Comprehensive Introduction and Patho-Epidemiology
The cavus foot is an exceedingly complex, multiplanar deformity characterized by an abnormally elevated medial longitudinal arch, frequently accompanied by hindfoot varus, forefoot pronation, midfoot equinus, and clawing of the lesser digits. Patients afflicted with this condition present to the orthopedic surgeon for a myriad of reasons, ranging from intractable metatarsalgia and recurrent lateral ankle instability to progressive gait deterioration, pre-ulcerative plantar callosities, and catastrophic failure of the lateral ligamentous complex. The architectural distortion of the foot fundamentally alters the weight-bearing mechanics of the lower extremity, creating a rigid, non-shock-absorbing construct that transmits pathologic forces proximally through the ankle, knee, and axial skeleton.
It is a fundamental and non-negotiable orthopedic maxim that a bilateral, or progressively unilateral, cavus foot is a symptom of an underlying neurological disorder until proven otherwise by exhaustive clinical and electrodiagnostic evaluation. While idiopathic cases certainly exist within the population, a meticulous clinical, neurological, and radiographic evaluation is absolutely mandatory to rule out progressive neuromuscular pathologies before formulating any surgical plan. The etiology of the cavus foot dictates not only the natural history of the deformity but also the predictable success or failure of joint-sparing reconstructive procedures.
The pathogenesis of the neuromuscular cavus foot is driven by highly specific, predictable patterns of intrinsic and extrinsic muscle imbalance. Charcot-Marie-Tooth (CMT) disease, or hereditary motor sensory neuropathy, remains the most ubiquitous cause of the neuromuscular cavus foot. In CMT, the deformity is initiated by the denervation and subsequent weakness of the intrinsic foot musculature, coupled with a highly characteristic imbalance of the extrinsic leg muscles. The peroneus brevis weakens significantly before the peroneus longus, leading to an unopposed, powerful plantar flexion force exerted by the peroneus longus on the base of the first metatarsal. Simultaneously, the tibialis anterior weakens before the tibialis posterior, contributing to global forefoot equinus and further exacerbating the elevation of the longitudinal arch.

In stark contrast to the progressive neuropathy of CMT, patients presenting with cavus deformity secondary to residual poliomyelitis or static encephalopathy exhibit distinctly different physical findings. The post-polio foot typically features a combination of anterior and posterior deformities driven by static, non-progressive muscle imbalance. For instance, a profoundly weak gastrocnemius-soleus complex opposing a strong anterior tibial muscle will inevitably precipitate a calcaneocavus deformity. Conversely, a strong gastrocnemius-soleus and posterior tibial muscle combined with weak toe extensors and anterior tibial muscles results in severe equinocavus. Because sensation generally remains completely intact and the deformity is non-progressive, post-polio patients generally possess a more predictable and durable surgical prognosis than those afflicted with progressive demyelinating or axonal neuropathies.
Detailed Surgical Anatomy and Biomechanics
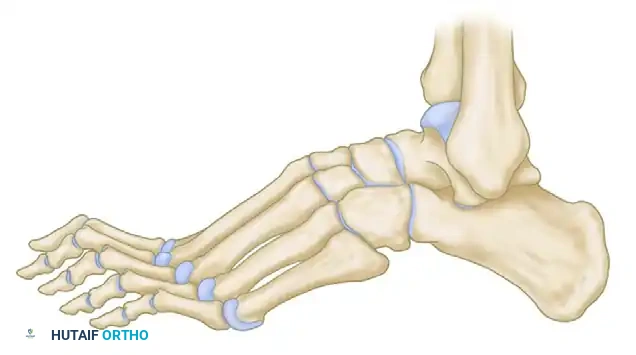
A profound understanding of the biomechanics of the cavus foot is the absolute prerequisite for rational surgical decision-making. The deformity is primarily driven by the "tripod effect," a biomechanical model that perfectly elucidates the cascade of secondary deformities observed in the hindfoot and ankle. In the normal foot, weight is distributed evenly across the calcaneal tuberosity and the metatarsal heads. In the cavus foot, the rigid, plantar flexed first ray acts as an abnormally long, anterior-medial leg of this tripod, completely disrupting normal load distribution during the stance phase of the gait cycle.


During the heel-strike and early stance phase of gait, as the rigidly plantar flexed first metatarsal prematurely strikes the ground, it disproportionately loads the medial column of the foot. Because the midfoot joints (specifically the tarsometatarsal and naviculocuneiform joints) are rigidly locked in this pathological position, the ground reaction force cannot be absorbed by normal sagittal plane dorsiflexion. Consequently, the entire foot must rotate around the axis of the subtalar joint to accommodate this rigid anterior pillar. The hindfoot is mechanically and forcefully driven into a compensatory varus position to allow the lateral border of the foot to contact the ground.

Over time, this chronic, repetitive compensatory hindfoot varus leads to severe attenuation and eventual incompetence of the lateral ligamentous complex (anterior talofibular ligament and calcaneofibular ligament). Patients develop recurrent ankle sprains, which further destabilize the hindfoot. As the deformity progresses chronologically, the initially flexible soft-tissue contractures of the subtalar joint capsule and the medial fascial bands become rigidly fixed. The subtalar joint undergoes asymmetric loading, leading to accelerated articular cartilage degradation, rigid degenerative joint disease, and the transition from a flexible, forefoot-driven varus to a fixed, structural hindfoot varus.
The intrinsic musculature and plantar aponeurosis play a critical role in the maintenance and exacerbation of the cavus architecture. The windlass mechanism, normally a dynamic stabilizer of the arch, becomes a static deforming force. The contracted central band of the plantar fascia acts as a bowstring, drawing the calcaneus and the metatarsal heads closer together, thereby shortening the foot and elevating the arch. The intrinsic minus clawing of the toes further depresses the metatarsal heads, exacerbating the metatarsalgia and creating a retrograde plantarflexion force on the metatarsophalangeal joints.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the cavus foot requires a meticulous balancing of the patient's symptoms, the flexibility of the deformity, and the underlying neurological prognosis. Surgical indications are primarily driven by the failure of comprehensive non-operative management to control pain, prevent progressive instability, or heal pre-ulcerative lesions. Patients with intractable metatarsalgia beneath the first and fifth metatarsal heads, recurrent lateral ankle instability refractory to bracing and physical therapy, or progressive gait deterioration due to severe foot drop are prime candidates for surgical reconstruction.
Furthermore, the presence of a progressive deformity in a young patient with an established diagnosis of Charcot-Marie-Tooth disease often warrants earlier surgical intervention. In these cases, proactive joint-sparing osteotomies and tendon transfers are indicated to rebalance the foot, preserve articular cartilage, and prevent the inevitable progression to rigid, end-stage arthrosis that would eventually necessitate a joint-sacrificing triple arthrodesis. The goal is to convert a rigid, non-braceable foot into a plantigrade, supple, and orthotically accommodative extremity.
Contraindications to surgical intervention are equally critical to recognize to prevent catastrophic postoperative complications. Absolute contraindications include active deep space infection, severe peripheral arterial disease precluding wound healing, and medically unstable patients unable to tolerate prolonged anesthesia. Relative contraindications revolve primarily around the patient's sensory status and the severity of their neurological decline. Surgery in the presence of profound peripheral neuropathy with complete loss of protective sensation is fraught with extreme risk, including the precipitation of Charcot neuroarthropathy, chronic non-healing ulcerations, and eventual amputation.
| Category | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Symptoms | Intractable metatarsalgia, recurrent ankle sprains, painful plantar callosities. | Asymptomatic deformity well-managed with custom orthotics or AFOs. |
| Deformity Progression | Progressive structural changes, impending skin breakdown, failure of conservative care. | Active, untreated deep space foot infection or osteomyelitis. |
| Neurological Status | Intact or adequate protective sensation, predictable muscle imbalances amenable to transfer. | Profound loss of protective sensation (high risk of Charcot arthropathy). |
| Vascular Status | Palpable pulses, biphasic/triphasic Doppler signals, adequate ABI/TBI. | Severe peripheral arterial disease, ABI < 0.5, lack of capillary refill. |
| Joint Integrity | Flexible deformity (joint-sparing), or rigid painful arthritis (arthrodesis indicated). | Medical comorbidities precluding safe administration of anesthesia. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning begins with an exhaustive clinical examination, focusing specifically on motor strength grading, sensory mapping, and the rigorous assessment of deformity flexibility. The cornerstone of the cavus foot physical examination is the Coleman block test (lateral block test). This indispensable maneuver determines unequivocally whether the hindfoot varus is flexible (driven by the rigid forefoot) or fixed (a rigid structural change within the subtalar joint complex). The patient stands with the heel and lateral border of the foot on a 1-inch wooden block, allowing the plantar flexed first metatarsal to hang free off the medial edge. If the hindfoot varus corrects to a neutral or slight valgus position, the deformity is deemed flexible, and surgical correction can focus primarily on the forefoot and midfoot. If the hindfoot remains in varus, the deformity is fixed, mandating a concurrent calcaneal osteotomy or subtalar arthrodesis.
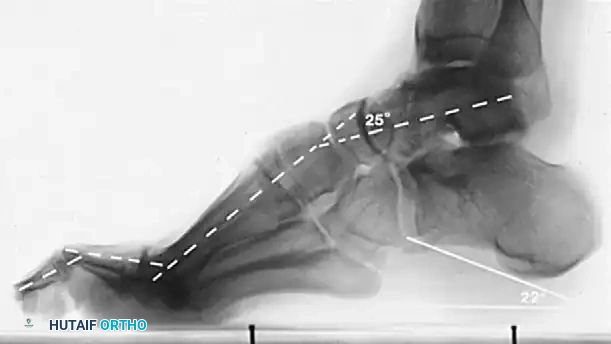
Radiographic evaluation requires meticulous analysis of standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot, along with weight-bearing AP and mortise views of the ankle. On the lateral radiograph, Meary’s angle (the longitudinal axis of the talus intersecting the longitudinal axis of the first metatarsal) is critically evaluated; in a normal foot, this is 0 degrees, but in a cavus foot, it is drastically increased with a dorsally directed apex. The Hibbs angle (intersection of the calcaneal axis and first metatarsal axis) approaches 90 degrees in severe cases. The calcaneal pitch must be measured to differentiate between etiologies. In CMT, patients typically exhibit severe forefoot equinus with a relatively normal calcaneal pitch (20-30 degrees). In post-polio patients, the calcaneal pitch is often drastically increased, indicative of a true calcaneocavus deformity driven by a paralyzed triceps surae.


Patient positioning in the operating theater must be meticulously executed to ensure optimal access to all aspects of the foot and ankle, as cavus reconstruction frequently requires multiple sequential incisions. The patient is placed strictly supine on a radiolucent operating table. A large gel bump is placed under the ipsilateral hip to internally rotate the lower extremity, bringing the naturally externally rotated foot into a neutral, vertical position. This is critical for visualizing the lateral wall of the calcaneus during osteotomies and the lateral fibula during tendon transfers. A well-padded pneumatic thigh tourniquet is applied to provide a bloodless surgical field, though a calf tourniquet may be utilized depending on surgeon preference and the proximal extent of the planned tendon harvests.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of the cavus foot is an exercise in sequential, logical reconstruction. The overarching philosophy is to correct the deformity from proximal to distal, soft tissue to bone, and posterior to anterior. The goal is a plantigrade, stable, and braceable foot. Failure to adhere to a strict sequence will result in under-correction and persistent pathological biomechanics.
Soft Tissue Releases and Plantar Fasciotomy
Soft tissue contractures must be aggressively addressed before any osseous correction is attempted; attempting to close an osteotomy against a tight plantar fascia will inevitably lead to failure of fixation or recurrent deformity. The Steindler stripping (radical plantar fascia release) is the foundational first step. A 4 cm medial longitudinal incision is made over the medial aspect of the calcaneal tuberosity.
Meticulous dissection is required to identify and protect the medial calcaneal nerve branches, which are highly variable in their arborization. Once the deep fascia is incised, the origin of the plantar aponeurosis is identified. Using a key elevator or electrocautery, the plantar fascia, along with the origins of the short plantar muscles (abductor hallucis, flexor digitorum brevis, and abductor digiti minimi), are released directly off their periosteal attachments on the calcaneal tuberosity. The release must be carried laterally to ensure the lateral band of the plantar fascia is completely transected.

Tendon Transfers and Rebalancing
Following soft tissue release, dynamic rebalancing via tendon transfer is executed to remove deforming forces and augment weakened antagonists. In the classic CMT foot, the peroneus longus to peroneus brevis (PL to PB) transfer is mandatory. A lateral longitudinal incision is made over the distal fibula, extending toward the base of the fifth metatarsal. The superior and inferior peroneal retinacula are carefully incised. The peroneus longus tendon is identified as it courses cuboid groove; it is transected as distally as possible. The distal stump is allowed to retract.
The proximal stump of the peroneus longus is then woven through the peroneus brevis tendon using a Pulvertaft weave technique or a side-to-side tenodesis, depending on tendon excursion and diameter. This transfer is secured with multiple figure-of-eight non-absorbable sutures while the foot is held in maximal eversion and neutral dorsiflexion. This critical maneuver simultaneously removes the powerful, pathological plantar-flexing force on the first ray and significantly augments the eversion power of the weakened lateral compartment. For the clawed hallux, a Jones transfer is frequently performed, relocating the Extensor Hallucis Longus (EHL) to the neck of the first metatarsal, combined with an interphalangeal joint arthrodesis to prevent a drop toe.
First Metatarsal Dorsiflexion Osteotomy
If the first ray remains rigidly plantarflexed after the Steindler stripping and the PL to PB transfer, an osseous correction is required to eliminate the anterior pillar of the tripod. A dorsal longitudinal incision is made centered over the base of the first metatarsal, lateral to the EHL tendon. The periosteum is elevated, exposing the proximal metaphysis.
A dorsally based closing wedge osteotomy is planned approximately 1 to 1.5 cm distal to the first tarsometatarsal joint to avoid violating the articular cartilage. Using a sagittal saw under copious saline irrigation, a wedge of bone is excised. The plantar cortex is carefully preserved to act as a hinge. The osteotomy is then closed, effectively elevating the metatarsal head out of its plantarflexed position. Fixation is achieved using a low-profile dorsal titanium plate or, alternatively, crossed headless compression screws.

Calcaneal Osteotomies for Hindfoot Varus
If the preoperative Coleman block test demonstrated a fixed hindfoot varus, a calcaneal osteotomy is absolutely indicated. The Dwyer closing wedge osteotomy or a lateralizing sliding calcaneal osteotomy are the workhorse procedures. An oblique lateral incision is made posterior and inferior to the sural nerve and the peroneal tendons. Deep dissection exposes the lateral wall of the calcaneus.
For the Dwyer osteotomy, a laterally based wedge of bone (typically 5-10 mm at the base) is removed from the calcaneal body using an oscillating saw, taking extreme care not to violate the medial cortex, which houses the neurovascular bundle. The osteotomy is manually closed, bringing the heel out of varus and into a neutral or slightly valgus alignment. Fixation is rigidly achieved with two large-fragment (6.5mm or 7.3mm) headless compression screws directed from the posterior tuberosity into the anterior calcaneal body, or via a specialized lateral locking plate.


Arthrodesis and Salvage Procedures
In severe, rigid, end-stage deformities accompanied by advanced degenerative joint disease of the subtalar, talonavicular, or calcaneocuboid joints, joint-sparing osteotomies are completely insufficient. In these scenarios, a Triple Arthrodesis is the definitive salvage procedure. This involves extensive surgical exposure via dual incisions (anterolateral and medial).
Meticulous and aggressive cartilage debridement of all three joints is performed down to bleeding subchondral bone. The deformity is manually corrected by translating the foot laterally, elevating the midfoot, and derotating the forefoot to achieve a perfectly plantigrade position. Rigid internal fixation is achieved using a combination of large fragment screws across the subtalar and talonavicular joints, and often a specialized midfoot/hindfoot plating system across the calcaneocuboid joint. Bone grafting (autograft or orthobiologics) is frequently utilized to fill structural voids and maximize union rates.
Complications, Incidence Rates, and Salvage Management
The surgical reconstruction of the cavus foot is a major undertaking fraught with potential complications, owing to the extensive soft tissue dissection, multiple osseous cuts, and the frequently compromised neurological status of the patient demographic. The most common and clinically significant pitfall is under-correction of the deformity. Failure to recognize a fixed hindfoot varus preoperatively—often due to neglecting the Coleman block test—leads to isolated forefoot surgery. This leaves the patient with persistent lateral column overload, recurrent ankle sprains, and inevitable failure of the reconstruction.
Conversely, over-correction can be equally debilitating. Excessive dorsiflexion of the first metatarsal during a closing wedge osteotomy will result in a functionally elevated first ray. This completely unloads the medial column and drastically shifts weight-bearing forces laterally, leading to severe transfer metatarsalgia beneath the lesser metatarsal heads, which is notoriously difficult to treat. Nonunion and delayed union are also significant risks, particularly at the site of the first metatarsal base osteotomy and within the talonavicular joint during a triple arthrodesis. These complications demand meticulous joint preparation, rigid compression, and optimization of patient biology (e.g., smoking cessation, glycemic control).
Neurovascular injury is a constant intraoperative threat. The sural nerve is at extremely high risk during the lateral approach for the calcaneal osteotomy and the PL to PB tendon transfer. Similarly, the medial calcaneal branches and the posterior tibial neurovascular bundle are at risk during the Steindler stripping and medial column procedures. Vigorous retraction and careless dissection must be avoided. In neuropathic patients, the ultimate catastrophic complication is the development of Charcot neuroarthropathy or chronic ulceration postoperatively, which may ultimately necessitate major lower extremity amputation.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Under-correction (Persistent Varus) | 10% - 15% | Failure to address fixed hindfoot varus; inadequate soft tissue release. | Revision osteotomy (calcaneal lateralizing slide) or definitive Triple Arthrodesis. |
| Over-correction (Transfer Metatarsalgia) | 5% - 8% | Excessive dorsiflexion of 1st MT osteotomy; over-tightening of tendon transfers. | Lesser metatarsal Weil osteotomies; custom orthotic offloading; revision 1st MT plantarflexion osteotomy. |
| Nonunion / Delayed Union | 3% - 7% | Smoking, poor fixation construct, thermal necrosis from saw blades. | Revision open reduction internal fixation (ORIF) with autologous bone grafting and robust plating. |
| Sural Nerve Injury (Neuroma) | 2% - 5% | Direct laceration or aggressive retraction during lateral calcaneal approaches. | Conservative management (gabapentin, injections); surgical neurectomy and burying of the proximal stump into muscle. |
| Charcot Neuroarthropathy | < 2% (Higher in profound neuropathy) | Operating on an insensate foot; premature weight-bearing. | Immediate prolonged immobilization (Total Contact Casting); potential Charcot reconstruction or amputation if infected. |
Phased Post-Operative Rehabilitation Protocols
Strict, unwavering adherence to a phased postoperative rehabilitation protocol is absolutely vital for successful outcomes, particularly when managing complex osteotomies and tendon transfers in neuropathic patients whose proprioceptive feedback is inherently compromised. The rehabilitation timeline is dictated by the principles of bone healing and the necessity of protecting delicate tendon transfers during the initial phases of fibroblastic repair.
During Phase I (Weeks 0-2), the immediate postoperative priority is wound healing and edema control. The patient is placed in a well-padded, short-leg non-weight-bearing (NWB) posterior splint or bivalved cast in the operating room. The foot is immobilized in a neutral position to protect tendon transfers (specifically the PL to PB transfer). Strict elevation above the level of the heart is mandatory to mitigate postoperative swelling, which can severely compromise incision viability, particularly on the lateral calcaneal wall. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk stratification.
Phase II (Weeks 2-6) begins at the first postoperative clinic visit. The initial surgical dressings are removed, and the incisions are meticulously inspected for signs of dehiscence or infection. Sutures are typically removed between days 14 and 21, depending on the tension of the closure and the patient's vascular status. Once wound healing is confirmed, the patient is transitioned to a rigid, fiberglass short-leg cast. Strict non-weight-bearing status is maintained. This period is critical for the initial woven bone formation at the osteotomy sites and the biological incorporation of the tendon transfers.
Phase III (Weeks 6-12) marks the transition to progressive loading. At the 6-week mark, new weight-bearing radiographs are obtained to assess for bridging callus and osseous consolidation at the osteotomy and/or arthrodesis sites. If radiographic healing is deemed adequate by the operating surgeon, the patient is transitioned into a Controlled Ankle Motion (CAM) boot. Weight-bearing is progressed slowly, typically starting with 25% partial weight-bearing with crutches and advancing by 25% weekly as tolerated. Formal physical therapy is initiated, focusing initially on active range of motion of the ankle and toes, and gentle isometric strengthening of the transferred tendons.
Phase IV (Weeks 12 and beyond) focuses on functional restoration and long-term orthotic management. Patients are gradually transitioned from the CAM boot into supportive, extra-depth athletic shoes. Depending on the underlying neurological deficit (e.g., CMT foot drop), a custom Ankle-Foot Orthosis (AFO) or custom functional foot orthotics may be prescribed to protect the reconstruction and assist with gait mechanics. Physical therapy intensifies, focusing heavily on proprioceptive retraining, aggressive gait mechanics, and dynamic strengthening of the lower extremity kinetic chain. Maximal medical improvement is typically not realized until 9 to 12 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for the cavus foot is deeply rooted in several landmark biomechanical and clinical studies that have shaped modern orthopedic protocols. The foundational understanding of the deformity's flexibility was established by Coleman and Chestnut in their seminal 1977 publication, which introduced the lateral block test. This simple yet profoundly elegant clinical maneuver completely revolutionized surgical decision-making by allowing surgeons to reliably differentiate between forefoot-driven flexible hindfoot varus and rigid structural hindfoot deformity, thereby dictating the necessity of calcaneal osteotomies.
The biomechanical rationale for tendon transfers, specifically the management of the peroneus longus, was heavily influenced by the work of Ward et al. and later refined by Sammarco. These authors elucidated the exact vector forces of the extrinsic musculature in the neuropathic foot, definitively proving that the unopposed peroneus longus is the primary deforming force driving the first ray into plantar flexion. Their clinical outcome studies established the peroneus longus to peroneus brevis transfer as the gold standard for rebalancing the lateral column and removing the anterior medial pillar of the cavus tripod.
Current clinical guidelines, supported by the American Orthopaedic Foot & Ankle Society (AOFAS), strongly advocate for a joint-sparing, "a la carte" approach to the flexible cavus foot. The modern consensus dictates that osteotomies (metatarsal and calcaneal) combined with aggressive soft-tissue releases and tendon transfers yield superior long-term functional outcomes compared to primary arthrodesis. Triple arthrodesis, once the historical panacea for all cavus deformities, is now strictly relegated to a salvage role, reserved exclusively for rigid, end-stage deformities with advanced osteoarthritic changes, due to its well-documented long-term complications of adjacent joint arthrosis
