DEFINITION
Elbow synovectomy surgically removes the thickened, inflamed, and painful synovium of the elbow joint.Synovectomy is commonly performed for rheumatoid arthritis, hemophiliac synovitis, synovial chondromatosis, and inflammatory arthropathies.In the past, synovectomy has been performed through an open arthrotomy, but currently, arthroscopic synovectomy is the treatment of choice.Compared with open synovectomy, arthroscopic synovectomy can be performed as an outpatient procedure, allows more rapid recovery, and offers visualization of the entire elbow joint and recognition of concomitant pathology.
ANATOMY


PATHOGENESIS
Rheumatoid disease is a chronic, systemic autoimmune condition that causes a microvascular disease of the synovium and synovial cell proliferation with perivascular lymphocytosis.13Synovial tissue hypertrophy is the hallmark of the disease.Inflammation of the synovium causes a joint effusion, leading to pain, swelling, and limited range of motion.Continued inflammation results in the formation of an erosive, hyperplastic synovium known as apannus. The release of inflammatory cytokines results in continued cartilage damage, periarticular bone erosions, and soft tissue degradation.14Capsular distension and synovial hypertrophy can lead to gradual ligamentous, cartilaginous, and bony destruction resulting in progressive instability and deformity.Recurrent hemarthroses in factor 8 or 9 deficient hemophiliac patients often leads to hemophiliac arthropathy. Hemarthroses lead to blood absorption by the synovium with reactive synovitis which causes the synovium to produce proteolytic enzymes to destroy the blood, articular cartilage, and adjacent bone.NATURAL HISTORYThe patient with elbow synovitis will initially present with an elbow effusion, with pain, and restriction of motion. In early stages of inflammatory arthritis, deformity of cartilage and bone are not present. In the case of hemophiliac synovitis, the swollen hypervascular synovium is friable and recurrently bleeds into the elbow joint.P.902In 10% of rheumatoid patients, synovitis will spontaneously resolve.7In the rheumatoid patient, early medical management may slow natural disease progression.2 This should be attempted prior to surgical intervention.If synovitis persists, secondary changes may occur.A fixed flexion contracture may result from the patient holding the elbow in a flexed position to minimize pain caused by joint motion and capsular distension.The disease may result in atrophy of the brachialis muscle, bringing the median nerve and brachial artery much closer to the synovial lining.Destruction of the annular ligament may cause radial head instability with anterior displacement resulting from the pull of the biceps brachii muscle.Damage to either or both of the medial collateral ligament and lateral collateral ligament (LCL) complexes may result in gross mediolateral elbow instability.Proliferation of the synovium or distension of the joint capsule into the forearm may result in vascular, neural, or muscular dysfunction, particularly compression neuropathies of the ulnar or radial nerves.Prolonged synovitis ultimately results in erosion of the articular hyaline cartilage.Progressive cartilage degeneration and advancing arthritis is associated with subchondral cyst and marginal osteophyte formation, further weakening the joint capsule and ligamentous supports. Hemophiliac arthropathy of the elbow may create pseudocysts in the adjacent bone.The end stage of disease in the elbow is marked by severe loss of joint space, damage to subchondral boneand collapse, and progressive elbow instability. This results in a joint that is painful, weak, and unstable.7PATIENT HISTORY AND PHYSICAL FINDINGSPatients will present with a chief complaint of pain and stiffness in the elbow, especially in early stages of synovitis. Stiffness is typically the biggest problem, with loss of terminal flexion and extension. Pain may be present at rest and exacerbated by activities.Patients may report swelling and fullness in the elbow with impingement-type symptoms. Hemophiliac patients often report recurrent painful bleeding into the joint.Physical examination often reveals a boggy swelling posterolaterally, indicative of synovitis or effusion. Effusion and synovial hypertrophy can be palpated in the anconeus triangle and posterolateral gutter.Elbow range of motion in flexion, extension, and forearm rotation should be measured with a goniometer. If there is loss of motion, a soft end point suggests a soft tissue cause, such as tense effusion with synovitis or capsular contracture, whereas a firm end point suggests osseous deformity. Limited rotation may be caused by radial head deformity or instability.In rheumatoid patients with loss of rotation, examination and imaging of the wrist is important to evaluate for pathology of the distal radioulnar joint, which is commonly involved in these patients.Hemophiliac patients most often have an elbow flexion contracture, even if it is painless.Ligamentous examination includes varus and valgus stress testing to evaluate the collateral ligaments. The supine lateral pivot shift test and push-off test evaluate for posterolateral rotatory instability (PLRI). The radial head should be palpated during forearm rotation to evaluate for deformity or instability.Elbow instability is usually associated with more advanced disease, when joint effusion and synovial hypertrophy have caused ligamentous incompetence. Crepitus may present as degeneration of articular cartilage develops.A routine neurovascular examination is essential. The PIN and ulnar nerve may be compressed by synovitis.IMAGING AND OTHER DIAGNOSTIC STUDIESPlain radiographs include anteroposterior (AP), lateral, and oblique views to evaluate the degree of joint destruction. This aids in predicting the efficacy of synovectomy for pain relief.The Mayo classification of rheumatoid elbows12 grades the severity of disease based on radiographic appearance (FIG 2A-E).Grade I is primarily synovitis with no radiographic changes other than periarticular osteopenia or soft tissue swelling (FIG 2A,B).Grade II shows narrowing of the joint, but the architecture of the joint is intact (FIG 2C).Grade III demonstrates alteration of the subchondral architecture of the joint, such as thinning of the olecranon or resorption of the trochlea or capitellum (FIG 2D-E).Grade IV shows gross destruction of the joint. Grade V is ankylosis.The Arnold and Hilgartner classification of hemophiliac arthropathy is divided into five stages from mild to severe.1Computed tomography (CT) is helpful to better define osseous anatomy, such as osteophyte formation, radialhead deformity, or loose bodies.Magnetic resonance imaging (MRI) can determine the extent of synovitis, intra-articular nonossified loose bodies, and the integrity of the collateral ligament complexes.DIFFERENTIAL DIAGNOSISRheumatoid arthritisInflammatory arthropathies (Lupus, psoriatic arthritis) Hemophilic arthropathyPigmented villonodular synovitis (PVNS)NONOPERATIVE MANAGEMENTSystemic antirheumatoid agents may help control inflammation in rheumatoid patients. Nonsteroidal anti-inflammatory drugs (NSAIDS)Infusion of specific clotting factors for factor-deficient hemophilia patients, according to their specific deficiency Judicious use of intra-articular corticosteroid injectionsPhysical therapy to control swelling and regain range of motion Dynamic bracing to improve terminal flexion/extension
SURGICAL MANAGEMENT










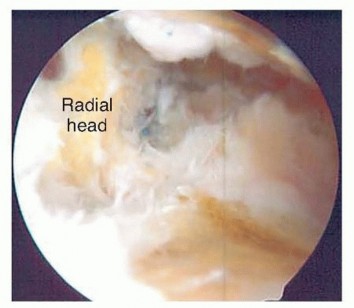
TECH FIG 6 • The posterior radiocapitellar joint can be visualized by advancing the arthroscope down the posterolateral gutter.1.Open SynovectomyLateral approach to the elbowThe arm is elevated and exsanguinated and a pneumatic tourniquet inflated.A 12-cm curvilinear incision is made on the lateral aspect of the elbow centered over the radiocapitellar joint. Dissection is carried sharply with scalpel down to the fascia, and fullthickness skin flaps are raised both anterior and posterior.The extended Kocher approach is typically used.10 A fatty stripe can be visualized that defines the interval between the anconeus and extensor carpi ulnaris (ECU). The fascia over the fatty stripe is incised, and blunt dissection with an elevator lifts the ECU anteriorly and anconeus posteriorly to expose the joint capsule. Keep the forearm pronated to protect the PIN.Alternatively, the lateral approach to the elbow can be used by developing the interval between the extensor digitorum communis (EDC) and the extensor carpi radialis longus (ECRL) or by splitting the EDC tendon. Through the lateral approach, the PIN is at risk of injury.The capsule and LCL complex should be in view.Make capsulotomy to access the elbow joint.Incise the capsule anterior to the equator of the radiocapitellar joint in line with the radius.Capsular incision should be made anterior to the lateral ulnar collateral ligament (LUCL) to avoid PLRI. The capsulotomy will go through a portion of the radial collateral ligament (RCL), which can be repaired at the completion of the case.Extend exposure with release of the LCL complex.With the LCL clearly identified, sharp release of the LCL off of the lateral epicondyle of the humerus allows the elbow joint to “book open” while preserving the integrity of the ligament.This provides excellent exposure to the anterior capsule and anterior compartment.The LCL complex can be repaired at the completion of the case through drill holes in the lateral epicondyle or with use of a double-loaded suture anchor.Incise annular ligament.The annular ligament can be incised in line with the radius and tagged for later repair.Take great caution in exposure distal to the annular ligament, as the PIN is at risk of injury. If dissection must be carried distal to the annular ligament, the PIN must first be identified and protected.Resect or keep radial head.At this stage, a radial head resection can be performed if indicated.Place small Hohmann retractors around the radial neck to protect the PIN and resect the radial head with a microsagittal saw.If the radial head is preserved, the anterior capsule can be exposed anterior to the radiocapitellar joint.Perform anterior synovectomy.Retractors can be placed into the elbow joint so the anterior musculature can be retracted anteriorly. The synovium can be excised with a rongeur, leaving the anterior capsule intact.If using electrocautery, take great care not to damage the articular cartilage. The medial recess cannot be accessed through this exposure.Extend exposure proximally to gain access to posterior compartment.Proximally, the interval between the triceps and ECRL can be defined. The triceps is retracted posterior and ECRL retracted anterior to gain access to the posterior compartment.A retractor can be placed deep to the triceps to access the posterior compartment.A synovectomy of the posterior compartment and the olecranon fossa can be performed.Expose the ulnar nerve if necessary.If indicated, the ulnar nerve can be exposed through a medial approach. Once the ulnar nerve is identified and protected, the posteromedial gutter can be exposed to complete the posterior synovectomy.ClosureThe LCL complex is repaired back to the lateral epicondyle of the humerus through drill holes or using a doubleloaded suture anchor.The capsulotomy is closed with interrupted suture, also repairing the split in the RCL. The interval between the anconeus and ECU is closed with suture.The subcutaneous layer and skin are closed with suture.Apply dressing.A bulky soft dressing is applied to the elbow to limit swelling and facilitate immediate range-of-motion exercises.P.908PEARLS AND PITFALLS
|Arthroscopic SynovectomyAvoid ▪ Keep inflow pressure low (<30 mm Hg if using pump), avoid capsular resection, excessive soft wrap forearm with elastic dressing during surgery|tissue swellingCreate a working space|1. If initial view is limited due to capsular tightness, use a switching stick through the lateral portal to elevate the capsule anteriorly off of the humerus.---|---Preserve capsular integrity|1. Use a nonaggressive full-radius shaver, keep shaver blades pointed away from capsule, use limited suctionAvoid iatrogenic injury to neurovascular structures|1. Know your three-dimensional anatomy and where nerves are at risk, judicious use of retractors to elevate the capsule and protect neurovascular structures, limited use of suction when working anterior to the radiocapitellar joint and in the medial gutterOpen SynovectomyAvoid damage to the LCL complex|1. Stay anterior to the equator of the radiocapitellar joint to avoid injury to the radial ulnar humeral ligament (RUHL) and resulting posterolateral instability; taking the entire LCL complex sharply off the lateral epicondyle preserves the integrity of the ligament.Avoid damage to the PIN|1. Do not carry dissection distal to the annular ligament.Avoid iatrogenic injury to neurovascular structures|1. Appropriate use of retractors; do not resect the capsule in the anterior compartment; do not attempt synovectomy in the medial gutter through the lateral approach unless the radial head has been removed. Most hemophiliac patients requiring elbow synovectomy will also require radial head resection for the radiocapitellar joint destruction. Bony curettage and osteoplasty may be required for hemophiliac pseudocysts in which the synovium has eroded subchondral bone into the medullary cavity especially between the trochlea and olecranon with telescoping.Increase exposure|1. Use an extensile approach; flex the elbow to remove tension from the anterior musculature and improve visualization in the anterior compartment; extend the elbow to improve visualization in the posterior compartment
POSTOPERATIVE CARE
Postoperative management depends on the extent of the surgery.Synovectomy alone is an outpatient procedure with initiation of early range of motion.Significant osseous resection or capsulectomy may be admitted for 23-hour observation with use of a postoperative drain, continuous passive motion (CPM), and cryocompression device.Indomethacin can electively be prescribed for heterotopic ossification prophylaxis.Patients are discharged with a continuous brachial plexus block for 72 hours for postoperative analgesia.Patients with severe hemophilia requiring factor 8 or 9 infusion during surgery will require infusion postoperative for several days as the hematologists taper the factor replacement dose.The bulky soft dressing is removed by the patient 48 to 72 hours postoperative, and range of motion is initiated. The portal sites are dressed with Band-Aids.Sutures are removed 7 to 10 days following surgery, and physical therapy is initiated for range of motion, terminal stretching, and edema control. Strengthening is begun at 4 to 6 weeks postoperative.
OUTCOMES
Elbow synovectomy, with or without radial head resection, is an effective treatment for the rheumatoid elbow and the hemophiliac elbow.The best results of elbow synovectomy, either open or arthroscopic, are in younger patients with greater than 90 degrees of flexion/extension, preserved articular cartilage, and mild bony deformities.12Studies indicate that 70% to 90% of patients have satisfactory outcomes within the first 3 to 5 years, although the results deteriorate with time.12Arthroscopic synovectomy offers the advantages of being less invasive with less soft tissue injury, which speeds recovery and rehabilitation and limits postoperative pain. The surgeon can visualize all intra-articular pathology and has superior access to the posterior compartment of the elbow.In 1997, Lee and Morrey11 reported on 14 patients who underwent arthroscopic synovectomy, with 93% good and excellent results. These results deteriorated to 57% at 42 months postoperative. Two cases of transient neurapraxia were reported and 4 patients were converted to total elbow arthroplasty.Horiuchi et al6 reported the results of 21 elbows after arthroscopic synovectomy, with good and excellent results for 71% of patients at 2 years. The Mayo Elbow Performance Score improved from 48.3 points preoperatively to 77.5 points postoperatively. The results deteriorated to 43% by 8 years. If elbows with advanced cartilage loss and bony deformity were excluded, the results were 100% and 71% of patients with good and excellent results at 2 and 8 years, respectively. Three patients had transient ulnar nerve paresthesias and two were converted to total elbow arthroplasty.In 2006, Tanaka and colleagues16 reported a prospective comparative study of arthroscopic versus open synovectomy with 23 elbows in each group. At a mean follow-up ofP.90910 years, 48% of those treated arthroscopically and 70% of those treated with open synovectomy had little or no pain. There was no significant difference with respect to pain, range of motion, or level of function.The results of both groups deteriorated with time.In 2011, Chalmers and coworkers4 performed a metaanalysis to compare the effects of arthroscopic versus open synovectomy on pain reduction, recurrence of synovitis, radiographic progression, and need for subsequent total joint arthroplasty. Patients undergoing arthroscopic synovectomy had similar pain reduction, but more frequent recurrences of synovitis and radiographic progression when compared to open synovectomy. The risk of subsequent total elbow arthroplasty was similar between the two groups.Kang et al9 reported on arthroscopic synovectomy in 26 rheumatoid elbows with radiographic changes that were mild to moderate. At a mean follow-up of 34 months, 73% of patients had good to excellent results.Pain decreased from 6.5 to 3.1, the mean flexion arc increased from 98 to 113 degrees, and the MayoElbow Performance Score improved from 58.5 to 77.4. Seven patients had radiographic progression of disease and four patients developed recurrent synovitis.Limited studies exist in the literature regarding the results of arthroscopic synovectomy for hemophilic arthropathy of the elbow.5,8,15,17 Studies are limited to very small numbers and often combine results of synovectomy of other joints. Either open or arthroscopic synovectomy dramatically decrease the rate ofrecurrent hemarthroses.
COMPLICATIONS
Nerve injury (PIN, median nerve, ulnar nerve) Instability with ligamentous injuryInfection, the risk of postoperative infection is higher in rheumatoid patients taking disease-modifying agents, which should be stopped 7 days prior to surgeryHeterotopic ossification Recurrence of synovitisREFERENCES1. Arnold WD, Hilgartner MW. Hemophilic arthropathy. Current concepts of pathogenesis and management. J Bone Joint Surg Am 1977; 59(3):287-305.2. Breedveld FC. Current and future management approaches for rheumatoid arthritis. Arthritis Res 2002;4(suppl 2):S16-S21.3. Bryan RS, Morrey BF. Extensive posterior exposure of the elbow joint. A triceps sparing approach. Clin Orthop Relat Res 1982;(166):188-192.4. Chalmers PN, Sherman SL, Raphael BS, et al. Rheumatoid synovectomy: does the surgical approach matter? Clin Orthop Relat Res 2011;469(7):2062-2071.5. Dunn AL, Busch MT, Wyly JB, et al. Arthroscopic synovectomy for hemophilic joint disease in a pediatric population. J Pediatr Orthop 2004;24:414-426.6. Horiuchi K, Momohara S, Tomatsu T, et al. Arthroscopic synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2002;84:342-347.7. Inglis AE, Figgie MP. Septic and non-traumatic conditions of the elbow: rheumatoid arthritis. In: Morrey BF, ed. The Elbow and Its Disorders, ed 2. Philadelphia: WB Saunders, 1993:751-766.8. Journeycake JM, Miller KL, Anderson AM, et al. Arthroscopic synovectomy in children and adolescents with hemophilia. J Pediatr Hematol Oncol 2003;9:726-731.9. Kang HJ, Park MJ, Ahn JH, et al. Arthroscopic synovectomy for the rheumatoid elbow. Arthroscopy2010;26(9):1195-1202.10. Kocher T. Textbook of Operative Surgery, ed 3. London: Adam & Charles Black, 1911.11. Lee BP, Morrey BF. Arthroscopic synovectomy of the elbow for rheumatoid arthritis. J Bone Joint Surg Br 1997;79(5):770-772.12. Lee BP, Morrey BF. Synovectomy of the elbow. In: Morrey BF, ed. The Elbow and Its Disorders, ed 3. Philadelphia: WB Saunders, 2000:708-717.13. Morrey BF, Adams RA. Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Joint Surg Am 1992;74:479-490.14. Papp SR, Athwal GS, Pichora DR. The rheumatoid wrist. J Am Acad Orthop Surg 2006;14(2):65-77.15. Tamurian RM, Spencer EE, Wojtys EM. The role of arthroscopic synovectomy in the management of hemarthrosis in hemophilia patients: financial perspectives. Arthroscopy 2002;18:789-794.16. Tanaka N, Sakahashi H, Hirose K, et al. Arthroscopic and open synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2006;88:521-525.17. Verma N, Valentino NA, Chawla A. Arthroscopic synovectomy in hemophilia: indications, technique and results. Haemophilia 2007; 13(suppl 3):38-44.
