Comprehensive Introduction and Patho-Epidemiology
Disorders of the posterior tibial tendon (PTT) encompass a complex, progressive spectrum of pathology that extends far beyond isolated tendinopathy. Historically referred to as posterior tibial tendon dysfunction (PTTD) or adult-acquired flatfoot deformity (AAFD), the orthopedic community has recently transitioned toward the nomenclature of Progressive Collapsing Foot Deformity (PCFD). This shift in terminology reflects a more profound understanding that the clinical presentation is rarely an isolated tendinous failure, but rather a multi-ligamentous, triplanar deterioration of the foot and ankle’s structural integrity. As the primary dynamic stabilizer of the medial longitudinal arch, the posterior tibial tendon plays an indispensable role in normal foot biomechanics. Insufficiency of this tendon initiates a predictable, progressive kinematic collapse of the foot and ankle, ultimately leading to profound disability, altered gait mechanics, and degenerative joint disease.
The epidemiology of posterior tibial tendon disorders reveals a distinct demographic predilection, predominantly affecting women in their fifth and sixth decades of life. The prevalence in this demographic is estimated to be as high as 10%, making it one of the most common causes of acquired foot deformity in adults. Systemic comorbidities play a critical role in the pathogenesis of the disease. Obesity is a nearly ubiquitous finding, exponentially increasing the mechanical load placed upon the medial longitudinal arch during the stance phase of gait. Furthermore, conditions that compromise microvascular perfusion—such as hypertension, diabetes mellitus, and hyperlipidemia—are strongly correlated with the development of tendinosis. Seronegative spondyloarthropathies and rheumatoid arthritis can also present with inflammatory tenosynovitis that accelerates structural attenuation.

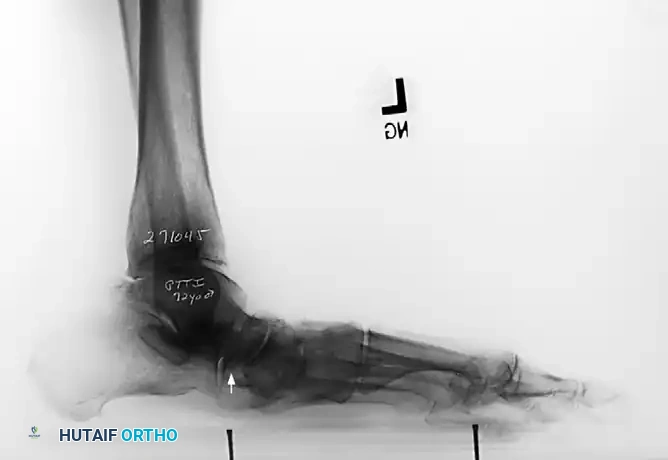
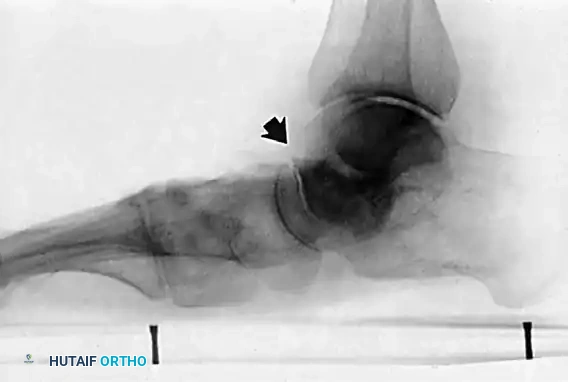
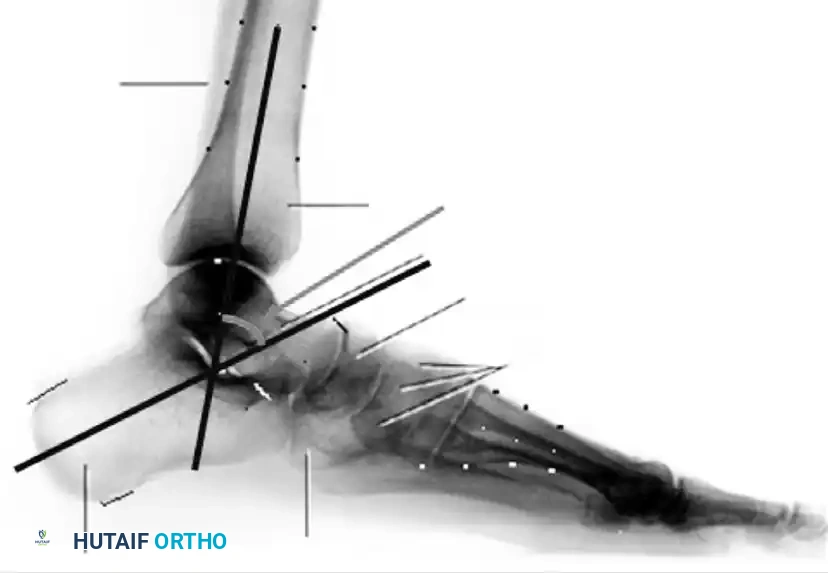
The talus slides distally, medially, and plantarward with the loss of the posterior tibial tendon and subsequent insufficiency of the plantar calcaneonavicular (spring) ligament.

Patient with bilateral pes planus demonstrating the classic loss of the medial longitudinal arch.
The pathophysiology of PTT degeneration is classically localized to an ischemic "watershed" zone located approximately 10 to 15 millimeters proximal to the tendon's insertion on the navicular tuberosity. Histologic analysis of surgical specimens from this region reveals a stark absence of acute inflammatory cells in chronic cases. Instead, the architecture is dominated by fibroblastic hyperplasia, mucinoid degeneration, hypervascularity of the paratenon, and a profound loss of normal linear collagen cross-linking. This degenerative cascade mechanically weakens the tendon, rendering it susceptible to longitudinal interstitial tearing and elongation under physiological loads. As the tendon elongates, its mechanical advantage is lost, shifting the immense forces of weight-bearing entirely onto the static ligamentous stabilizers of the midfoot and hindfoot, thereby precipitating the classic cascade of structural failure.
For the practicing orthopedic surgeon, mastering the nuances of this disorder requires an exhaustive understanding of hindfoot biomechanics, a meticulous clinical examination, and a comprehensive surgical armamentarium. The surgeon must be adept at evaluating the triplanar nature of the deformity—hindfoot valgus, midfoot abduction, and forefoot varus (supinatus)—and must tailor the intervention to address both the soft-tissue attenuation and the underlying bony malalignment. Failure to recognize and correct each component of the deformity invariably leads to recurrent collapse and surgical failure.
Detailed Surgical Anatomy and Biomechanics
A rigorous comprehension of the surgical anatomy and biomechanics of the posterior tibial tendon is paramount for executing successful reconstructive procedures. The posterior tibial muscle is the deepest muscle of the posterior compartment of the leg. It takes a broad, fleshy origin from the posterior aspect of the interosseous membrane, the proximal two-thirds of the medial surface of the fibula, and the lateral portion of the posterior surface of the tibia. The muscle belly transitions into a robust tendon in the distal third of the leg, descending posterior to the medial malleolus within the retromalleolar groove. Here, it is securely constrained by the flexor retinaculum. The tendon is enclosed within a synovial sheath that begins approximately 6 centimeters proximal to the medial malleolus and extends to its insertion.



Patients with posterior tibial tendon insufficiency as a result of attritional loss of continuity. Note the marked midfoot abduction, hindfoot valgus, and the convexity of the medial side with concavity of the lateral side.
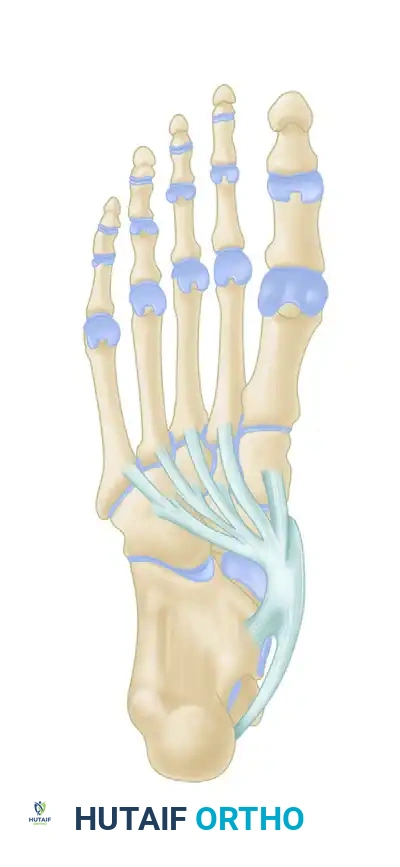
The insertion of the posterior tibial tendon is remarkably complex, reflecting its role as a global stabilizer of the midfoot. The main, largest slip inserts directly onto the prominent tuberosity of the navicular and the plantar surface of the medial cuneiform. A plantar slip continues distally to insert onto the bases of the second, third, and fourth metatarsals, the intermediate and lateral cuneiforms, and the cuboid. A recurrent slip courses laterally and proximally to insert on the sustentaculum tali of the calcaneus. This expansive, multi-pronged insertion allows the posterior tibial tendon to act as a dynamic sling, supporting the medial longitudinal arch and drawing the midtarsal bones together during muscular contraction.
Biomechanically, the posterior tibial tendon is the primary invertor of the subtalar joint and a secondary plantarflexor of the ankle. Its function is exquisitely timed within the normal gait cycle. During the initial heel strike and loading response, the hindfoot is driven into eversion (valgus), unlocking the transverse tarsal joint (Chopart's joint, comprising the talonavicular and calcaneocuboid articulations) to allow the foot to remain supple and absorb shock. As the stance phase progresses toward terminal stance and toe-off, the posterior tibial tendon fires concentrically. This action inverts the calcaneus, which dynamically alters the axes of the talonavicular and calcaneocuboid joints so they are no longer parallel. This "locking" of the transverse tarsal joint converts the midfoot into a rigid lever arm, allowing the gastrocsoleus complex to efficiently propel the body forward.
When the posterior tibial tendon becomes insufficient, this critical inversion at terminal stance fails to occur. The transverse tarsal joint remains unlocked, and the immense propulsive forces generated by the Achilles tendon are transmitted directly through a supple, unstable midfoot. This subjects the static stabilizers to massive, repetitive strain. The spring ligament (plantar calcaneonavicular ligament) complex, particularly its superomedial band, is the first to attenuate, allowing the talar head to plantarflex and rotate medially. Subsequently, the plantar fascia, the long and short plantar ligaments, and ultimately the superficial deltoid ligament (tibionavicular and tibiospring portions) fail. This sequential deterioration explains the progressive nature of the deformity, transitioning from a flexible arch collapse to rigid hindfoot valgus, profound forefoot abduction, and eventual ankle valgus instability.
Exhaustive Indications and Contraindications
The decision-making process in the surgical management of posterior tibial tendon disorders is dictated strictly by the stage of the disease, the flexibility of the deformity, the presence of degenerative joint disease, and the patient's physiologic status. The classification system originally developed by Johnson and Strom, and later modified by Myerson to include Stage IV, remains the foundational algorithm for guiding treatment. Surgical intervention is generally indicated when a minimum of 3 to 6 months of comprehensive conservative management—including immobilization in a controlled ankle motion (CAM) boot, custom rigid ankle-foot orthoses (AFOs), non-steroidal anti-inflammatory drugs, and targeted physical therapy—has failed to halt disease progression or alleviate debilitating symptoms.
For Stage I disease, characterized by tenosynovitis without structural deformity or elongation of the tendon, the primary indication for surgery is recalcitrant pain and swelling. The surgical goal is purely soft-tissue debridement (tenosynovectomy) to prevent further attritional wear. Stage II disease, defined by a flexible flatfoot deformity, represents the critical window for joint-sparing reconstruction. The indications for Stage II reconstruction include symptomatic medial arch collapse, hindfoot valgus, and forefoot abduction that are passively correctable. The surgeon must be prepared to perform a multi-apical reconstruction, combining a flexor digitorum longus (FDL) tendon transfer with structural osteotomies (e.g., medial displacement calcaneal osteotomy, lateral column lengthening, medial cuneiform dorsal opening wedge osteotomy) to restore the biomechanical axis.
Stage III disease is characterized by a rigid, fixed flatfoot deformity where the hindfoot and midfoot cannot be passively reduced to a neutral alignment. Degenerative arthritic changes are frequently present in the subtalar and talonavicular joints. Joint-sparing osteotomies are strictly contraindicated in Stage III, as attempting to realign a rigid, arthritic joint will universally result in severe pain and rapid failure. The indication here is a joint-sacrificing arthrodesis, typically a triple arthrodesis or a double arthrodesis (sparing the calcaneocuboid joint if un-involved), to create a stable, plantigrade foot. Stage IV disease involves failure of the deltoid ligament with subsequent valgus tilt of the talus within the ankle mortise. Indications for Stage IV include tibiotalocalcaneal (TTC) arthrodesis or, in highly selected patients with flexible ankle deformities and preserved cartilage, a complex deltoid ligament reconstruction combined with hindfoot arthrodesis.
| Stage / Pathology | Primary Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Stage I (Tenosynovitis, No Deformity) | Recalcitrant pain > 6 months; MRI evidence of severe tenosynovitis without tearing > 50%. | Active soft tissue infection; Charcot neuroarthropathy. | Poor vascular supply; Uncontrolled diabetes mellitus (HbA1c > 8.0). |
| Stage II (Flexible Deformity, Tendon Attenuation) | Painful, flexible pes planus; Inability to perform single heel rise; Failure of custom AFOs. | Rigid hindfoot/midfoot deformity; Subtalar or talonavicular arthritis. | Morbid obesity (BMI > 40); Active tobacco use; Severe osteopenia. |
| Stage III (Rigid Deformity, Arthritic Changes) | Fixed hindfoot valgus; Fixed forefoot abduction; Subfibular impingement pain; Arthritis on radiographs. | Active infection; Critical limb ischemia. | Non-ambulatory status; Severe peripheral neuropathy. |
| Stage IV (Ankle Valgus Tilt, Deltoid Failure) | Symptomatic ankle valgus instability; Talar tilt on weight-bearing mortise view. | Active infection; Uncorrectable soft tissue contractures preventing plantigrade positioning. | High-demand athletic expectations; Poor soft tissue envelope. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning begins with an exhaustive clinical examination. The patient must be observed standing barefoot to assess the global alignment of the lower extremity. The "Too Many Toes" sign is evaluated from a posterior vantage point; uncovering of the talonavicular joint due to forefoot abduction allows the examiner to visualize more toes lateral to the heel on the affected side compared to the contralateral limb. The single-leg heel rise test is critical for evaluating the functional integrity of the posterior tibial tendon and the flexibility of the hindfoot. A normal response involves inversion of the calcaneus as the patient rises onto the metatarsal heads. In Stage II or greater disease, the patient will either be unable to perform the maneuver or the calcaneus will remain locked in valgus.
Weight-bearing posterior view showing the three components of deformity: hindfoot valgus, forefoot abduction, and arch collapse. The Achilles tendon tightens in long-standing deformity, exacerbating heel valgus.

In the sitting position, when asked to hold the foot in plantarflexion-inversion, the patient unconsciously recruits the anterior tibial tendon to substitute for the deficient posterior tibial tendon.
Assessing the flexibility of the deformity is paramount for distinguishing between Stage II and Stage III disease. The examiner must passively invert the calcaneus to a neutral position and evaluate the forefoot. If the lateral border of the foot lifts off the ground, a fixed forefoot supinatus (varus) is present. This contracture is driven by the anterior tibial tendon acting unopposed over time. If this forefoot supinatus is not addressed surgically (typically via a Cotton osteotomy or first tarsometatarsal fusion), reducing the hindfoot to neutral will force the patient to walk on the lateral border of the foot. Additionally, the Silfverskiöld test must be performed to differentiate between isolated gastrocnemius tightness and a combined gastrocsoleus contracture, as equinus is a major deforming force in arch collapse.


The Silfverskiöld test determines selective gastrocnemius tightness. Passive dorsiflexion is measured with the knee flexed (left) and extended (right). A significant reduction in dorsiflexion with the knee extended indicates an isolated gastrocnemius contracture, necessitating a gastrocnemius recession.
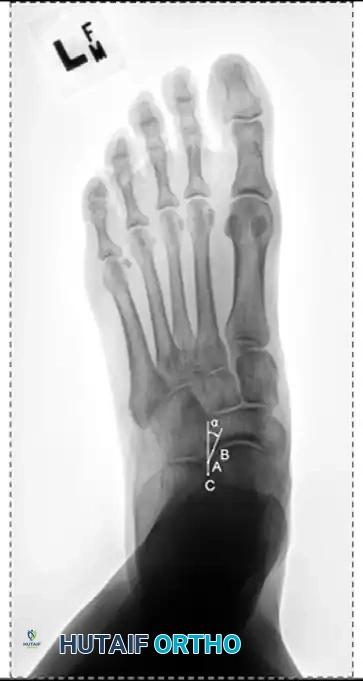
Radiographic evaluation demands strict weight-bearing views. On the AP view, the talonavicular coverage angle is measured to quantify forefoot abduction; normal coverage is approximately 70-80%, and progressive uncoverage correlates with spring ligament failure. The lateral view is utilized to assess the medial longitudinal arch via Meary's angle (the intersection of the longitudinal axes of the talus and the first metatarsal, which should be 0 degrees) and the calcaneal pitch. The lateral tibial-calcaneal angle is a sensitive metric for quantifying Achilles contracture. Advanced imaging with MRI is highly sensitive for evaluating the integrity of the PTT, spring ligament, and deltoid ligament. T2-weighted fat-suppressed images excel at demonstrating peritendinous effusions, interstitial tearing, and the "posterior tibial edema sign."
Measurement of the standing lateral tibial-calcaneal angle, utilized to quantify Achilles contracture.


Preoperative and postoperative radiographic comparisons demonstrating correction of Meary's angle and talonavicular coverage following structural reconstruction.


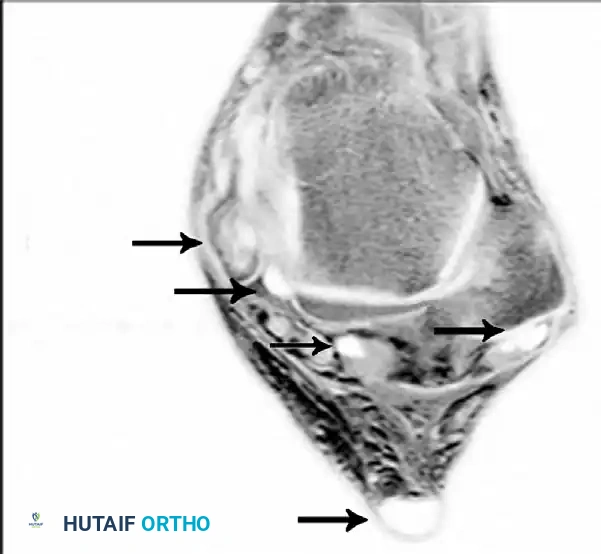
Axial MRI slices demonstrating severe tendinosis, fluid within the tendon sheath, and attenuation of the spring ligament complex.
Pre-operative templating involves determining the size of the structural grafts required for lateral column lengthening (typically 8-10 mm) or medial cuneiform osteotomies (typically 5-7 mm). Patient positioning is critical for intraoperative success. The patient is placed supine on the operating table with a large bump under the ipsilateral hip. This internally rotates the leg, bringing the lateral aspect of the hindfoot (necessary for the calcaneal osteotomies and fibular approaches) into a perfectly vertical orientation. A thigh tourniquet is applied, and the table must be fully radiolucent to accommodate unhindered multi-planar fluoroscopy.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be methodical, addressing the soft tissue and bony pathology in a sequential manner. For Stage I disease, the procedure is limited to a tenosynovectomy. A longitudinal incision is made along the course of the PTT, extending from the retromalleolar groove to the navicular tuberosity. The flexor retinaculum is incised, taking extreme care to preserve a 1-2 cm distal pulley near the medial malleolus to prevent postoperative tendon subluxation. Hypertrophic, inflamed synovium is meticulously excised using a combination of sharp dissection and rongeurs. If the tendon exhibits longitudinal splits involving less than 50% of its cross-sectional area, these are debrided and tubularized using a running, continuous non-absorbable suture (e.g., 2-0 Prolene) to restore a smooth gliding surface.

Patient with mild unilateral pes planus and recalcitrant tenosynovitis. Inflamed synovium is obvious along the tendon, causing loss of excursion. Radiographs are typically normal in this stage.
Stage II reconstruction is highly complex and multi-apical. The procedure typically begins with a gastrocnemius recession (Strayer or Baumann procedure) to eliminate the deforming equinus force. Next, the medial displacement calcaneal osteotomy (MDCO) is performed to correct hindfoot valgus. An oblique lateral incision is made posterior to the sural nerve and peroneal tendons. An oscillating saw creates a transverse osteotomy through the calcaneal tuberosity. The posterior fragment is translated medially by 8 to 10 millimeters, shifting the Achilles insertion medially and converting it into a potent invertor. Fixation is achieved with one or two large-fragment (6.5mm or 7.3mm) cannulated, partially threaded screws placed percutaneously from the posterior heel into the dense bone of the anterior calcaneus.


Intraoperative views and fluoroscopy demonstrating the medial displacement calcaneal osteotomy (MDCO) and subsequent screw fixation.
If significant forefoot abduction remains (Stage IIb), a lateral column lengthening (Evans osteotomy) is required. A vertical osteotomy is made in the anterior calcaneus, 1.5 cm proximal to the calcaneocuboid joint. The osteotomy is distracted with a lamina spreader, and a tricortical iliac crest autograft or allograft wedge (typically 8-10 mm) is impacted into the defect. This lengthens the lateral column, effectively swinging the forefoot medially and restoring talonavicular coverage. Fixation is secured with a specialized cervical H-plate or staples. Following the bony corrections, attention is turned to the medial soft tissues. The diseased PTT is excised. The flexor digitorum longus (FDL) tendon is identified at the Master Knot of Henry, transected distally, and mobilized. A drill hole is created dorsal-to-plantar through the navicular. The FDL is passed through this tunnel and tensioned with the foot held in maximal plantarflexion and inversion. Fixation is achieved using a biotenodesis screw or a suspensory button. The spring ligament is then imbricated and repaired using suture anchors placed into the sustentaculum tali.



Clinical progression of a Stage II reconstruction: Preoperative deformity, intraoperative correction via osteotomies and tendon transfer, and final postoperative alignment.
For Stage III rigid deformities, a joint-sacrificing triple arthrodesis is the gold standard. Through combined medial and lateral approaches, the articular cartilage of the subtalar, talonavicular, and calcaneocuboid joints is meticulously denuded down to bleeding subchondral bone using curettes, osteotomes, and high-speed burrs. The critical step is positioning: the hindfoot MUST be fused in approximately 5 degrees of valgus. Fusing the hindfoot in varus or neutral locks the transverse tarsal joint permanently, leading to rigid lateral border overload, stress fractures of the 5th metatarsal, and intractable pain. The forefoot is rotated to a neutral plantigrade position. Fixation involves large cannulated screws (7.3mm) across the subtalar joint, and either dual 4.5mm screws or specialized compression plates for the talonavicular and calcaneocuboid joints.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of the posterior tibial tendon is fraught with potential complications, given the massive biomechanical forces at play and the complexity of multi-apical corrections. Neurologic injury is one of the most frequent complications, particularly involving the sural nerve during the lateral approach for the MDCO or Evans osteotomy. The sural nerve courses unpredictably along the lateral hindfoot and is exquisitely sensitive to retraction neuropraxia or direct transection. Medially, the saphenous nerve and the medial calcaneal branches of the tibial nerve are
Clinical & Radiographic Imaging Archive