture healing, or healing in an unacceptable position. Osteoporotic bone has diminished healing capacity.
- Incidence: 5-15% for various fragility fractures. Higher in femoral neck fractures treated with ORIF.
-
Salvage Strategies:
- Revision Surgery: Re-ORIF with more stable construct, bone grafting (autograft, allograft, synthetic), biological augmentation (e.g., BMPs, PRP).
- Corrective Osteotomy: For symptomatic malunion.
- Arthroplasty: For nonunion of articular fractures (e.g., femoral neck nonunion treated with THA).
-
Subsequent Fracture:
The primary osteoporotic event increases the risk of new fractures, both adjacent to the initial fracture (e.g., adjacent VCF) or at other sites.
- Incidence: 20% risk of second VCF after initial one. ~50% lifetime risk of another fragility fracture after the first.
- Salvage Strategies: Medical optimization of bone health (Calcium, Vitamin D, anti-resorptive/anabolic agents). Surgical management as per new fracture. Fracture Liaison Services are crucial here.
-
Cement Extravasation (Vertebroplasty/Kyphoplasty):
PMMA leakage outside the vertebral body. Can involve epidural space (spinal cord/nerve root compression), paravertebral veins (pulmonary embolism), or retroperitoneal structures.
- Incidence: Varies, 5-10% for vertebroplasty, lower for kyphoplasty. Symptomatic extravasation is much lower (<1%).
-
Salvage Strategies:
- Observation: For asymptomatic extravasation.
- Surgical Decompression: For symptomatic neurological deficit due to epidural extravasation.
- Anticoagulation/Supportive Care: For pulmonary embolism.
-
Periprosthetic Fracture:
Fracture occurring around an existing orthopedic implant (e.g., total hip/knee replacement, IM nail).
- Incidence: ~1-5% for THA, often requiring complex revision.
- Salvage Strategies: Often requires extensive revision surgery with long plating systems, cabling, or revision arthroplasty, taking into account bone loss and implant design.
-
Avascular Necrosis (AVN):
Particularly of the femoral head after femoral neck fracture, or humeral head after proximal humerus fracture. Due to disruption of blood supply.
- Incidence: Up to 30% for displaced femoral neck fractures treated with ORIF.
- Salvage Strategies: Arthroplasty (hemiarthroplasty or THA for hip, hemi- or reverse shoulder arthroplasty for shoulder).
Table of Common Complications and Management Strategies
| Complication | Typical Incidence (Approximate) | Salvage/Management Strategy |
|---|---|---|
| Implant Pullout/Loosening | 5-20% (site-dependent) | Revision surgery with stronger construct, cement augmentation, conversion to arthroplasty (e.g., hip, shoulder). Consider bone grafting. |
| Nonunion | 5-15% (site-dependent) | Revision surgery with re-ORIF, internal fixation with bone grafting (autograft, allograft), biological augmentation (BMPs), external fixation (rarely). Conversion to arthroplasty (e.g., femoral neck). |
| Malunion | Variable (site-dependent) | Observation for asymptomatic malunion. Corrective osteotomy for symptomatic deformity. |
| Surgical Site Infection | 1-5% | Superficial: wound care, oral antibiotics. Deep: surgical debridement, irrigation, IV antibiotics, implant retention vs. removal (based on organism, stability, chronicity). |
| DVT/PE | 1-10% | Prophylaxis: pharmacological (LMWH, DOACs), mechanical (compression devices). Treatment: therapeutic anticoagulation, IVC filter (rarely). |
| Cement Extravasation (VCFs) | 5-10% (clinically significant <1%) | Asymptomatic: observation. Symptomatic (neurological deficit): surgical decompression. Pulmonary embolism: therapeutic anticoagulation. |
| Periprosthetic Fracture | 1-5% (post-arthroplasty) | Revision surgery: complex plating, cabling, revision arthroplasty, sometimes with allograft-prosthesis composites. |
| Avascular Necrosis | Up to 30% (femoral neck) | Arthroplasty (hemiarthroplasty, total hip/shoulder arthroplasty). |
| Subsequent Fragility Fracture | High (e.g., 20% for 2nd VCF) | Aggressive medical management of osteoporosis (Calcium, Vit D, bisphosphonates, denosumab, anabolic agents). Fracture Liaison Services. Prophylactic fixation (rarely). |
| Nerve/Vascular Injury | Rare (<1%) | Intraoperative repair if recognized. Postoperative monitoring. EMG/NCS. Symptomatic nerve injury may require neurolysis or tendon transfers. |
| Medical Complications (e.g., delirium, cardiac event, pneumonia) | High (due to patient age/comorbidity) | Pre-operative optimization, careful intraoperative/postoperative monitoring, early mobilization, multidisciplinary care (geriatric co-management), delirium protocols. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation for fragility fractures is crucial for functional recovery, pain management, and preventing secondary complications. It must be tailored to the individual patient, fracture stability, fixation achieved, and the underlying medical comorbidities.
Early Mobilization
- Prevention of Deconditioning: Prompt mobilization is vital to minimize muscle atrophy, loss of cardiovascular fitness, and functional decline, particularly in the elderly.
- Complication Reduction: Reduces the risk of DVT/PE, pneumonia, pressure ulcers, and urinary tract infections.
- Pain Management: Facilitates participation in therapy by addressing pain effectively using a multimodal approach (acetaminophen, NSAIDs (if no contraindications), neuropathic agents, judicious opioid use).
Weight-Bearing and Range of Motion Restrictions
-
Load-Bearing Status:
Determined by the surgeon based on fracture stability and implant purchase.
- Protected Weight-Bearing: Often initiated for long bone fractures (e.g., distal radius, proximal humerus, stable intertrochanteric fractures) with protected weight-bearing (toe-touch or partial) progressing as callus forms and bone healing progresses.
- Full Weight-Bearing as Tolerated (FWBAT): May be allowed immediately for certain stable arthroplasty constructs (e.g., hip hemiarthroplasty) or adequately stabilized intertrochanteric fractures.
- Non-Weight Bearing: Reserved for highly unstable fractures, severe comminution, or when implant failure is a significant concern.
-
Range of Motion (ROM):
- Early Active/Passive ROM: Initiated for joints not directly involved in fixation (e.g., knee/ankle for hip fracture, hand/finger for distal radius).
- Graded ROM for Fractured Joint: Protocols vary by site. For instance, protected pendulum exercises for proximal humerus, active wrist/forearm ROM for distal radius, often initiated within days to weeks post-op. Strict adherence to weight-bearing and ROM precautions is essential to prevent fixation failure.
Physical Therapy (PT)
- Initial Phase (Hospital): Focus on safe transfers, gait training with assistive devices (walker, crutches), pain control, and education on precautions.
- Subacute Phase (Home/Rehab Facility): Progressive strengthening exercises for involved and uninvolved limbs, balance training, endurance conditioning, and advanced gait training.
- Long-Term Phase (Outpatient): Functional rehabilitation, proprioceptive training, and sport-specific or activity-specific exercises as appropriate.
Occupational Therapy (OT)
- Activities of Daily Living (ADLs): Training in compensatory strategies and use of adaptive equipment for dressing, bathing, toileting, and feeding.
- Home Safety Assessment: Identification and modification of environmental hazards to prevent falls.
Bone Health Optimization (Secondary Fracture Prevention)
This is a critical component of post-operative care and must be initiated promptly in consultation with an endocrinologist or primary care physician.
*
Calcium and Vitamin D Supplementation:
Essential foundational therapy.
*
Pharmacological Agents:
*
Anti-resorptive agents:
Bisphosphonates (oral or IV), denosumab (subcutaneous), raloxifene. These slow bone breakdown.
*
Anabolic agents:
Teriparatide (parathyroid hormone analog), romosozumab (sclerostin inhibitor). These stimulate bone formation and are often reserved for severe osteoporosis or those at very high risk of future fractures.
*
Lifestyle Modifications:
Smoking cessation, reduction of alcohol intake, regular weight-bearing exercise.
*
Fall Prevention:
Multifactorial approach including balance training, vision checks, medication review, and home hazard modification.
Long-Term Follow-up
- Radiographic Monitoring: To assess fracture healing, implant integrity, and detect signs of loosening or nonunion.
- BMD Monitoring: Regular DEXA scans to assess response to medical therapy for osteoporosis.
- Adherence to Medical Therapy: Crucial for preventing subsequent fractures.
Summary of Key Literature / Guidelines
The management of bone mineral density conditions, particularly fragility fractures, is guided by robust literature and evidence-based guidelines from orthopedic, geriatric, and endocrinology societies.
-
Fracture Liaison Services (FLS): A cornerstone of secondary fracture prevention, strongly recommended by the International Osteoporosis Foundation (IOF) and National Osteoporosis Foundation (NOF). FLS programs involve a dedicated coordinator to identify, investigate, and initiate treatment for patients presenting with fragility fractures, significantly reducing the risk of subsequent fractures. Studies have consistently demonstrated the cost-effectiveness and efficacy of FLS models in improving osteoporosis diagnosis and treatment rates.
-
Vertebral Compression Fractures (VCFs):
- Vertebroplasty vs. Kyphoplasty: The initial high-impact, randomized controlled trials (RCTs) (e.g., NEJM 2009 for vertebroplasty, Spine 2009 for kyphoplasty) showed limited or no significant benefit over sham procedures for pain relief in all VCFs. However, subsequent literature and sub-group analyses suggest that for carefully selected patients with acute, painful VCFs refractory to conservative management, these procedures can provide significant, rapid pain relief and functional improvement, with kyphoplasty potentially offering better height restoration and lower cement extravasation rates. The American Academy of Orthopaedic Surgeons (AAOS) guidelines recommend against routine vertebroplasty/kyphoplasty but acknowledge their role for intractable pain.
- Conservative Management: Remains the initial approach for most VCFs, involving pain control, activity modification, and bracing.
-
Proximal Femur Fractures:
-
Femoral Neck Fractures:
- Displaced: For elderly patients (>65-70 years), arthroplasty (hemiarthroplasty or THA) generally yields better functional outcomes and lower reoperation rates compared to ORIF, especially for displaced fractures. THA is often preferred for active, cognitively intact patients with pre-existing arthritis.
- Non-displaced: ORIF with cannulated screws is the standard. However, rates of nonunion and AVN remain significant, necessitating close follow-up.
- Intertrochanteric Fractures: Intramedullary nailing (IMN) is the preferred method for most unstable intertrochanteric fractures, offering biomechanical advantages over plate fixation (e.g., dynamic hip screw) in osteoporotic bone due to its central load-sharing mechanism and reduced bending moments. The AAOS guidelines support IMN for unstable intertrochanteric fractures.
- Cement Augmentation: Emerging evidence supports the use of PMMA augmentation for cephalic screws in IMN for unstable intertrochanteric fractures in severely osteoporotic bone, showing improved pullout strength and reduced cutout rates in biomechanical studies and some clinical series.
-
Femoral Neck Fractures:
-
Distal Radius Fractures:
- Volar Locking Plate Fixation: Widely considered the gold standard for unstable, displaced distal radius fractures, particularly in osteoporotic patients. It allows for rigid fixation, anatomical reduction, and early mobilization, leading to superior functional outcomes compared to cast immobilization alone or K-wire fixation in many cases. The benefits are most pronounced in patients needing early return to function.
-
Proximal Humerus Fractures:
- ORIF vs. Arthroplasty: For complex 3- or 4-part fractures in elderly osteoporotic patients, the evidence comparing ORIF with locking plates to reverse shoulder arthroplasty (RSA) continues to evolve. While ORIF can achieve good results in carefully selected patients, RSA is increasingly recognized as a reliable option for these complex fractures, particularly in the presence of rotator cuff deficiency, comminution, or severe osteoporosis, offering predictable pain relief and functional recovery, bypassing the challenges of osteoporotic fracture healing.
-
Pharmacological Management of Osteoporosis: Numerous guidelines (e.g., NOF Clinician's Guide, Endocrine Society Clinical Practice Guidelines) outline the use of anti-resorptive (bisphosphonates, denosumab) and anabolic agents (teriparatide, romosozumab) for fracture prevention. Orthopedic surgeons are crucial in initiating the referral for these therapies post-fracture. There is growing evidence of "osteosarcopenia" where osteoporosis co-exists with sarcopenia, requiring a combined approach to both bone and muscle health.
The current literature emphasizes a multidisciplinary approach to fragility fracture care, integrating surgical expertise with geriatric co-management, bone health optimization, and dedicated rehabilitation, to improve outcomes and prevent the cascade of recurrent fractures.
