INTRODUCTION AND PATHOANATOMY
Hammer toe deformity is a complex, progressive structural abnormality of the lesser toes characterized primarily by a flexion contracture at the proximal interphalangeal (PIP) joint. As the deformity advances, it is frequently accompanied by a secondary extension contracture or subluxation at the metatarsophalangeal (MTP) joint, and occasionally a compensatory hyperextension at the distal interphalangeal (DIP) joint.
The pathoanatomy is rooted in a dynamic imbalance between the extrinsic musculature (extensor digitorum longus [EDL] and flexor digitorum longus [FDL]) and the intrinsic musculature (lumbricals and interossei). When the MTP joint is forced into prolonged extension—often due to restrictive footwear, pes cavus, or neuromuscular disorders—the intrinsic muscles lose their mechanical advantage to flex the MTP and extend the PIP joints. Consequently, the FDL overpowers the extensor mechanism at the PIP joint, leading to the classic hammer toe posture.
CLINICAL FINDINGS AND EVALUATION
A meticulous clinical examination is paramount for staging the deformity and formulating an appropriate surgical plan. The evaluation must differentiate between flexible, semi-rigid, and rigid deformities, as this dictates the necessity of soft tissue versus osseous procedures.
Three distinct anatomical zones are highly susceptible to painful pressure and hyperkeratotic lesions in the presence of a hammer toe deformity:
- The Dorsum of the PIP Joint: This is the most common site of symptomatic presentation. A hard corn (heloma durum) develops secondary to repetitive shear and compressive forces against the toe box or vamp of the shoe.
- The Distal Tuft (End-Bearing Posture): When a severe flexion posture of the PIP joint forces the DIP joint into an end-bearing position, a painful callus (end corn) develops just plantar to the nail bed.
- The Plantar Metatarsal Head: If the proximal phalanx subluxates dorsally at the MTP joint, the plantar fat pad is drawn distally. This exposes the plantar aspect of the metatarsal head to increased weight-bearing forces, resulting in a painful plantar intractable plantar keratosis (IPK) or transfer metatarsalgia.
Furthermore, the dorsofibular aspect of the second MTP joint is frequently tender to palpation. This tenderness is a clinical hallmark of early plantar plate attenuation or collateral ligament insufficiency, often preceding frank crossover toe deformity.
Clinical Pearl: In patients with compromised sensibility—most notably those with diabetes mellitus, peripheral neuropathy, or myelomeningocele—these focal areas of pressure are highly prone to ulceration. Deep infection, osteomyelitis, and subsequent amputation are severe risks that complicate the treatment plan and endanger the viability of the foot. Prophylactic surgical correction is often indicated in these high-risk populations before ulceration occurs.
CONSERVATIVE MANAGEMENT
Conservative treatment of hammer toe deformities is frequently disappointing in achieving long-term correction, though it remains the first line of defense for mild, flexible deformities or in patients with absolute contraindications to surgery.
Non-operative modalities include extra-depth footwear with a wide toe box, commercially available silicone crest pads, and strapping techniques designed to reduce the deformity and offload prominent pressure points.
If the deformity is of short duration and lacks a fixed extension contracture at the MTP joint, daily manipulation and taping of the toe to prevent MTP extension can occasionally correct the PIP flexion deformity. The biomechanical rationale is that the EDL can only forcefully extend the middle phalanx if the MTP joint is held in neutral or slight flexion. However, recurrence is nearly universal once passive stretching and taping are discontinued. Consequently, the vast majority of patients with symptomatic, progressive hammer toes will eventually require surgical intervention.
SURGICAL INDICATIONS AND ALGORITHM
The fundamental prerequisite for surgical intervention is a symptomatic toe. Cosmetic dissatisfaction alone is an absolute contraindication to surgical correction due to the inherent risks of toe surgery, including stiffness, floating toe, and vascular compromise.
Hammer toe encompasses a broad spectrum of deformities. The indicated procedure is dictated by the flexibility of the joints, the presence of MTP subluxation, and the patient's age and arch morphology.
Treatment Algorithm by Deformity Stage
- Flexible Hammer Toe: No fixed contracture at the MTP or PIP joint. Deformity is primarily dynamic (increases on weight-bearing).
- Treatment: Usually nonoperative. If refractory, a flexor-to-extensor transfer (FDL transfer) is indicated.
- Rigid Hammer Toe (Moderate): Fixed flexion contracture at the PIP joint; no extension contracture at the MTP joint.
- Treatment: Resection of the condyles of the proximal phalanx (head/neck resection) with dermodesis. Percutaneous EDL lengthening or tenotomy if extensor tightness is present.
- Rigid Hammer Toe with MTP Subluxation (Severe): Fixed flexion contracture at the PIP joint; fixed extension contracture or subluxation at the MTP joint.
- Treatment: Proximal phalanx condylectomy, dermodesis, EDL lengthening, EDB tenotomy, MTP dorsal capsulotomy, and collateral ligament sectioning.
- Rigid Hammer Toe with MTP Dislocation / Claw Toe: Fixed PIP flexion, MTP subluxation/dislocation in extension.
- Treatment: All soft tissue releases listed above, plus MTP arthroplasty or distal metatarsal shortening osteotomy (Weil osteotomy).
- Crossover Toe: Fixed PIP flexion, MTP subluxation in varus or valgus.
- Treatment: Proximal phalanx condylectomy, collateral ligament/capsular repair, EDB transfer.
- Mallet Toe: Fixed flexion contracture isolated to the DIP joint.
- Treatment: Resection of the condyles of the middle phalanx, dermodesis, and FDL tenotomy.
SOFT TISSUE PROCEDURES: FLEXOR-TO-EXTENSOR TRANSFER
The use of soft tissue procedures in isolation—without bone shortening or arthrodesis—is reserved for highly specific clinical scenarios. The Girdlestone-Taylor procedure (and its modifications by Parrish, Mann, and Coughlin) involves transferring the FDL to the dorsal extensor hood.
Indications and Patient Selection
A soft tissue procedure is most reliable under the following strict criteria:
1. Skeletally immature foot with a symptomatic flexible hammer toe.
2. Young adult (<30 years old) with a dynamic, flexible deformity that interferes with shoe wear.
3. Normal arch or planovalgus foot morphology (contraindicated in rigid cavus feet).
4. No fixed deformity at the MTP joint (the joint can be passively flexed beyond neutral).
5. No fixed flexion deformity at the PIP joint.
The procedure is based on the biomechanical assumption that the FDL is a primary deforming force. By transferring it dorsally, its plantarflexion force at the PIP is eliminated, and it is converted into a plantarflexor of the MTP joint, restoring the intrinsic-extrinsic balance.
The Boyer and DeOrio Modification
Historically, the FDL transfer was plagued by the "floating toe" complication—a toe that fails to purchase the ground during the stance phase of gait. To mitigate this, Boyer and DeOrio introduced critical technical modifications:
* Incision: Utilizing a longitudinal plantar incision at the MTP joint crease for FDL harvest, rather than a transverse incision.
* Routing: Passing the transferred tendon deep to the dorsal hood rather than superficial to it, improving the mechanical vector.
* Fixation: Utilizing larger (0.54-mm) Kirschner wires for robust temporary fixation and absorbable sutures for the tenodesis.
* Outcomes: This modified technique yields an 89% patient satisfaction rate with a near-zero incidence of floating toe deformities.
BONE AND JOINT PROCEDURES: MODERATE TO SEVERE DEFORMITIES
For rigid deformities, soft tissue balancing alone is insufficient. Osseous shortening is required to decompress the contracted soft tissue envelope and restore alignment. The most commonly utilized procedures include resection arthroplasty of the PIP joint and PIP joint arthrodesis.
Moderate Deformity: PIP Joint Resection Arthroplasty
In a moderate deformity featuring a fixed PIP contracture but a supple MTP joint, resection of the head and neck of the proximal phalanx is the gold standard.
Surgical Technique:
1. Incision: A dorsal elliptical skin incision is made over the PIP joint. The ellipse of skin is excised to perform a simultaneous dermodesis, which aids in maintaining extension postoperatively.
2. Exposure: The extensor tendon is split longitudinally or tenotomized transversely (depending on the need for lengthening). The collateral ligaments of the PIP joint are sharply released.
3. Bone Resection: The PIP joint is acutely flexed to expose the head of the proximal phalanx. A microsaw or bone-cutting forceps is used to resect the head and surgical neck of the proximal phalanx.
4. Assessment: The toe is reduced. If residual extensor tightness exists at the MTP joint, a percutaneous EDL tenotomy is performed with the ankle held in neutral dorsiflexion.
5. Fixation: While some surgeons rely solely on the dermodesis and a bulky soft dressing, temporary stabilization with a 0.045-inch or 0.062-inch Kirschner wire driven antegrade through the middle and distal phalanges, and then retrograde into the proximal phalanx, ensures alignment during the initial healing phase.
Surgical Warning: Resection of only the head of the proximal phalanx (resection arthroplasty) is generally preferred over formal arthrodesis for the 2nd through 5th toes. Patients must be counseled preoperatively that the toe will "mold" to fit comfortably between adjacent toes. Most patients prefer the limited mobility of a pseudoarthrosis over a completely rigid, fused PIP joint, which can be symptomatic in tight footwear.
PIP Joint Arthrodesis
When formal fusion is desired (often in the 2nd toe to provide a buttress for hallux valgus correction), intramedullary fixation is required. Recently, absorbable intramedullary pins have demonstrated excellent outcomes (up to 90% success).
* Advantages: Avoidance of percutaneous pin tract infections, no need for pin removal, less restriction on postoperative activity, and a decreased incidence of floating toe.
* Pitfalls: Surgeons must exercise caution in larger, longer toes, as standard 2-mm absorbable pins may fail to provide adequate biomechanical rigidity, leading to delayed union or hardware failure.
Severe Deformity: Comprehensive MTP and PIP Reconstruction
Severe hammer toes present with a fixed PIP flexion contracture combined with a fixed MTP extension contracture or frank dorsal subluxation. This requires a sequential, stepwise release of the MTP joint in addition to the PIP bone resection.
Stepwise MTP Joint Release:
1. Extensor Lengthening: A Z-lengthening of the EDL tendon is performed.
2. EDB Tenotomy: The extensor digitorum brevis is tenotomized.
3. Dorsal Capsulotomy: A transverse dorsal capsulotomy of the MTP joint is executed.
4. Collateral Ligament Release: If the MTP joint remains extended, the medial and lateral collateral ligaments are sectioned off the metatarsal head.
5. Reduction and Repair: The joint is reduced into a neutral position (both anteroposteriorly and mediolaterally). The EDL is repaired in its lengthened state.
6. Pinning: A longitudinal K-wire is driven across the DIP, PIP, and MTP joints to maintain the reduction.
Management of the Dislocated MTP Joint:
If the MTP joint remains subluxated or dislocated despite aggressive soft tissue release, osseous decompression is mandatory. A Weil osteotomy (distal metatarsal shortening osteotomy) is performed. This osteotomy is cut parallel to the plantar aspect of the foot, allowing the metatarsal head to slide proximally, thereby decompressing the joint and relaxing the intrinsic musculature without depressing the metatarsal head.
ADVANCED TECHNIQUES: PLANTAR PLATE TENODESIS
For flexible hammer toes or early claw toe deformities driven by plantar plate insufficiency, an arthroscopic-assisted or open plantar plate tenodesis is highly effective. As demonstrated by Lui et al., this technique restores the plantar restraint of the MTP joint.
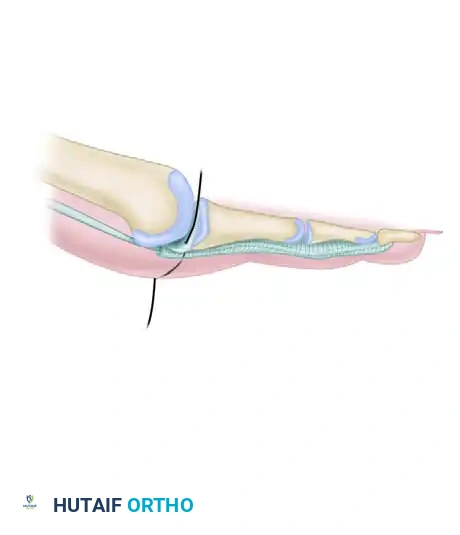
Figure 1: Initial pass of the suture needle through the attenuated plantar plate and plantar capsule. The needle is directed carefully to capture robust tissue without violating the flexor tendon sheath.
The procedure involves passing a heavy, non-absorbable suture through the plantar plate and securing it to the base of the proximal phalanx. This effectively reef the attenuated plantar plate, pulling the proximal phalanx out of its hyperextended posture and restoring the normal MTP joint alignment.
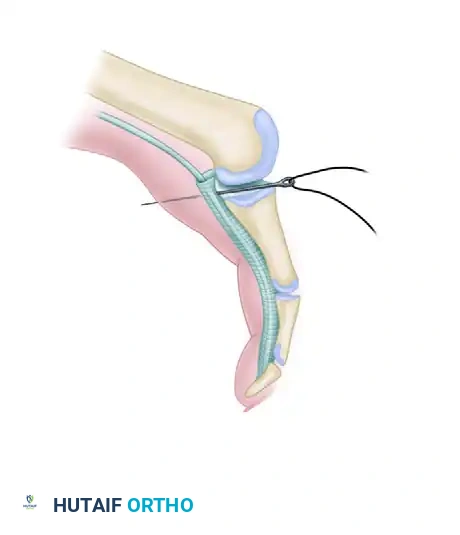
Figure 2: The suture is tensioned and tied dorsally, effectively tenodesing the plantar plate to the proximal phalanx. This maneuver plantarflexes the MTP joint, correcting the dynamic extension deformity.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Postoperative Care
- Dressing: A meticulously applied compressive forefoot dressing is crucial. The dressing must hold the toe in the corrected position, splinting the soft tissues. This dressing is changed weekly as edema subsides.
- Weight-Bearing: Patients are typically allowed heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe immediately following surgery.
- Pin Management: If K-wires are utilized, they are left in place for 3 to 4 weeks for soft tissue procedures and 4 to 6 weeks for arthrodesis. Pin tract care is essential to prevent superficial infections.
Complications and Management
- Vascular Compromise ("White Toe"): The most devastating immediate complication. If a toe is profoundly ischemic after pinning, the K-wire must be removed immediately. The toe should be placed in a dependent position, warmed, and if necessary, treated with topical vasodilators (e.g., papaverine) or sympathetic blocks. Never leave the operating room with a pulseless, white toe.
- Floating Toe: Often results from over-lengthening of the extensor mechanism, excessive metatarsal shortening, or failure to address intrinsic contractures. Prevention via precise surgical technique (e.g., deep routing in FDL transfers) is paramount.
- Recurrence: Usually secondary to under-correction of the MTP joint extension contracture. A thorough stepwise release must be confirmed intraoperatively before final fixation.
- Stiffness: Expected after PIP resection or arthrodesis. Preoperative patient counseling is critical to align postoperative expectations regarding toe mobility.
