DEFINITION
Wrist arthritis occurs when the codependent joints of the wrist lose the ability to rotate normally around one another, thereby impairing wrist kinematics.Wrist arthritis can originate from many causes including osteoarthritis, degenerative arthritis, and inflammatory arthritis.Although sacrificing motion at the wrist, arthrodesis has been shown to reliably relieve pain.
ANATOMY
The wrist is perhaps the most complex set of joints in the body.The eight bones of the wrist work together to provide motion in multiple planes, governed by the complex array of soft tissue ligaments that unite them.Single ligament disruptions can cause degenerative change in nonadjacent bones and at times unlikely sites.Untreated fractures can lead to malunions or nonunions that can disrupt the delicate balance of the wrist.In broad terms, the wrist is divided into two distinct rows of bones.The distal row, including the trapezium, trapezoid, capitate, and hamate, is united to the hand and shows little gross motion relative to the metacarpals.As such, the most significant articulations in the wrist occur in the proximal row bones, which are the scaphoid, lunate, and triquetrum. These proximal row bones allow the wrist to flex, extend, deviate both radially and ulnarly, and pronosupinate.
PATHOGENESIS
Because of the many possible routes to the eventual destruction of the wrist joint, it is difficult to describe a single chain of events that leads to end-stage arthritis, most suitably treated by complete wrist fusion.
NATURAL HISTORY
Causes of wrist degeneration and the often-predictable pattern and pace of wear are detailed in other chapters.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients describe pain and stiffness as their major reasons for presentation. Pain limits their function and their strength.Most patients are less concerned with motion loss if their dominant extremity is not involved. Wrist flexionand extension is typically more involved than supination and pronation.If their dominant wrist is involved, patients prefer to preserve some motion even if faced with low-grade persistent pain after treatment. In this clinical setting, complete wrist fusions are less often performed as the index operation.Physical examination findings may include deformity, tenderness, soft tissue swelling, loss of motion, instability, and pain with motion. Pinch and grip strength are reduced compared with age-matched peers and the uninvolved contralateral extremity.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Wrist arthritis is best studied with standard posteroanterior and lateral radiographs of the wrist.These images often reveal the cause of the degeneration together with its pattern and progression. Special attention is paid to the alignment of the wrist and the bone stock available for fusion and fixation.Computed tomography helps plan limited fusions or salvage procedures when arthritis may have spared areas of the midcarpal or proximal carpal rows.
DIFFERENTIAL DIAGNOSIS
Limited wrist arthritisExtrinsic joint contracture (including calcific tendinitis)Inflammatory arthritis and synovitis (ie, rheumatoid, gout, or pseudogout) InfectionPosttraumatic changes Connective tissue diseases
NONOPERATIVE MANAGEMENT
In most every case, the first form of treatment for wrist arthritis is nonoperative:Nonsteroidal anti-inflammatory medications (NSAIDs)Disease-modifying medications (if the cause of the degenerative process can be identified and is appropriate)SplintingA custom-made thumb spica splint allows interphalangeal motion of the thumb but limits painful wrist motion.A padded glove (similar to weight lifting or cycling glove) helps decrease the load across the wrist and the motion necessary for a satisfactory grip.Narcotics should be avoided as addiction, dependency, and diversion may occur.P.993Local steroid injections placed in the wristThese should be placed with a sterile technique and can be repeated as needed if the joint is destroyed and limited salvage options are available.
SURGICAL MANAGEMENT
Alternative motion-sparing procedures, including partial wrist fusions and proximal row carpectomy, should be considered before performing a complete wrist fusion, especially in patients who have at least 60 degrees of wrist flexion-extension and have isolated articular degeneration.Wrist arthroplasty remains in its infancy and is associated with high revision rates and frequent implant design changes.Wrist arthrodesis after arthroplasty is more difficult due to bone stock loss.Wrist arthrodesis is the final treatment method for end-stage wrist degeneration due to multiple causes or as a salvage procedure in patients who have failed the more limited procedures mentioned earlier.Arthrodesis can be obtained reliably and provides a stable wrist in a high-demand patient.1,2,13,15In patients who have undergone lower extremity joint replacements and therefore require support for ambulation, fusion of the wrist is generally regarded as a reliable procedure.The two most popular methods used to fuse a wrist are plate osteosynthesis and rod osteosynthesis.2,8,15 A new locked intramedullary rod has been proposed to limit dorsal plate prominence.10The chief considerations when choosing between these two options are the desired position of fusion, the quality of the bone and available soft tissue coverage, and the possibility of future infection.The strongest grip is achieved when the wrist is fused in 20 to 30 degrees of extension. Advocates of fusion in this position favor the use of a plate and screw construct that is fabricated to reproduce thisposition.2,4,16 Straight wrist fusion plates are also available, and all these devices include screws and plates that match the size of the radius and the metacarpal.A neutral wrist position obtained with rod osteosynthesis may be more favorable for activities of daily living, including perineal care.2,3,5,13Plate and screw constructs rely on solid screw purchase and stable soft tissue coverage. If good-quality bone and viable soft tissues are not present, as might be the case in a patient with severe rheumatoid disease, intramedullary rod fixation may be a more effective means of fixation.In patients taking aggressive disease-remitting medications, the possibility of late infection should be considered. These patients may benefit from metal removal, which is often more easily accomplished after rod osteosynthesis.
PREOPERATIVE PLANNING
Patients should be assessed for comorbidities including first carpometacarpal joint arthritis and carpal tunnel syndrome (CTS). CTS untreated at the time of fusion may worsen acutely and lead to emergency management.Although the use of aspirin may be continued, clopidogrel (Plavix) should be discontinued to avoid bleeding and flap complications. Warfarin (Coumadin) may be continued if the international normalized ratio (INR) is kept low in the 2 to 2.5 range. The continued use of diseasemodifying medicines may be continued at thesurgeon's discretion.12Radiographs should be reviewed before performing a wrist arthrodesis. Specific attention should be paid tothe amount of available bone stock and the bony alignment. Special plates may need to be ordered if prior surgeries have been performed on the radius.Intraoperative evaluation will require a fluoroscopic device. Appropriate alignment, reduction, screw length, and implant length should be confirmed before closure.
POSITIONING
Patients are placed supine with the operative hand extended on a hand table extension. A tourniquet is applied to the proximal arm over padding.Before anesthesia is induced, the patient's comfortable shoulder position should be assessed. The arm board should not place the shoulder above this position. This test is especially important in rheumatoid patients with limited joint mobility.
APPROACH
Both arthrodesis procedures are performed through a standard dorsal approach to the wrist.11,14,15,16 A longitudinal midline dorsal incision ulnar to the tubercle of Lister is used.The extensor pollicis longus tendon is released from its sheath and retracted radially.11,14The fourth extensor compartment is subperiosteally elevated from the dorsum of the distal radius and retracted ulnarly.The posterior interosseous nerve can be dissected free and excised for pain relief.The dorsal capsule is incised in line with the skin incision and elevated off the carpus.14This exposure allows for performance of concomitant procedures such as a distal ulna excision and dorsal tenosynovectomy.P.994
TECHNIQUES
PLATE AND SCREW OSTEOSYNTHESIS

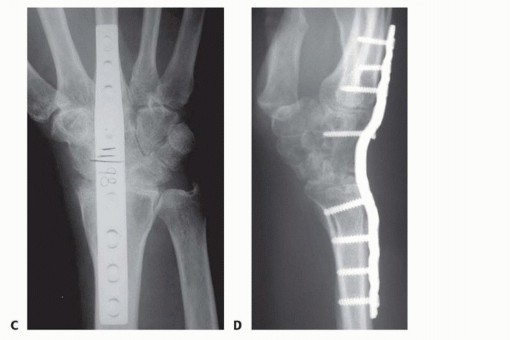


TECH FIG 2 • A,B. Complex wrist collapse secondary to rheumatoid arthritis treated with an intramedullary rod and wiring. Ulnar impaction symptoms developing at the distal radioulnar joint. C,D. Less severe wrist disease in a different patient was treated with a Darrach resection and wrist arthrodesis.(continued)

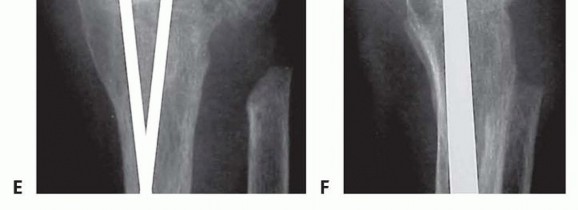
TECH FIG 2 •(continued)E,F. PA and lateral radiographs after wrist arthrodesis in a different patient with rheumatoid arthritis was undertaken using two Steinmann pins inserted through the second and third and third and fourth intermetacarpal spaces. (A-D: Courtesy of P.J. Stern, MD; E,F: Copyright Thomas R. Hunt III, MD.)
PEARLS AND PITFALLS
The third metacarpal should be aligned with the radius. This alignment is essential when applying a plate.Patients prefer to be in slight wrist extension without significant radial or ulnar deviation; significant deviation into flexion or radial deviation leads to problems and weakness. Patients already stiff at neutral may prefer a neutral position.Bilateral fusions may not be preferred but rarely affect function.2If the proximal row has displaced, proximal row carpectomy and fusion has been shown to be successful.4If the ulnar head appears arthritic or prominent, it will need to be addressed using a Darrach procedure, hemiresection techniques, or head replacement. If not addressed, it may be a source of pain postoperatively.If a locked plate design is used due to osteoporosis, one should place the first metacarpal and radius screws as nonlocking screws to pull the plate to the bones.
POSTOPERATIVE CARE
Patients are placed into a removable brace 2 weeks after surgery and started on active finger flexion-extension exercises as well as pronation and supination.Osteoporotic patients may benefit from the short-term use of a thumb spica cast before being advanced into a splint.Patients with an extensor lag due to dorsal swelling are started on a program of dynamic extension with an outrigger splint until full active extension is regained.Strengthening is initiated when motion is recovered and the radiographs demonstrate union. Union usually takes 6 to 8 weeks but is prolonged in smokers. Comorbidities may also affect healing rates. Bone stimulation devices (ultrasound) may be of benefit to accelerate healing especially in at-risk patient populations.If patient compliance is an issue, a cast may be used for the first 4 weeks to protect the plate construct.A cast is recommended for 4 to 6 weeks when using Steinmann rods until the patient's wrist is nontender on examination indicating healing.Therapy may also need to be modified depending on any additional procedures performed.
COMPLICATIONS
InfectionNonunion, delayed union, and malunionDorsal wrist tenderness Tendon adhesions and rupturesNeuromas and complex regional pain syndromes Pin migrationWound breakdown
OUTCOMES
Wrist arthrodesis boasts a high fusion rate, a high satisfaction rate, and a low complication rate.1,5,7,8,9,15 It is for this reason that fusion of the wrist is selected in patients who can tolerate fewer trips to the operating room for secondary procedures.Although more satisfying than rod stabilization in rheumatoid patients (74% vs. 37%), plate fixation mayrequire tenolysis or plate removal after arthrodesis.1,13 Satisfaction may be affected by the patient's underlying disease.Houshian and Schrøder6 found that plate removal was common (15%) due to the complications listed earlier but was successful in relieving symptoms.
REFERENCES
- Barbier O, Saels P, Rombouts JJ, et al. Long-term functional results of wrist arthrodesis in rheumatoid arthritis. J Hand Surg Br 1999;24(1):27-31.
- Calundruccio JH. Osteoarthritis of the wrist. In: Trumble TE, ed. Hand Surgery Update 3. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2003:528-529.
- Clendenin MP, Green DP. Arthrodesis of the wrist: complications and their management. J Hand Surg Am 1981;6:253-257.P.997
- Hartigan BJ, Nagle DJ, Foley MJ. Wrist arthrodesis with excision of the proximal carpal bones using the AO/ASIF wrist fusion plate and local bone graft. J Hand Surg Br 2001;26(3):247-251.
- Hayden RJ, Jebson PJ. Wrist arthrodesis. Hand Clin 2005;21:631-640.
- Houshian S, Schrøder HA. Wrist arthrodesis with the AO titanium wrist fusion plate: a consecutive series of 42 cases. J Hand Surg Br 2001;26(4):355-359.
- Jebson PJ, Adams BD. Wrist arthrodesis: review of current techniques. J Am Acad Orthop Surg 2001;9:53-60.
- Krimmer H. Radiocarpal and total wrist arthrodesis. In: Berger RA, Weiss AP, eds. Hand Surgery. Philadelphia: Lippincott Williams & Wilkins, 2004:1319-1337.
- Mack GR, Bosse MJ, Gelberman RH, et al. The natural history of scaphoid non-union. J Bone Joint Surg Am 1984;66(4):504-509.
- Orbay JL, Feliciano E, Orbay C. Locked intramedullary total wrist arthrodesis. J Wrist Surg 2012;1(2):179-184.
- Ruby LK, Stinson J, Belsky MR. The natural history of scaphoid nonunion. A review of fifty-three cases. J Bone Joint Surg Am 1985;67(3): 428-432.
- Thorsness RJ, Hammert WC. Perioperative management of rheumatoid medications. J Hand Surg Am 2012;37(9):1928-1931.
- Toma CD, Machacek P, Bitzan P, et al. Fusion of the wrist in rheumatoid arthritis: a clinical and functional evaluation of two surgical techniques. J Bone Joint Surg Br 2007;89(12):1620-1626.
- Weil C, Ruby LK. The dorsal approach to the wrist revisited. J Hand Surg Am 1986;11(6):911-912.
- Weiss AC, Wiedeman G Jr, Quenzer D, et al. Upper extremity function after wrist arthrodesis. J Hand Surg Am 1995;20(5): 813-817.
- Weiss AP, Hastings H II. Wrist arthrodesis for traumatic conditions: a study of plate and local graft application. J Hand Surg Am 1995;20(1):50-56.
