Pathoanatomy and Biomechanics of Radial Longitudinal Deficiency
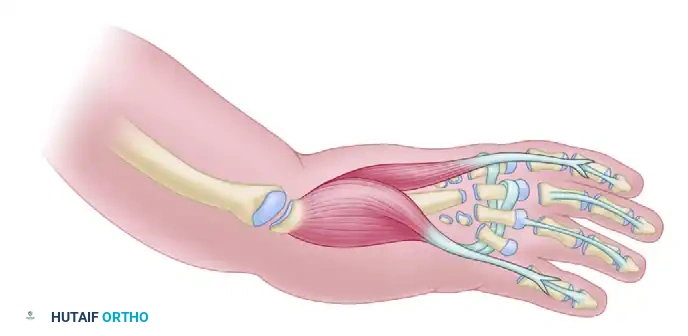
Radial longitudinal deficiency (RLD), historically referred to as radial clubhand, represents a complex spectrum of congenital upper extremity anomalies characterized by hypoplasia or complete aplasia of the radius and radial-sided carpal bones. This structural deficit eliminates the critical skeletal support for the radial aspect of the carpus, leading to a severe biomechanical imbalance.
The extrinsic flexor and extensor tendons, lacking their normal osseous fulcrum, exert an unopposed radial and volar deforming force. Over time, this results in a progressive, rigid perpendicular relationship between the hand and the forearm. The distal ulna frequently develops a compensatory bow, and the surrounding soft tissues—particularly the radial collateral ligament, radiocarpal capsule, and radial-sided neurovascular structures—become severely contracted.
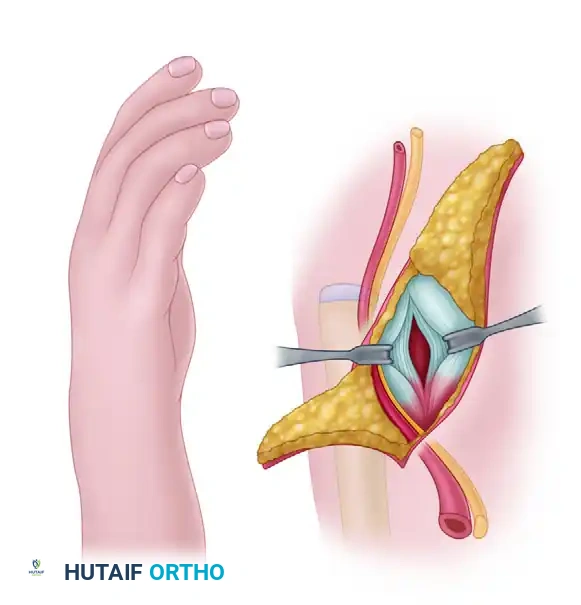
Clinical Pearl: In severe RLD, the median nerve is often anomalous. It frequently lies superficially along the radial border of the forearm, directly beneath the fascia, acting as a tethering cord. Extreme caution must be exercised during the radial approach to avoid iatrogenic transection of this superficially displaced nerve.
Bora et al. established that successful management of this deformity requires a comprehensive, staged approach. Treatment must begin immediately after birth with serial corrective casting and passive stretching to elongate the contracted radial soft tissues. Once the patient reaches 6 to 12 months of age, surgical centralization of the carpus over the distal ulna is indicated. To maintain this correction and counteract the persistent radial deforming forces, a second-stage tendon transfer is performed 6 to 12 months later.
Preoperative Assessment and Indications
The primary goal of centralization is to reposition the carpus over the distal end of the ulna, thereby creating a stable mechanical fulcrum that improves the functional length of the extremity, enhances digital flexor mechanics, and provides a cosmetically acceptable alignment.
Indications for Surgery
- Bayonet-type radial deviation of the hand that cannot be actively corrected.
- Adequate elbow flexion. (The hand must be able to reach the mouth post-centralization).
- Failure of conservative serial casting to maintain acceptable alignment.
Absolute Contraindications
- Severe Elbow Extension Contracture: If the elbow lacks flexion, the radial deviation of the wrist is often the only mechanism allowing the child to bring the hand to the mouth for feeding. Straightening the wrist in such patients will severely compromise their independence.
- Mild deformities with adequate radial support (e.g., Type I or mild Type II RLD) where functional deficit is minimal.
- Older patients with severe, rigid, untreated deformities where soft tissue release would compromise neurovascular integrity.
STAGE I: Surgical Centralization of the Hand (Bora et al. Technique)
The centralization procedure is typically performed when the infant is between 6 and 12 months of age. At this stage, the anatomical structures are large enough to handle surgically, yet the soft tissues remain pliable enough to allow for correction without excessive tension on the neurovascular bundles.
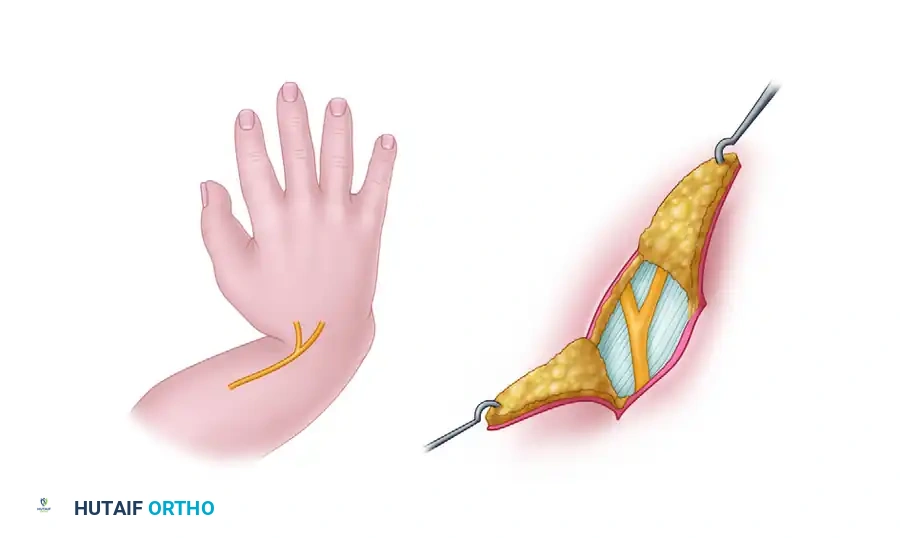
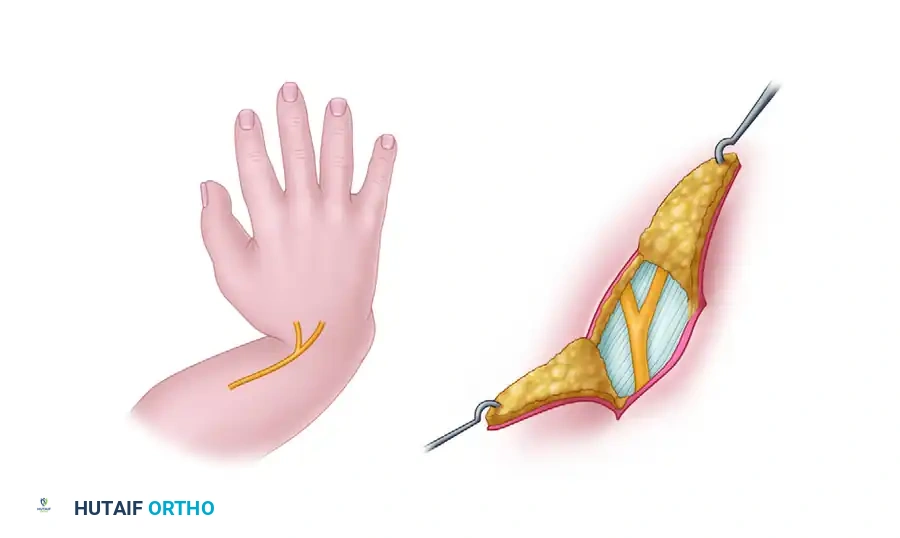
1. Positioning and Incision
The patient is placed supine with the affected upper extremity on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm.
- Design a radial S-shaped or Z-plasty incision over the radial aspect of the wrist. This incision allows for adequate exposure of the contracted radial structures while providing a lengthening effect during closure to accommodate the corrected posture.

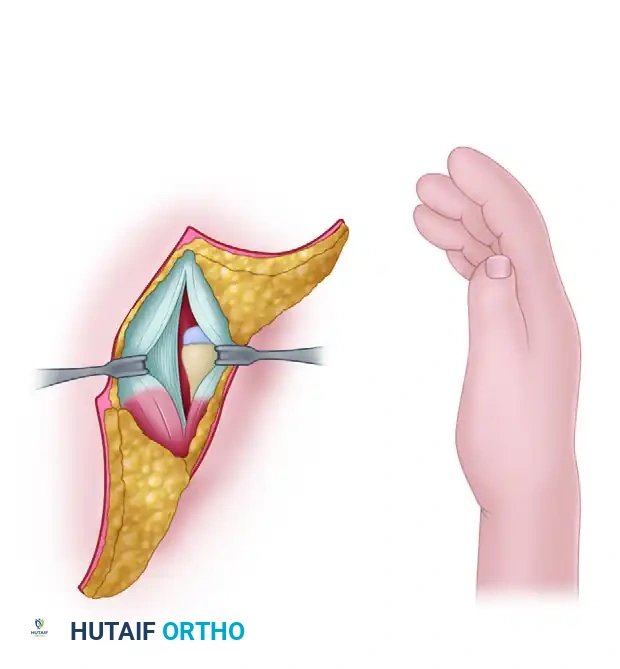
2. Soft Tissue Release and Exposure
- Carefully elevate the skin flaps. Identify and protect the dorsal sensory branch of the ulnar nerve, the superficial radial nerve (if present), and the superficially displaced median nerve.
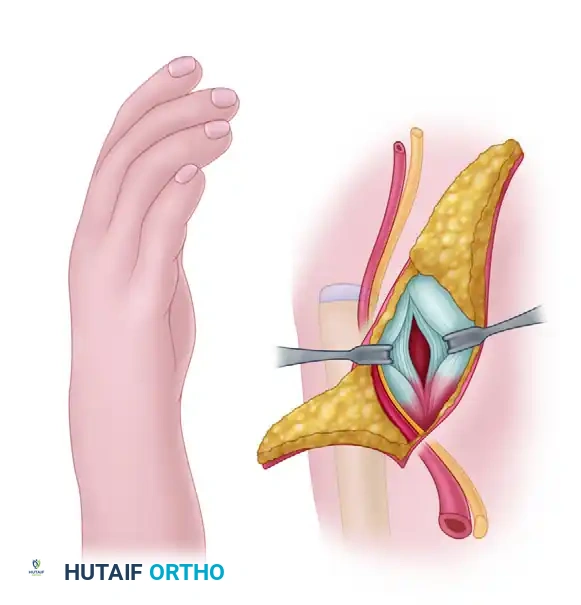
- Identify the thickened, fibrotic bands representing the anlage of the radius and the contracted radiocarpal ligaments.
- Perform a thorough release of the radial-sided soft tissues, including the radial collateral ligament and the volar capsule, to mobilize the carpus.

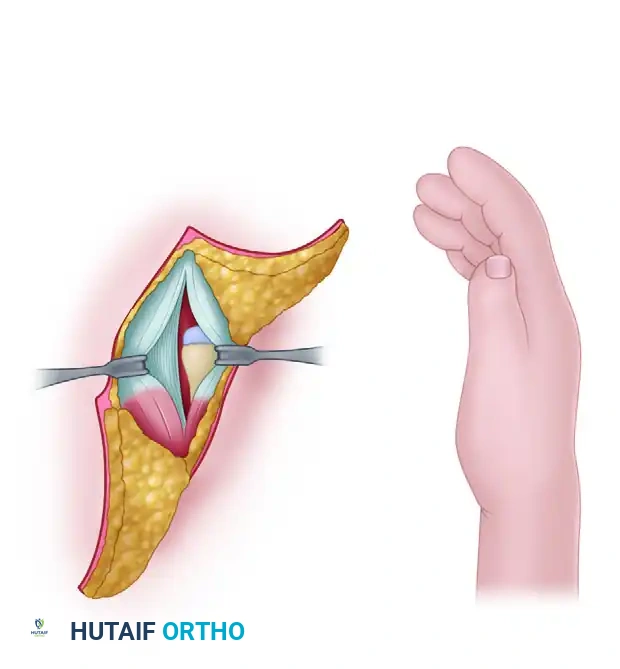
3. Carpal Preparation and Slot Creation
To prevent the distal ulna from sliding radially or volarly off the carpus postoperatively, a central slot must be created within the carpal mass to securely seat the ulnar epiphysis.
- Isolate the central carpal bones. In the infant carpus, these are largely cartilaginous.
- Carefully excise the lunate and the capitate. This creates a deep, rectangular notch or "slot" in the proximal carpal row, perfectly sized to receive the distal ulnar epiphysis.
Surgical Warning: Extreme care must be taken not to damage the distal ulnar physis during preparation and seating. Physeal arrest of the distal ulna is a devastating complication that will lead to severe forearm shortening and recurrent deformity.
4. Ulnar Preparation and Transposition
- Make a separate longitudinal incision over the distal ulnar epiphysis if the primary incision does not provide adequate exposure.
- Free the distal ulna from its surrounding soft tissue attachments, taking meticulous care to preserve the extensor carpi ulnaris (ECU) and extensor digiti minimi (EDM) tendons, as these will be crucial for postoperative ulnar stability.
- Transpose the distal end of the ulna through the plane between the flexor and extensor tendons.
5. Skeletal Fixation
- Seat the distal ulnar epiphysis deeply into the surgically created carpal slot (the space previously occupied by the lunate and capitate).
- Align the longitudinal axis of the ulna directly with the base of the long finger (third) metacarpal.
- Drive a smooth, stout Kirschner wire (typically 0.045 or 0.062 inch, depending on patient size) longitudinally through the carpus and into the intramedullary canal of the third metacarpal.
- Once the wire is secured in the metacarpal, drive it retrograde across the carpal slot and down the intramedullary canal of the ulnar shaft. This transfixes the hand in a centralized, neutral position.
6. Radiographic Confirmation and Closure
- Obtain intraoperative fluoroscopic imaging in both anteroposterior and lateral planes to confirm that the ulna is perfectly aligned with the long axis of the third metacarpal and that the K-wire is centrally placed within the medullary canals.
- Suture the dorsal radiocarpal ligament and redundant dorsal capsule tightly over the neck of the ulna to reinforce the stabilization.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the skin. If skin tension is excessive on the radial side, a local rotation flap or full-thickness skin graft may be required.
Stage I Postoperative Protocol
- Apply a well-padded, long-arm cast.
- Unilateral Deformity: Place the elbow at 90 degrees of flexion with the wrist and hand in a neutral position.
- Bilateral Deformity: Place the elbows at 90 degrees. Position one forearm in 45 degrees of pronation and the other in 45 degrees of supination to facilitate bilateral function and feeding.
- The cast and K-wire are typically maintained for 6 to 8 weeks. Following pin removal, a custom-molded thermoplastic splint is applied and worn strictly at night until skeletal maturity to prevent recurrence.
STAGE II: Tendon Transfers for Dynamic Rebalancing
Despite a successful skeletal centralization, the inherent soft tissue imbalance remains. The powerful radial flexors and extensors will inevitably pull the hand back into radial deviation if a dynamic counterforce is not established. Bora et al. advocated for tendon transfers 6 to 12 months following the initial centralization to provide an active ulnar-tethering force.
Preoperative Assessment of Donor Tendons
Before attempting to transfer the flexor digitorum superficialis (FDS) tendons, their function must be rigorously tested. In patients with RLD, the FDS tendons to the radial digits are frequently hypoplastic, fibrotic, or entirely absent.
- Clinical Testing: Passively maintain the metacarpophalangeal (MCP) joints and the wrist joint in hyperextension, and keep the interphalangeal joints in extension. Release one finger at a time. An intact, functioning FDS tendon will actively flex the proximal interphalangeal (PIP) joint of the released finger.
- Only functioning FDS tendons (typically from the long and ring fingers) should be selected for transfer.
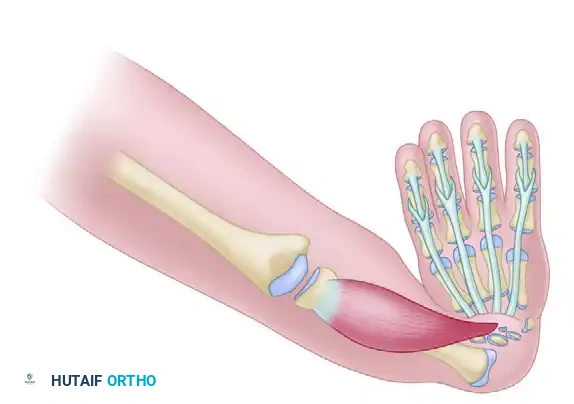
Surgical Technique for Tendon Transfer
- Under general anesthesia and tourniquet control, make a midlateral incision on the ulnar side of the long finger at the level of the PIP joint.
- Identify the FDS tendon slips, divide them at their insertion on the middle phalanx, and withdraw them into the proximal forearm through a separate volar incision.
- Repeat this process for the ring finger FDS if dual transfers are planned.

- Route the harvested FDS tendons subcutaneously around the ulnar border of the forearm to the dorsal aspect of the wrist.
- The tendons are typically woven into the extensor carpi ulnaris (ECU) tendon or anchored directly to the dorsal ulnar aspect of the carpus. This creates a dynamic "checkrein" that actively pulls the hand into ulnar deviation, counteracting the radial deforming forces.

- Set the tension of the transfer with the wrist in neutral to slight ulnar deviation. Suture the transfer securely using non-absorbable braided suture (e.g., 3-0 or 4-0 Ethibond).
Biomechanics of the Transfer: By rerouting a volar-radial force (FDS) to a dorsal-ulnar insertion (ECU or dorsal carpus), the surgeon effectively eliminates a deforming force while simultaneously creating a corrective, stabilizing force. This dual benefit is critical for long-term maintenance of the centralized carpus.
Clinical Outcomes and Long-Term Management
The combination of skeletal centralization and dynamic tendon transfer significantly improves the cosmetic appearance and functional capacity of the extremity. By stabilizing the wrist, the extrinsic digital flexors are provided with a rigid fulcrum, which markedly improves grip strength and digital dexterity.
Complications and Pitfalls
- Recurrent Radial Deviation: This is the most common long-term complication. It occurs due to the relentless pull of the radial musculature, inadequate initial soft tissue release, or failure of the tendon transfer. Continuous night splinting until skeletal maturity is mandatory to mitigate this risk.
- Physeal Arrest: Damage to the distal ulnar physis during slot creation or K-wire insertion will halt longitudinal growth of the ulna. Given that the ulna is already the sole bone of the forearm in these patients, any further loss of length is functionally devastating.
- Stiffness: Prolonged immobilization can lead to severe stiffness of the digits. Early mobilization of the fingers while the wrist remains pinned is essential.
