CLINICAL PRESENTATION AND DIAGNOSTIC CHALLENGES
The evaluation of a painful shoulder remains one of the most formidable diagnostic challenges in orthopedic surgery. The complexity arises from the anatomical density of the shoulder girdle, where multiple distinct clinical conditions present with strikingly similar histories, pain patterns, and physical examination findings. Pathologies such as various subacromial impingement syndromes, partial or complete rotator cuff tears, calcific tendinitis, adhesive capsulitis, and subtle nerve entrapment syndromes frequently mimic one another.
All of these conditions can precipitate a triad of symptoms: pain, subjective or objective weakness, and a loss of motion in the affected extremity. The pain is classically exacerbated by overhead activities, is typically worse with active rather than passive motion, and frequently awakens the patient from sleep—a hallmark of rotator cuff pathology. Pain is often referred to the lateral aspect of the arm near the deltoid insertion, rather than the joint itself.
Clinical Pearl: On physical examination, it is often impossible to reliably establish which specific structure is the primary pain generator based solely on palpation. The close anatomical proximity of the coracoacromial arch, the rotator cuff footprint, and the capsulolabral complex confounds precise localization.
Furthermore, while many provocative tests are highly sensitive for detecting shoulder pathology, they notoriously lack specificity. Multiple conditions can elicit pain during the same provocative maneuver. Palpation is of limited diagnostic benefit, particularly in muscular or obese patients. It is anatomically impossible to directly palpate the glenoid labrum or the deep articular capsule. While some authors claim the ability to palpate specific rotator cuff tears through the deltoid, this is highly subjective and generally unreliable. Similarly, clicks and crepitus within the shoulder are non-specific; the reverberating quality of these mechanical sounds makes them unreliable for precise anatomical localization.
Despite these limitations, a meticulous physical examination is an indispensable component of the patient evaluation. Crucially, it serves to eliminate other potential sources of referred pain.
Surgical Warning: Always rule out extrinsic sources of shoulder pain. Disorders of the cervical spine (herniated disc, cervical spondylosis, brachial plexopathy), the chest cavity (Pancoast tumor, upper lobe pneumonia), the axillary area, and the abdomen (diaphragmatic irritation, gallbladder dysfunction) can all present as primary shoulder pain.
THE SYSTEMATIC PHYSICAL EXAMINATION
The physical examination must follow a strict, systematic algorithm beginning with inspection. Proper exposure is mandatory; the patient should be undressed above the waist (women may utilize a strapless gown to allow full visualization of the shoulder girdle).
Inspection and Palpation
Observation of both the anterior and posterior aspects of the shoulder is critical. Bilateral comparison may reveal subtle supraspinatus or infraspinatus atrophy (indicative of chronic rotator cuff tearing or suprascapular neuropathy), swelling, or structural deformity (such as an acromioclavicular joint step-off). Ecchymosis may suggest acute trauma, such as a contusion or a rupture of the rotator cuff or the long head of the biceps tendon.
Palpation of superficial bony landmarks may identify localized pathology at the acromioclavicular joint, sternoclavicular joint, clavicle, or acromion. While palpation of the soft tissues is less specific, examining the joints above and below the affected area is mandatory. For the shoulder, the "joint above" is the cervical spine, which must be cleared via Spurling's maneuver and a thorough neurologic assessment. A comprehensive neurovascular examination of both upper extremities, including an assessment of motor strength and dermatomal sensation, is required.
Range of Motion (ROM)
Range of motion must be determined both actively and passively. The examiner should carefully note the presence of painful arcs (typically between 60 and 120 degrees of abduction) and any tendencies to substitute muscle function, such as utilizing scapulothoracic shrugging to compensate for glenohumeral stiffness or rotator cuff insufficiency.
PROVOCATIVE TESTS FOR IMPINGEMENT AND TENDINITIS
Several provocative maneuvers have been popularized for detecting tendinitis and tears of the rotator cuff. These tests are biomechanically designed to either reproduce the patient's symptoms or produce localized pain suggesting impingement of the rotator cuff against the coracoacromial arch.
Neer Impingement Sign and Test
Charles Neer first described the impingement sign in 1972.
Execution: With the patient seated, the examiner stabilizes the scapula to prevent upward rotation. The examiner then raises the affected arm in forced forward elevation.

Biomechanics: This maneuver forcibly drives the greater tuberosity of the humerus against the anteroinferior surface of the acromion and the coracoacromial ligament.
This test produces pain in impingement lesions of all stages. However, it is highly non-specific and will produce pain in conditions such as adhesive capsulitis, glenohumeral osteoarthritis, calcific tendinitis, and occult bone lesions.
The Neer Injection Test: Neer also described an adjunctive test utilizing a subacromial injection of 10 mL of 1% lidocaine. If the pain is caused by true subacromial impingement, the pain is significantly reduced or eliminated post-injection. Pain caused by other conditions (with the exception of calcific tendinitis) typically remains unrelieved.
Statistical Reliability: Studies reveal a sensitivity for the Neer sign of 75% for bursitis and 88% for cuff abnormalities, but specificities are low (48% and 51%, respectively). The test is also positive in 25% of patients with Bankart lesions, 46% with SLAP lesions, and 69% with acromioclavicular arthritis.
Hawkins-Kennedy Test
Described in 1980 as an alternative to the Neer test, Hawkins and Kennedy designed this maneuver to aggressively compress the subacromial space.
Execution: The test is performed by forward flexing the humerus to 90 degrees in the sagittal plane, followed by forcible internal rotation of the shoulder by the examiner.

Biomechanics: This maneuver drives the greater tuberosity farther under the rigid coracoacromial ligament, reliably reproducing impingement pain.
Statistical Reliability: Sensitivities of 92% for bursitis and 88% for cuff abnormalities have been reported, with specificities of 44% and 43%. Like the Neer test, it is frequently positive in concurrent pathologies: 31% in Bankart lesions, 69% in SLAP lesions, and 94% in AC joint arthritis.
Jobe (Supraspinatus) Test
Described by Frank Jobe in 1983, this test isolates the supraspinatus muscle.
Execution: The shoulder is placed in 90 degrees of abduction and 30 degrees of forward flexion (the scapular plane). The arm is then internally rotated so that the thumb points toward the floor (the "empty can" position). The examiner applies downward resistance.

Interpretation: Weakness or insufficiency against resistance indicates a structural tear of the supraspinatus, whereas pain without profound weakness suggests tendinopathy or impingement.
Internal Rotation Resistance Stress Test (IRRST)
Zaslav described this test to differentiate between internal (posterosuperior) impingement and classic outlet (subacromial) impingement.
Execution: The patient is seated, and the examiner stands behind them. The arm is positioned in 90 degrees of coronal abduction and approximately 80 degrees of external rotation. A manual isometric muscle test is performed for external rotation and then compared with internal rotation in the exact same position.
Interpretation: If a patient with a positive impingement sign demonstrates good strength in external rotation but weakness in internal rotation, the test is positive for internal impingement. Conversely, more weakness in external rotation suggests classic outlet impingement. Zaslav reported a sensitivity of 88% and a specificity of 96% for this specific differentiation.
Gerber Subcoracoid Impingement Test
Designed to identify atypical impingement between the anterior rotator cuff and the coracoid process.
Execution: The arm is forward flexed to 90 degrees and adducted 10 to 20 degrees across the body. The examiner then internally rotates the arm.

Biomechanics: This brings the lesser tuberosity into direct contact with the coracoid process. Pain indicates coracoid impingement, often associated with subscapularis pathology.
Jobe Apprehension-Relocation Test
Described in 1989, this combination test distinguishes primary impingement from secondary impingement caused by subtle anterior glenohumeral instability.
Execution: With the patient supine, the arm is abducted to 90 degrees and externally rotated, which typically produces pain. The examiner then applies a posteriorly directed force to the proximal humerus (relocating the humeral head into the glenoid).
Interpretation: If the posterior force relieves the pain and allows greater external rotation, the primary pathology is anterior instability (secondary impingement). If the pain remains unchanged, it suggests primary subacromial impingement.
Speed Test
Described by Crenshaw and Kilgore in 1966, this test evaluates the long head of the biceps tendon.
Execution: The patient forward flexes the shoulder to 90 degrees with the elbow fully extended and the forearm supinated. The examiner applies downward resistance to the forearm.

Interpretation: A positive result produces pain localized precisely to the bicipital groove. While historically used for biceps tendinitis, it is also frequently positive in SLAP lesions. Sensitivity is reported around 38-90%, with highly variable specificity.
Yergason Sign
Described in 1931, this is another classic test for biceps pathology.
Execution: The elbow is flexed to 90 degrees, and the forearm is pronated. The patient attempts to actively supinate the forearm against the examiner's resistance at the wrist.

Interpretation: Pain localized to the bicipital groove indicates inflammation or instability of the long head of the biceps tendon. Yergason originally noted that this test may be negative in the presence of a complete supraspinatus rupture.
CLINICAL TESTS FOR ROTATOR CUFF INTEGRITY
The following tests are explicitly designed to assess the structural integrity of the rotator cuff tendons. They fall into two categories: active movement tests and passive position maintenance tests (lag signs).
Diagnostic Pitfall: During the examination of a painful shoulder, it can be exceedingly difficult to determine if weakness is due to pain inhibition or a true structural tendon tear. Weakness accompanied by severe pain should be interpreted with caution and does not automatically confirm a full-thickness tear. True structural failure is best demonstrated by painless weakness or a positive "lag" sign.
Lift-Off Test (Subscapularis)
Described by Gerber and Krushell in 1991, this test detects isolated ruptures of the subscapularis tendon.
Execution: With the patient seated or standing, the arm is internally rotated, and the dorsum of the hand is placed against the mid-lumbar spine. The patient is asked to actively lift the hand away from the back.

Interpretation: Inability to lift the hand off the back constitutes a positive test. Electromyography confirms that the subscapularis is maximally active in this mid-lumbar position.
Belly Press Test (Subscapularis)
Gerber et al. developed this alternative for patients who lack the internal rotation required to reach their lumbar spine for the Lift-Off test.
Execution: The patient presses the palm of their hand flat against their abdomen and attempts to bring the elbow forward (maximal internal rotation).

Interpretation: If the subscapularis is intact, the elbow remains in front of the trunk. If the tendon is torn, the patient cannot maintain internal rotation; the elbow drops backward behind the trunk, and the patient compensates by extending the shoulder and flexing the wrist to maintain abdominal pressure.
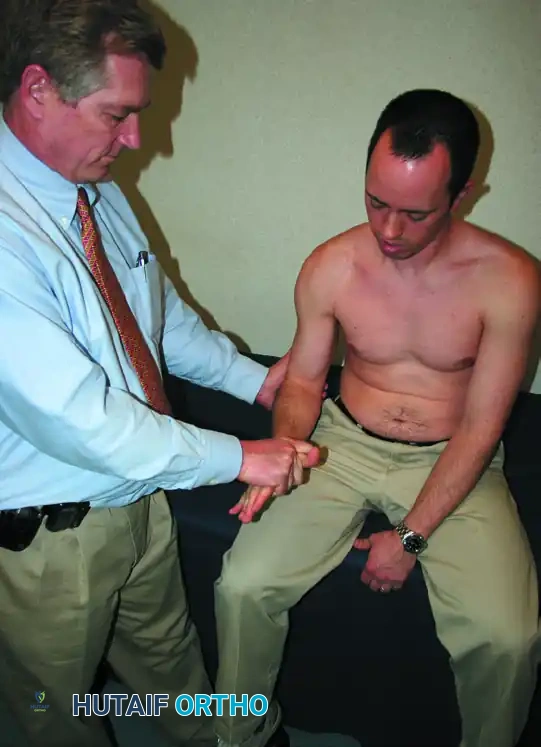
External Rotation Stress Test (Infraspinatus / Teres Minor)
This test evaluates the integrity of the posterior rotator cuff.
Execution: The patient's arms are held at their sides in neutral flexion/abduction, with the elbows flexed to 90 degrees. The shoulders are passively externally rotated 45 to 60 degrees. The examiner applies inward force against the dorsum of the hands while the patient resists.

Interpretation: Pain and yielding weakness suggest inflammation or tearing of the infraspinatus and/or teres minor.
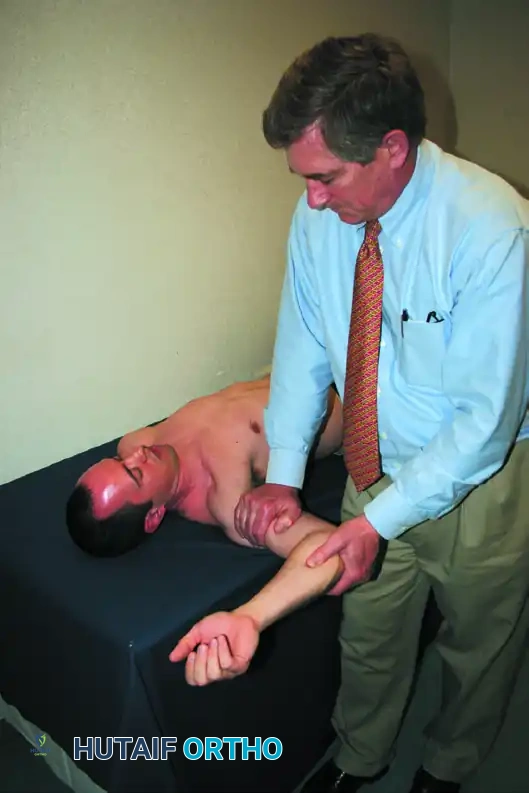
External Rotation Lag Sign
This is a highly specific test for structural failure of the supraspinatus and infraspinatus tendons.
Execution: The patient is seated with their back to the examiner. The examiner passively places the affected arm into maximal external rotation (with the elbow flexed to 90 degrees and the arm slightly abducted). The patient is then asked to actively maintain this position as the examiner releases the wrist.

Interpretation: If the arm "lags" or drifts back into internal rotation, the test is positive, indicating a significant structural defect in the external rotators (infraspinatus/teres minor) that cannot be attributed merely to pain inhibition.
EVIDENCE-BASED DIAGNOSTIC ACCURACY
Relying on a single clinical test is fraught with diagnostic error. Park et al. evaluated eight common impingement tests in a cohort of 552 patients to determine cumulative diagnostic accuracy.
Their landmark findings demonstrated that clinical tests are most powerful when clustered:
* If the Hawkins-Kennedy sign, the Painful Arc sign, and the Jobe (Supraspinatus) test are all positive, the likelihood of the patient having a clinically significant impingement syndrome is greater than 95%.
* Conversely, if all three of these tests are negative, the likelihood of impingement syndrome drops to less than 24%.
Understanding the statistical weight of these physical examination maneuvers allows the orthopedic surgeon to transition from a broad differential diagnosis to a targeted, evidence-based treatment pathway, optimizing the use of advanced imaging (MRI/Ultrasound) and surgical intervention.
