Panadol: A Comprehensive Medical SEO Guide to Paracetamol (Acetaminophen)
Welcome to this authoritative guide on Panadol, a widely recognized brand name for the active pharmaceutical ingredient paracetamol, also known as acetaminophen in some regions. As an expert medical SEO copywriter and orthopedic specialist, this guide aims to provide a massive, exhaustive, and highly authoritative resource for patients, caregivers, and healthcare professionals seeking in-depth knowledge about this ubiquitous medication.
Panadol is a cornerstone in pain management and fever reduction globally, renowned for its efficacy and relatively favorable safety profile when used correctly. However, its widespread availability and common usage often lead to underestimation of its potential risks, particularly concerning overdose and liver toxicity. This guide will delve into its technical specifications, clinical applications, safety considerations, and critical management strategies to ensure optimal and safe use.
Disclaimer: This guide provides extensive medical information for educational purposes only and should not be considered a substitute for professional medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider before making any decisions about your health or treatment.
Deep Dive into Panadol's Technical Specifications and Mechanisms
Panadol's effectiveness stems from its unique pharmacological profile, distinguishing it from other common pain relievers.
What is Paracetamol (Acetaminophen)?
Paracetamol (N-acetyl-p-aminophenol, APAP) is an aniline derivative with analgesic (pain-relieving) and antipyretic (fever-reducing) properties. Unlike Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) such as ibuprofen or aspirin, paracetamol exhibits minimal anti-inflammatory activity at standard therapeutic doses and does not share the same mechanism of action or side effect profile, particularly regarding gastric irritation and antiplatelet effects.
Mechanism of Action
The precise mechanism of action of paracetamol is still a subject of ongoing research, but it is primarily understood to exert its effects centrally within the nervous system.
- Central Prostaglandin Inhibition: Paracetamol is believed to selectively inhibit prostaglandin synthesis in the central nervous system (CNS). Prostaglandins are lipid compounds that mediate pain, inflammation, and fever. While NSAIDs inhibit cyclooxygenase (COX) enzymes in both peripheral tissues and the CNS, paracetamol's effect is thought to be more pronounced on central COX enzymes, particularly COX-2 and a theoretical COX-3 isoform. This central action explains its efficacy in reducing pain and fever without significant peripheral anti-inflammatory effects.
- Modulation of Serotonergic Pathways: Some research suggests paracetamol may activate descending serotonergic pathways, which play a role in pain modulation.
- Endocannabinoid System Interaction: There is also evidence indicating that paracetamol's analgesic effect might involve an indirect interaction with the endocannabinoid system, specifically through the activation of cannabinoid CB1 receptors by a metabolite called AM404.
- Thermoregulatory Center: Its antipyretic effect is achieved by acting on the hypothalamus, the part of the brain responsible for regulating body temperature. It helps to reset the body's thermostat, leading to peripheral vasodilation and sweating, which facilitates heat loss and reduces fever.
Pharmacokinetics
Understanding how Panadol is absorbed, distributed, metabolized, and excreted is crucial for appreciating its therapeutic profile and potential for toxicity.
Absorption
- Rate: Rapidly and almost completely absorbed from the gastrointestinal (GI) tract.
- Peak Plasma Concentration: Typically reached within 30 to 60 minutes after oral administration, although this can vary slightly with different formulations (e.g., effervescent tablets may absorb faster).
- Food Effect: While food may slightly delay the rate of absorption, it generally does not affect the extent of absorption.
Distribution
- Tissue Distribution: Widely distributed throughout most body fluids and tissues.
- Protein Binding: Has a relatively low plasma protein binding (10-25%) at therapeutic concentrations, but this can increase slightly with higher doses.
- Blood-Brain Barrier: Crosses the blood-brain barrier, which is essential for its central analgesic and antipyretic actions.
Metabolism
- Primary Site: Primarily metabolized in the liver (hepatic metabolism), accounting for 90-95% of the dose.
- Main Pathways:
- Glucuronidation (Major): Conjugation with glucuronic acid (approximately 45-55%).
- Sulfation (Minor): Conjugation with sulfate (approximately 20-30%).
- Cytochrome P450 (CYP2E1) Pathway (Minor but Critical): A small fraction (5-10%) is metabolized by cytochrome P450 enzymes (primarily CYP2E1) to form a highly reactive and toxic intermediate metabolite called N-acetyl-p-benzoquinone imine (NAPQI).
- NAPQI Detoxification: Under normal therapeutic doses, NAPQI is rapidly detoxified by conjugation with glutathione and subsequently excreted.
- Overdose Risk: In cases of overdose, the glucuronidation and sulfation pathways become saturated, leading to an increased proportion of paracetamol being shunted through the CYP2E1 pathway. This rapidly depletes hepatic glutathione stores, allowing NAPQI to accumulate and bind covalently to cellular macromolecules, leading to hepatocyte necrosis and severe liver damage.
Excretion
- Route: The majority of paracetamol and its metabolites are excreted renally (via the kidneys) in the urine.
- Half-life: The elimination half-life is typically 1 to 3 hours in individuals with normal liver function. This can be significantly prolonged in cases of liver impairment or overdose.
Extensive Clinical Indications & Usage
Panadol is a versatile medication indicated for a wide range of conditions requiring pain relief or fever reduction.
Primary Indications
Panadol is primarily used for the symptomatic relief of:
- Pain Relief (Analgesic):
- Mild to moderate pain of various etiologies.
- Headaches (tension headaches, migraines, cluster headaches, sinus headaches).
- Musculoskeletal pain (e.g., backache, osteoarthritis, sprains, strains, muscle aches, fibromyalgia).
- Dental pain (toothache, post-extraction pain).
- Post-operative pain.
- Menstrual pain (dysmenorrhea).
- Pain associated with colds and flu.
- Neuralgia.
- Fever Reduction (Antipyretic):
- Febrile conditions of various origins, including those associated with colds, influenza, and other viral or bacterial infections.
- Post-immunization fever.
Dosage Guidelines
Adherence to recommended dosage guidelines is paramount to ensure efficacy and prevent toxicity. The maximum daily dose is a critical safety limit.
General Adult Dosing
- Standard Dose: 500 mg to 1000 mg (1-2 tablets/caplets).
- Frequency: May be repeated every 4 to 6 hours as needed.
- Maximum Daily Dose: Do not exceed 4000 mg (4 grams) in a 24-hour period. Exceeding this limit significantly increases the risk of liver damage.
- Duration: For self-medication, limit use to a few days for fever and not more than 10 days for pain without medical consultation.
Pediatric Dosing
- Weight-Based Dosing: Pediatric dosing is strictly based on the child's weight, not age. Always use a measuring device provided with liquid formulations.
- Formulations: Available in various pediatric formulations such as syrups, suspensions, and chewable tablets, often with lower concentrations.
- Consultation: Always consult a doctor or pharmacist for precise pediatric dosing, or refer to the product's package insert, which typically includes a dosing chart.
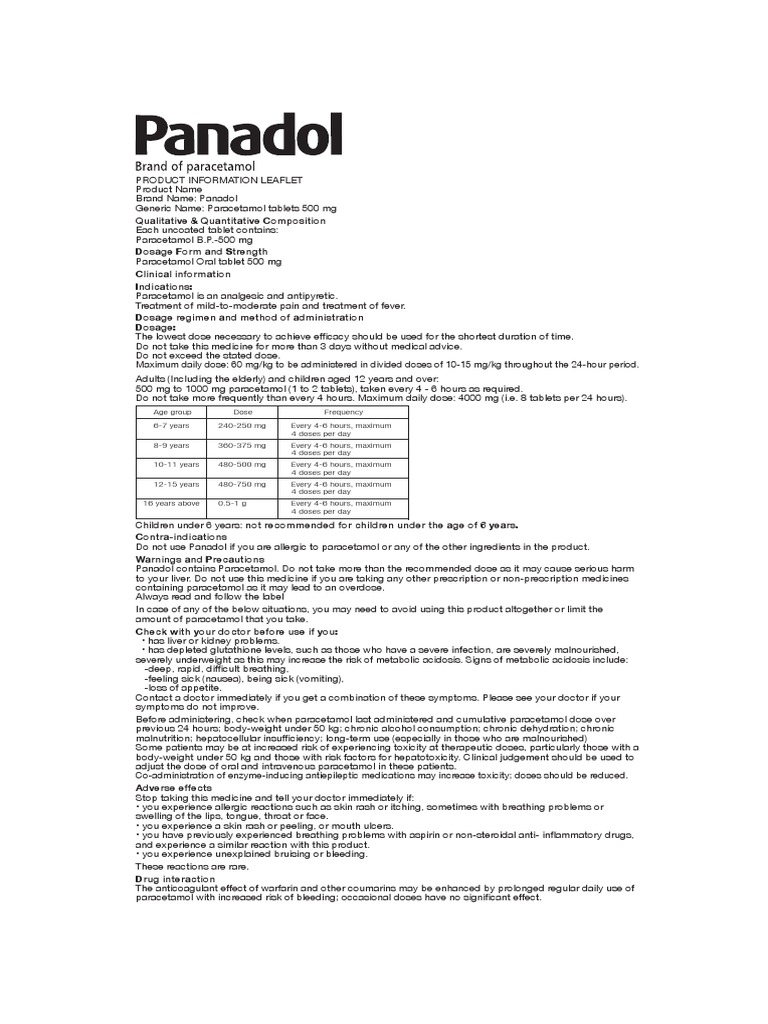
- General Guideline (approximate): 10-15 mg/kg body weight per dose, every 4-6 hours. Maximum 60 mg/kg/day.
| Age / Weight Range | Typical Single Dose (mg) | Max Doses in 24 hrs |
|---|---|---|
| 0-3 months | 60 mg | 4 |
| 3-6 months | 60-120 mg | 4 |
| 6-12 months | 120 mg | 4 |
| 1-2 years | 120-180 mg | 4 |
| 2-4 years | 180-240 mg | 4 |
| 4-6 years | 240 mg | 4 |
| 6-8 years | 240-360 mg | 4 |
| 8-10 years | 360-480 mg | 4 |
| 10-12 years | 480 mg | 4 |
| 12-16 years | 480-750 mg | 4 |
| Adults (16+) | 500-1000 mg | 4 |
Note: This table is a general guide. Always refer to the specific product's instructions or consult a healthcare professional.
Specific Populations
- Elderly: Generally, the same adult dose can be used, but caution is advised, especially if there is impaired kidney or liver function. Close monitoring may be necessary.
- Renal Impairment: Dose adjustment (e.g., extending dosing intervals) may be necessary in severe renal impairment (creatinine clearance < 10 mL/min).
- Hepatic Impairment: Panadol should be used with extreme caution or avoided in patients with pre-existing severe hepatic impairment or active liver disease. Reduced doses and extended intervals may be required under strict medical supervision.
- Chronic Alcohol Users: Increased risk of hepatotoxicity. Maximum daily dose should not exceed 2000 mg (2 grams) in these individuals, and medical advice is strongly recommended.
Administration Tips
- Panadol can be taken with or without food. Taking it with food may help reduce the chance of stomach upset in sensitive individuals, although this is less common with paracetamol than with NSAIDs.
- Always use the lowest effective dose for the shortest necessary duration.
- Be vigilant about checking the active ingredients of other medications (e.g., cold and flu remedies) to avoid accidental overdose from multiple paracetamol-containing products.
Risks, Side Effects, and Contraindications
While generally safe, Panadol is not without risks, particularly when misused. Understanding these is vital for safe administration.
Contraindications
Panadol is contraindicated in patients with:
* Severe Hepatic Impairment or Active Liver Disease: Due to the risk of exacerbating liver damage.
* Hypersensitivity: Known allergy or severe allergic reaction to paracetamol or any of its excipients (inactive ingredients).
* Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency: While not an absolute contraindication, high doses of paracetamol may induce hemolytic anemia in G6PD-deficient individuals.
Warnings and Precautions
Liver Damage (Hepatotoxicity)
- Most Serious Risk: The primary and most severe adverse effect associated with paracetamol, especially with overdose.
- Risk Factors:
- Exceeding the maximum recommended daily dose.
- Chronic alcohol consumption.
- Pre-existing liver disease (e.g., cirrhosis, hepatitis).
- Malnutrition or chronic fasting.
- Concomitant use of other hepatotoxic drugs.
- Certain genetic polymorphisms affecting metabolism.
- Symptoms of Overdose: Initial symptoms may be non-specific (nausea, vomiting, abdominal pain, loss of appetite, sweating) and may not appear for 24-48 hours. Delayed symptoms include jaundice, dark urine, and signs of liver failure. Immediate medical attention is crucial.
Allergic Reactions
- Rare but Serious: While uncommon, allergic reactions can occur, ranging from skin rashes, itching, and hives to more severe systemic reactions.
- Severe Cutaneous Adverse Reactions (SCARs): Very rare but life-threatening skin reactions such as Stevens-Johnson Syndrome (SJS), Toxic Epidermal Necrolysis (TEN), and Acute Generalized Exanthematous Pustulosis (AGEP) have been reported. Discontinue use immediately at the first sign of rash or other hypersensitivity reactions.
Kidney Damage (Nephrotoxicity)
- Less common than hepatotoxicity, but chronic high-dose use, especially in combination with NSAIDs, or in susceptible individuals with pre-existing kidney disease, can lead to renal papillary necrosis and kidney failure.
Blood Disorders
- Very rare reports of blood dyscrasias, including thrombocytopenia (low platelet count), agranulocytosis (severe reduction in white blood cells), leukopenia (low white blood cell count), and neutropenia (low neutrophil count).
Drug Interactions
Careful consideration of potential drug interactions is essential to prevent adverse outcomes.
| Interacting Drug/Substance | Effect of Interaction
What is Panadol?
Panadol is a common brand name for medicines containing the active ingredient paracetamol (also known as acetaminophen). It's one of the most widely used over-the-counter (OTC) pain relievers and fever reducers globally. Panadol products are available in various formulations, strengths, and combinations, designed to provide effective relief for a range of mild to moderate pain conditions and to reduce fever.
Why is Panadol so prevalent?
Its prevalence stems from its effectiveness, generally favorable safety profile when used as directed, and the fact that it does not typically cause the gastrointestinal irritation associated with NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) like ibuprofen or aspirin.
Key Applications:
- Pain Relief: Headaches, muscle aches, backache, toothache, menstrual pain, pain of osteoarthritis.
- Fever Reduction: Associated with colds, flu, and other infections.
Important Safety Note:
Despite its OTC status, Panadol is a potent medication that requires careful adherence to dosage instructions. Exceeding the recommended dose can lead to severe and potentially fatal liver damage. This guide will provide comprehensive details on safe and effective usage.
Deep Dive into Panadol's Technical Specifications and Mechanisms
Understanding the science behind Panadol helps in appreciating its benefits and limitations.
What is Paracetamol (Acetaminophen)?
Paracetamol (N-acetyl-p-aminophenol, APAP) is an aniline derivative. It is classified as an analgesic and antipyretic. Crucially, it is not an NSAID. This distinction is important as it has a different mechanism of action and side effect profile, particularly concerning gastrointestinal and antiplatelet effects.
Mechanism of Action
The precise mechanism of paracetamol is still under investigation, but it is primarily understood to exert its effects within the central nervous system (CNS).
- Central Prostaglandin Inhibition: Panadol is believed to selectively inhibit prostaglandin synthesis in the brain and spinal cord. Prostaglandins are chemical messengers that mediate pain, inflammation, and fever. Unlike NSAIDs, which inhibit cyclooxygenase (COX) enzymes (COX-1 and COX-2) throughout the body, paracetamol's action is thought to be more specific to central COX enzymes, potentially a distinct isoform known as COX-3, or through modulating the activity of existing COX enzymes under specific conditions (e.g., low peroxide tone