CLOSED MANIPULATION FOR SHOULDER STIFFNESS
Refractory shoulder stiffness, frequently manifesting as adhesive capsulitis, is characterized by a profound, progressive restriction of both active and passive glenohumeral range of motion. When conservative modalities—including structured physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections—fail to yield clinical improvement after an adequate trial, closed manipulation under anesthesia (MUA) becomes a viable and highly effective intervention.
Biomechanics and Surgical Execution
The primary objective of closed manipulation is the controlled, sequential rupture of the contracted capsuloligamentous complex, particularly targeting the coracohumeral ligament, the rotator interval, and the inferior axillary pouch.
The procedure must be performed with meticulous care to avoid catastrophic iatrogenic complications. The surgeon must utilize short lever arms, stabilizing the scapula firmly against the thoracic wall to isolate glenohumeral motion. The manipulation typically follows a precise sequence:
1. Elevation in the Scapular Plane: To release the inferior capsule.
2. External Rotation at Varying Degrees of Abduction: To release the rotator interval and anterior capsule.
3. Internal Rotation: To release the posterior capsule.
Surgical Warning: Aggressive manipulation utilizing a long lever arm (e.g., grasping the distal forearm or wrist) places the humerus at severe risk for an iatrogenic spiral fracture. Always apply manipulative forces as proximally as possible, ideally at the surgical neck or proximal humerus.
We occasionally obtain intraoperative anteroposterior (AP) and axillary lateral radiographs immediately after the procedure. This is a mandatory safety protocol to definitively rule out periarticular fractures or iatrogenic glenohumeral dislocations that may have occurred during the capsular release.
Postoperative Care and Rehabilitation Protocol
Rehabilitation following closed manipulation is the most critical determinant of long-term success; without it, the rapid recurrence of capsular contracture is inevitable.
To optimize the rehabilitation timeline, we strategically perform manipulations during the earlier part of the week. This scheduling ensures that the patient can initiate aggressive, supervised physical therapy the very next day without the interruption of a weekend.
- Physical Therapy: Supervised physical therapy sessions are mandated daily for at least 2 to 4 weeks post-manipulation. The primary, non-negotiable goal of this rehabilitation phase is the immediate restoration and maintenance of early, full range of motion.
- Orthotic Management: In a subset of patients with severe preoperative stiffness, we recommend the use of an abduction orthosis worn strictly at night for 3 weeks. This positioning places the inferior capsule on stretch, effectively preventing the significant axial pouch adhesions from returning and cross-linking during the vulnerable early inflammatory phase.
CALCIFIC TENDINITIS OF THE ROTATOR CUFF
Calcific tendinitis is a reactive, self-limiting condition characterized by the deposition of calcium hydroxyapatite crystals within the substance of the rotator cuff tendons, most commonly the supraspinatus. Although most patients seek treatment during the acutely painful resorptive phase of the calcification stage, in some individuals, the calcium deposits are merely an incidental radiographic finding or present as a secondary component of subacromial impingement syndrome.
We firmly believe that only patients actively in the resorptive phase should have treatment directed specifically at the calcium deposit itself. For patients in other phases, the clinical focus should follow treatment protocols directed at the primary pathological condition (e.g., subacromial impingement or rotator cuff tendinopathy).
Chronological Progression
Calcific tendinitis follows a definitive, predictable biological progression in most patients. Spontaneous resolution is observed in almost all cases, with the length of time required for complete resorption being the only true variable. The comprehensive three-phase chronology, originally described by Sarkar and Uhthoff, remains the gold standard framework for understanding the pathology and planning appropriate treatment:
- Phase I: Precalcification Stage
In this initial stage, the site of predilection for calcification—frequently an area within the tendon experiencing a diminished blood supply or localized hypoxia (the "critical zone")—undergoes fibrocartilaginous metaplasia. The tenocytes transform into chondrocytes. At this stage, patients are generally asymptomatic, and the condition is undetectable on standard radiographs. - Phase II: Calcification Stage
This stage is subdivided into three distinct biological events:- Phase of Formation: Calcium is actively deposited into matrix vesicles, which are excreted by the cells and coalesce into larger calcium deposits. On gross surgical inspection, the deposits at this time are dry, chalky, and granular. As the matrix vesicles coalesce into larger deposits, the surrounding fibrocartilage is gradually replaced and eroded.
- Resting Phase: The active deposition ceases. The patient enters a resting phase during which clinical pain may be minimal or entirely absent. The radiographic appearance is characteristic: well-marginated, dense, and mature-appearing deposits. This resting phase is of variable length and ends abruptly with the onset of resorption.
- Resorptive Phase: This is the most clinically significant phase. Vascular channels rapidly appear at the periphery of the deposit, bringing macrophages and multinucleated giant cells to phagocytize the calcium. This stage can be exceedingly painful due to the intense inflammatory response and increased intratendinous pressure. Many patients present to the emergency department or clinic at this time. The calcium deposits undergo a morphological change, resembling thick cream or toothpaste. As the calcium is actively resorbed, the resulting dead space within the tendon is filled with vascular granulation tissue.
- Phase III: Postcalcification Phase
During this final healing phase, the granulation tissue matures into organized collagen. Fibroblasts align the new collagen along the mechanical stress lines parallel to the longitudinal axis of the tendon, effectively reconstituting the tendon's structural integrity. Pain subsides markedly during this phase as the inflammatory cascade resolves.
Nonoperative Management
As noted previously, essentially all patients eventually recover from calcific tendinitis, making nonoperative management the definitive initial treatment of choice. Standard nonoperative treatment usually includes:
* Activity modification and physical therapy.
* Targeted rotator cuff and periscapular exercises.
* Anti-inflammatory medications (NSAIDs).
* Subacromial steroid injections.
Clinical Pearl: While corticosteroids provide profound short-term pain relief, they have been suggested to prematurely abort the resorptive phase. By suppressing the macrophage-mediated inflammatory response, corticosteroids may return the lesion to a state of dormancy, effectively setting into motion the biological factors necessary for future recurrence.
Alternative nonoperative modalities have gained traction. An ultrasound-guided percutaneous needling technique (barbotage), used in conjunction with a subacromial corticosteroid injection, has been reported to be successful in approximately 70% of patients. Furthermore, Extracorporeal Shock Wave Therapy (ESWT) has been advocated for the treatment of calcific tendinitis. Several comparative studies have reported greater pain relief with ESWT than with placebo or sham treatments; however, it is notable that in one major study, half of the patients treated with ESWT eventually required surgical intervention.
Long-term follow-up studies have unequivocally confirmed the benign natural history of this disorder. Although surgically or procedurally treated patients tend to have superior clinical results in the short-term (at 1-year follow-up), at longer-term follow-up (5+ years), there are no statistically significant differences in functional outcomes between operative and nonoperative cohorts.
Surgical Treatment
When conservative measures fail, surgical intervention is warranted. Gschwend et al. listed the following strict indications for operative treatment:
1. Unrelenting symptom progression.
2. Constant, severe pain that actively interferes with activities of daily living (ADLs) and sleep.
3. Complete absence of clinical improvement after a dedicated course of conservative therapy.

FIGURE 46-13 A: Preoperative AP radiograph demonstrating a large, dense, well-marginated calcium deposit within the supraspinatus tendon, characteristic of the resting phase prior to acute resorption.
Currently, we prefer an all-arthroscopic technique when surgery is warranted. The patient is positioned in either the beach-chair or lateral decubitus position. Following a standard diagnostic arthroscopy, the subacromial space is entered.
Localization of the calcific deposit can sometimes be challenging if it is entirely intratendinous. Some authors have reported high success rates using intraoperative ultrasound to identify deposits that are not readily visible on the bursal surface. Alternatively, a spinal needle can be used to systematically puncture the tendon; the extrusion of "toothpaste-like" material confirms the location.
Once localized, the removal of calcium deposits is performed meticulously with a mechanical shaver or a curette. The goal is decompression and evacuation of the deposit without excessively violating the structural integrity of the rotator cuff.
Acromioplasty is performed concurrently for patients with definitive preoperative or intraoperative evidence of subacromial stenosis or mechanical impingement. Several authors have reported good to excellent results in approximately 90% of patients undergoing arthroscopic removal of calcific deposits. The absolute necessity of a routine acromioplasty, as well as the clinical significance of leaving residual micro-calcifications on postoperative radiographs, remains a subject of ongoing debate in the literature.
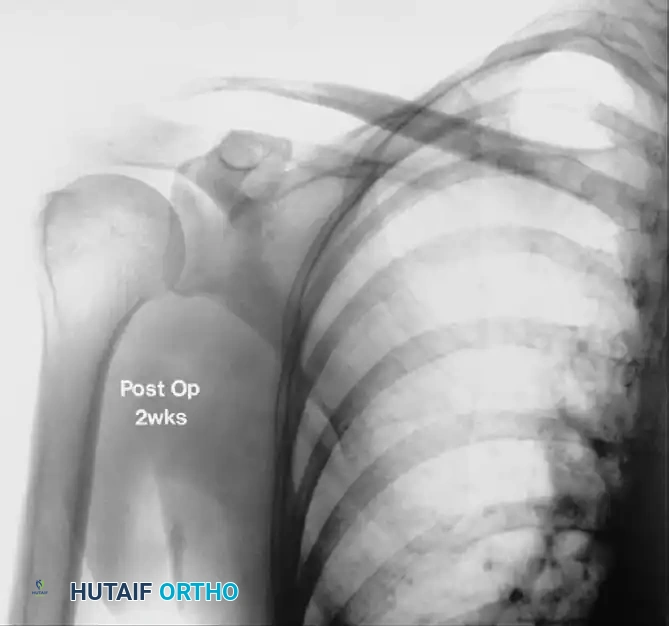
FIGURE 46-13 B: Radiograph taken 2 weeks after arthroscopic excision, demonstrating complete resolution of the calcific deposit and restoration of the subacromial interval.
QUADRILATERAL SPACE SYNDROME
Quadrilateral space syndrome (QSS) is an uncommon but clinically significant neurovascular entrapment syndrome. It involves the dynamic compression of the axillary nerve and the posterior humeral circumflex artery as they traverse the quadrilateral space.
The quadrilateral space is anatomically bounded by the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially, and the surgical neck of the humerus laterally.
Pathoanatomy and Clinical Presentation
The hallmark of QSS is dynamic compression. Angiographic and MRI studies frequently demonstrate a patent posterior humeral circumflex artery with the arm resting at the side. However, when the arm is placed in the ABER position (Abduction and External Rotation), the artery and nerve become acutely compressed.
The lesion typically consists of anomalous, oblique fibrous bands that traverse the space, acting as a tethering mechanism that compresses the axillary nerve and artery against the muscular borders when the shoulder is in abduction and external rotation. Occasionally, a paralabral cyst originating from a posterior labral tear may extend into the quadrilateral space, causing direct mass-effect compression of the nerve.
Patients typically present with poorly localized posterior shoulder pain, paresthesias in the lateral arm (over the deltoid insertion), and perceived weakness, particularly exacerbated by overhead activities or throwing motions.
Management Protocol
Nonoperative treatment is universally indicated initially for all patients presenting with QSS. This regimen includes:
* Strict activity modification (avoidance of repetitive ABER positioning).
* NSAIDs to reduce localized inflammation.
* Targeted cortisone injections into the quadrilateral space (often ultrasound-guided).
* Comprehensive physical therapy focusing on rotator cuff muscle strengthening and periscapular stabilization.
If debilitating symptoms persist after 3 to 6 months of compliant nonoperative treatment, surgical decompression is indicated.
Surgical Approach:
Surgical decompression is traditionally performed through a posterior approach. The patient is placed in the lateral decubitus position. An incision is made parallel to the posterior border of the deltoid. The interval between the teres minor and teres major is identified and bluntly developed.
Careful dissection reveals the axillary nerve and posterior humeral circumflex artery. The offending oblique fibrous bands are meticulously lysed, freeing the neurovascular bundle. If a paralabral cyst is identified as the compressive etiology, it must be decompressed, and the underlying posterior labral pathology should be addressed, often requiring a concurrent or staged arthroscopic labral repair. Lysis of these fibrous bands through a posterior approach consistently yields good to excellent results, with a high rate of return to pre-injury activity levels and resolution of neurovascular symptoms.
