Comprehensive Introduction and Patho-Epidemiology
The surgical correction of cavovarus foot deformity represents one of the most formidable challenges in orthopedic foot and ankle surgery. This pathology is not a singular anatomical anomaly but rather a complex, multiplanar cascade of biomechanical derangements encompassing the hindfoot, midfoot, and forefoot. Successful intervention demands an exhaustive understanding of the underlying pathomechanics, meticulous preoperative planning, and precise intraoperative execution. As reconstructive surgeons, our primary objective is to restore a plantigrade, stable, and pain-free foot while preserving joint kinematics whenever feasible. The paradigm has shifted significantly over the past few decades from primarily joint-sacrificing procedures, such as triple arthrodesis, toward joint-sparing, soft-tissue-balancing, and osteotomy-driven reconstructions.
Understanding the etiology is paramount, as the underlying diagnosis heavily dictates the natural history and the durability of our surgical reconstructions. The classic etiology of the cavovarus foot is Charcot-Marie-Tooth (CMT) disease, a hereditary sensorimotor neuropathy. In CMT, a predictable pattern of muscle denervation occurs, typically beginning with the intrinsic foot musculature and progressing to the extrinsic muscles. The intrinsic minus foot leads to clawing of the toes, which subsequently depresses the metatarsal heads, exacerbating the cavus. However, the hallmark of the deformity is driven by the extrinsic muscle imbalance: the tibialis anterior and peroneus brevis weaken early, while the peroneus longus and tibialis posterior remain relatively spared and overactive.
This specific muscle imbalance creates a vicious biomechanical cycle. The unopposed pull of the robust peroneus longus powerfully plantarflexes the first ray. As the first metatarsal is driven toward the floor, it acts as a rigid kickstand during the stance phase of gait. To accommodate this plantarflexed first ray and allow the lateral column to contact the ground, the hindfoot is forced into a compensatory varus alignment. Over time, what begins as a flexible, compensatory hindfoot varus becomes a rigid, structural deformity due to contracture of the medial soft tissues (including the plantar fascia, spring ligament, and deltoid ligament) and adaptive bony changes within the subtalar and transverse tarsal joints. Therefore, addressing the plantarflexed first ray is the absolute linchpin of cavovarus reconstruction; failing to correct the forefoot will inevitably doom any hindfoot correction to failure.
Beyond CMT, the differential diagnosis for a cavovarus foot is extensive and must be systematically evaluated. Neuromuscular etiologies include poliomyelitis, cerebral palsy, Friedreich’s ataxia, spinal cord tethering, and sequelae of cerebrovascular accidents. Post-traumatic causes, such as malunited calcaneal or talar neck fractures, can also present with severe cavovarus morphology, often complicated by post-traumatic arthrosis. Idiopathic cavovarus feet do exist, but a subtle, undiagnosed neurological condition must be highly suspected and ruled out with electromyography (EMG) and nerve conduction velocity (NCV) studies before assigning this diagnosis. Regardless of the etiology, the fundamental surgical philosophy remains consistent: release contracted tissues, correct bony malalignment, and dynamically balance the foot through targeted tendon transfers.
Detailed Surgical Anatomy and Biomechanics
Mastery of the cavovarus reconstruction requires a three-dimensional appreciation of foot and ankle anatomy, particularly the neurovascular structures that are at high risk during extensive medial and lateral exposures. On the lateral aspect of the hindfoot, the sural nerve is the structure most vulnerable to iatrogenic injury. It courses posterior to the lateral malleolus, intimately associated with the short saphenous vein, and runs distally along the lateral border of the Achilles tendon and the superior peroneal retinaculum. During a lateralizing calcaneal osteotomy, the sural nerve must be meticulously identified, mobilized, and protected, as neuromas in this region are notoriously debilitating and can compromise an otherwise successful structural reconstruction.
The peroneal tendons represent the dynamic lateral stabilizers of the ankle and are central to the pathoanatomy of the cavovarus foot. The peroneus brevis and longus share a common synovial sheath posterior to the fibula, constrained by the superior peroneal retinaculum. The brevis inserts onto the base of the fifth metatarsal, acting as a primary evertor of the hindfoot. The longus, however, has a much more complex course, diving obliquely across the plantar aspect of the midfoot through the cuboid groove to insert on the plantar-lateral aspect of the medial cuneiform and the base of the first metatarsal. In the cavovarus foot, the longus overpowers the brevis, driving the first ray into plantarflexion and contributing to the varus thrust. Transferring the peroneus longus to the peroneus brevis (PL to PB) effectively removes the deforming plantarflexion force on the first ray while augmenting the eversion power of the weakened brevis.
Medially, the neurovascular bundle containing the tibial nerve and posterior tibial artery is of paramount concern, particularly during medial soft tissue releases such as a plantar fasciotomy or a complete subtalar release. The tibial nerve bifurcates into the medial and lateral plantar nerves beneath the abductor hallucis muscle fascia. Furthermore, the medial calcaneal branches, which provide crucial sensation to the weight-bearing heel pad, branch off the tibial nerve proximal to the tarsal tunnel and course superficially over the medial calcaneal tuberosity. Blind or overly aggressive release of the plantar fascia from a medial approach places these calcaneal branches at significant risk.
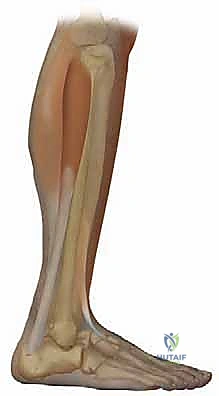
Biomechanically, the "tripod" concept of the foot is essential for understanding deformity correction. A normal foot rests on three points: the calcaneal tuberosity, the first metatarsal head, and the fifth metatarsal head. In a rigid cavovarus foot, the tripod is severely distorted. The plantarflexed first ray acts as an abnormally long leg of the tripod. When the patient bears weight, the ground reaction force pushes up against this rigid first ray, which, through the mechanics of the subtalar joint axis, supinates the midfoot and drives the hindfoot into varus. This is the physiological basis for the Coleman block test. By placing the patient's heel and lateral border of the foot on a block while allowing the first metatarsal to drop freely off the edge, we negate the deforming influence of the first ray. If the hindfoot varus corrects to neutral or valgus on the block, the hindfoot deformity is flexible and driven entirely by the forefoot. If the hindfoot remains in varus, the subtalar joint has developed rigid, structural adaptations that will necessitate a calcaneal osteotomy or arthrodesis.
Exhaustive Indications and Contraindications
The decision-making process for cavovarus reconstruction is highly nuanced and must be individualized to the patient's specific pathoanatomy, functional demands, and medical comorbidities. Surgical intervention is generally indicated when conservative measures—such as custom ankle-foot orthoses (AFOs), lateral heel wedges, and physical therapy—fail to alleviate symptoms or halt the progression of the deformity.
Pain is a primary driver for surgery, often manifesting as lateral column overload, recurrent fifth metatarsal stress fractures, or peroneal tendon pathology due to chronic subluxation and over-stretching. Progressive instability, characterized by frequent lateral ankle sprains and a feeling of "giving way," is another strong indication. In patients with progressive neuromuscular disorders, such as CMT, early joint-sparing reconstruction is advocated to rebalance the foot, prevent the development of rigid structural deformities, and delay or eliminate the eventual need for joint-sacrificing arthrodesis.
Contraindications must be carefully weighed to prevent catastrophic postoperative complications. Absolute contraindications include active deep infection, critical limb ischemia that precludes wound healing, and non-ambulatory status where the surgical risks outweigh the functional benefits. Severe, uncontrolled psychiatric illness or documented medical non-compliance are relative contraindications, as the postoperative rehabilitation protocol is lengthy, demanding, and critical to the ultimate success of the procedure.
Furthermore, the presence of an active Charcot neuroarthropathy event in a diabetic patient strictly contraindicates acute deformity correction until the active inflammatory phase has completely coalesced. In patients with profound sensory neuropathy (where protective sensation is entirely lost), joint-sparing osteotomies carry a high risk of subsequent Charcot breakdown; in these specific scenarios, primary arthrodesis with robust internal fixation may be a more prudent, albeit salvage-oriented, surgical choice.
| Category | Indications for Cavovarus Reconstruction | Contraindications for Cavovarus Reconstruction |
|---|---|---|
| Clinical Presentation | Intractable lateral foot pain / overload | Non-ambulatory patient status |
| Biomechanical | Recurrent lateral ankle instability / sprains | Severe, active Charcot neuroarthropathy |
| Pathological | Recurrent 5th metatarsal stress fractures | Active osteomyelitis or deep soft tissue infection |
| Neuromuscular | Progressive deformity in CMT (joint-sparing) | Critical peripheral arterial disease (ischemia) |
| Conservative Failure | Failure of custom AFOs and orthotics | Severe medical non-compliance / inability to follow rehab |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning is the blueprint for surgical success and begins with a rigorous, systematic clinical examination. The flexibility of the deformity must be meticulously mapped. The Silfverskiold test is performed to differentiate between isolated gastrocnemius contracture and combined gastrocnemius-soleus complex tightness; this dictates whether a gastrocnemius recession or a formal Achilles tendon lengthening is required. The Coleman block test, as previously detailed, is mandatory to assess hindfoot flexibility. Forefoot flexibility is assessed by manually elevating the first metatarsal head to see if the midfoot arch reduces. Muscle strength testing of the tibialis anterior, tibialis posterior, peroneals, and extensor hallucis longus (EHL) is documented to plan appropriate tendon transfers.
Radiographic evaluation requires weight-bearing anteroposterior (AP), lateral, and oblique views of the foot, along with a weight-bearing AP of the ankle and a Saltzman hindfoot alignment view. On the lateral radiograph, we scrutinize Meary’s angle (the angle between the longitudinal axis of the talus and the first metatarsal), which is normally 0 degrees but is significantly increased (convex upward) in a cavus foot. The calcaneal pitch angle is typically elevated above 30 degrees. Hibbs angle (the angle between the longitudinal axis of the calcaneus and the first metatarsal) approaches 90 degrees in severe deformity. The AP view often reveals a lack of talonavicular coverage, indicating midfoot adduction. If plain radiographs are equivocal regarding the presence of subtalar or midfoot arthrosis, a fine-cut Computed Tomography (CT) scan is essential to map joint degeneration, which may pivot the surgical plan from osteotomies to arthrodesis.
Templating is performed digitally to quantify the required correction. For a lateralizing calcaneal osteotomy, the amount of lateral translation (typically 10-15 mm) or the size of a closing lateral wedge is estimated to restore the mechanical axis of the hindfoot slightly lateral to the midline of the calcaneal tuberosity. For the first metatarsal, a dorsiflexion closing wedge osteotomy is templated to bring Meary's angle back to neutral.

Patient positioning in the operating room must facilitate seamless access to the medial, lateral, and dorsal aspects of the foot without requiring intraoperative repositioning. The patient is placed supine on the operating table. Crucially, the patient is positioned such that the heel rests just over the distal edge of the bed. This allows for unrestricted, full-arc ankle dorsiflexion and plantarflexion, which is vital for assessing the adequacy of the Achilles release and the tensioning of tendon transfers. A thick bump is placed beneath the ipsilateral hip to internally rotate the lower extremity, bringing the foot perpendicular to the floor. A pneumatic thigh tourniquet is applied over copious padding. The C-arm fluoroscopy unit is draped and brought in from the contralateral side, positioned to easily obtain true AP, lateral, and axial views with minimal manipulation of the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a cavovarus reconstruction is highly modular, addressing the deformity systematically, usually progressing from proximal to distal, and from soft tissue releases to bony corrections, culminating in dynamic tendon transfers.
Soft Tissue Releases: The Foundation of Correction
The procedure typically commences with addressing the posterior equinus contracture. Based on preoperative Silfverskiold testing, either a gastrocnemius recession (Strayer or Baumann technique) or a percutaneous triple hemisection Achilles lengthening (Hoke technique) is performed. For a Strayer procedure, a posteromedial longitudinal incision is made over the musculotendinous junction. The sural nerve is protected laterally. The gastrocnemius aponeurosis is identified and sharply transected transversely, allowing the muscle belly to retract proximally while keeping the underlying soleus fascia intact.
Following the posterior release, the plantar fascia is addressed. A Steindler stripping is often required for rigid cavus. Through a medial incision over the calcaneal tuberosity, the plantar fascia and the origins of the short plantar musculature (abductor hallucis, flexor digitorum brevis, abductor digiti minimi) are sharply elevated off the calcaneus. Extreme caution is exercised to protect the medial calcaneal nerve branches and the lateral plantar nerve, which courses deep to the abductor hallucis.
Hindfoot Correction: Lateralizing Calcaneal Osteotomy
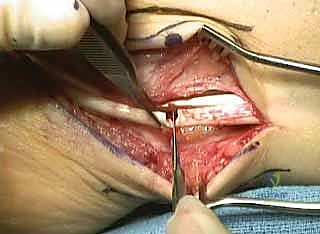
If the Coleman block test demonstrated rigid hindfoot varus, a calcaneal osteotomy is mandatory. A curvilinear lateral incision is made inferior and parallel to the peroneal tendons.
Dissection is carried down carefully through the subcutaneous tissues. The sural nerve is meticulously identified, mobilized, and retracted gently with a vessel loop.

The superior peroneal retinaculum (SPR) and the peroneal tendon sheath are exposed.

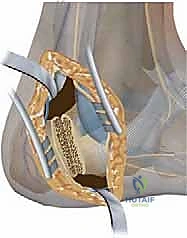
The periosteum over the lateral calcaneal wall is incised, and Hohmann retractors are placed dorsally over the tuberosity and plantarly to protect the neurovascular bundle. An oscillating saw is used to perform an oblique osteotomy, starting posterior to the posterior facet of the subtalar joint and exiting plantarly, anterior to the calcaneal tuberosity.

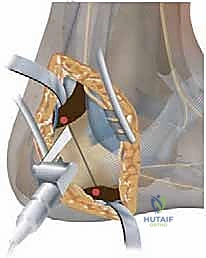
Once the osteotomy is complete, a lamina spreader is inserted to mobilize the tuberosity fragment. The posterior fragment is then translated laterally by 10 to 15 millimeters. In cases of severe structural varus, a laterally based closing wedge (Dwyer osteotomy) may be incorporated into the cut.

The osteotomy is provisionally pinned with Kirschner wires and evaluated under fluoroscopy.

Once alignment is satisfactory, definitive fixation is achieved using two large-fragment (typically 6.5mm or 7.0mm) partially threaded cannulated screws placed from the posterior heel pad, across the osteotomy site, and into the dense bone of the anterior calcaneus.


Forefoot Correction: Dorsiflexion First Metatarsal Osteotomy
Addressing the plantarflexed first ray is the most critical step in preventing recurrence. A dorsal longitudinal incision is made over the proximal first metatarsal, lateral to the EHL tendon. The periosteum is elevated. A dorsally based closing wedge osteotomy is planned approximately 1 to 1.5 cm distal to the first tarsometatarsal (TMT) joint.

Using a microsagittal saw, the wedge of bone is meticulously removed, ensuring the plantar cortex remains intact to act as a hinge.
The osteotomy is closed, dorsiflexing the first ray and effectively flattening the medial longitudinal arch.

Fixation is typically achieved with a low-profile dorsal titanium plate and locking screws, or alternatively, with crossed Kirschner wires or a dorsal staple, depending on surgeon preference and bone quality.


Dynamic Rebalancing: Tendon Transfers
With the structural architecture restored, dynamic muscle balance must be established. The peroneus longus to brevis (PL to PB) transfer is standard. Through the lateral hindfoot incision, the peroneus longus is identified and transected as distally as possible.

The proximal stump of the peroneus longus is then tenodesed to the peroneus brevis tendon using a Pulvertaft weave or side-to-side anastomosis with non-absorbable suture, tensioned with the foot held in neutral dorsiflexion and slight eversion.

For toe clawing and further elevation of the first ray, a Jones procedure is often performed. The EHL tendon is transected at the interphalangeal joint of the hallux. The distal stump is tenodesed to the extensor hallucis brevis to prevent a drop toe.

The proximal EHL tendon is routed through a drill hole in the first metatarsal neck from medial to lateral, and sutured back onto itself under tension with the ankle in neutral.


If lesser toe clawing is severe, a Hibbs procedure (transfer of the extensor digitorum longus to the lateral cuneiform) or Girdlestone-Taylor flexor-to-extensor transfers may be incorporated.

Meticulous layered closure is performed, ensuring the extensor retinaculum and superior peroneal retinaculum are securely repaired to prevent tendon bowstringing or subluxation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, cavovarus reconstruction carries a distinct complication profile due to the extensive soft tissue dissection and multiple osteotomies required. The most frequent neurological complication is injury to the sural nerve, occurring in approximately 5-10% of cases involving lateral calcaneal osteotomies. This can range from transient neurapraxia due to retraction, to permanent numbness or the development of a painful neuroma if the nerve is lacerated. Management of
