Patient Presentation & History
We present the case of Mr. J.D., a 35-year-old male, previously fit and healthy, with no significant medical comorbidities or regular medications. He presented to the emergency department following a high-speed motorcycle collision with a stationary object. The mechanism involved a direct impact to his left lower extremity, followed by entrapment under the motorcycle for approximately 15 minutes before extrication by emergency services.
Initial pre-hospital assessment revealed a grossly deformed left lower leg with significant swelling and ecchymosis. He was hemodynamically stable on arrival (BP 130/80 mmHg, HR 92 bpm, RR 16, SaO2 99% on room air). Glasgow Coma Scale (GCS) was 15. Primary survey was negative for life-threatening injuries. Secondary survey revealed no other major traumatic injuries, specifically ruling out head, chest, abdominal, and spinal trauma.
His pain was initially well-controlled with intravenous fentanyl, however, he reported a significant increase in pain in his left lower leg, disproportionate to the analgesia administered, approximately 4 hours post-injury. He described the pain as "bursting" and "tight," worsening with any movement, particularly passive dorsiflexion of the ankle. He denied any pre-existing neurological deficits or prior injuries to the affected limb. Smoking status was non-smoker, and he consumed alcohol socially. No known allergies.
Clinical Examination
Upon focused re-evaluation of the left lower extremity approximately 4 hours post-injury, the following findings were noted:
Inspection:
The left lower leg exhibited marked circumferential swelling, particularly in the anterior and lateral compartments. The skin appeared taut, shiny, and erythematous, with developing ecchymosis over the fracture site. A significant open wound was not appreciated, suggesting a closed or Gustilo-Anderson Type I open fracture at worst (pending further exploration). No blistering was evident at this stage. The foot appeared well-perfused with appropriate skin turgor and color.
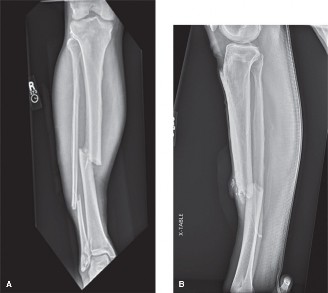
Figure 1: Representative image of a tense, swollen lower limb demonstrating signs suggestive of compartment syndrome. Note the characteristic taut, shiny skin and prominent swelling.
Palpation:
All four compartments of the left lower leg (anterior, lateral, deep posterior, superficial posterior) were palpably tense, non-compressible, and exquisitely tender to light touch. The anterior compartment felt particularly firm, almost "wood-like." Pulses (dorsalis pedis and posterior tibial) were palpable, albeit somewhat diminished compared to the contralateral limb, but definitively present. Capillary refill in the toes was brisk (<2 seconds).
Range of Motion (ROM):
Active range of motion of the ankle and toes was severely limited due to pain. Passive dorsiflexion of the ankle and passive plantarflexion of the toes elicited excruciating pain in the calf and foot, respectively. Passive stretch of the anterior compartment musculature (plantarflexion of the ankle) caused severe pain, as did passive stretch of the superficial and deep posterior compartments (dorsiflexion of the ankle and extension of the toes).
Neurological Assessment:
*
Motor:
Weakness was noted in ankle dorsiflexion (tibialis anterior, innervated by deep peroneal nerve) and great toe extension (extensor hallucis longus, also deep peroneal nerve), graded 2/5 against gravity. Plantarflexion strength was 3/5. Eversion (peroneus longus/brevis, superficial peroneal nerve) and inversion (tibialis posterior, tibial nerve) were difficult to assess accurately due to pain, but gross motor function appeared mildly impaired (4/5).
*
Sensory:
Numbness and paresthesias were reported in the first web space of the foot (deep peroneal nerve distribution). Light touch sensation over the lateral aspect of the foot (superficial peroneal nerve distribution) was also diminished. Sensation over the plantar aspect of the foot (tibial nerve) and medial aspect of the foot (saphenous nerve) was intact.
*
Reflexes:
Patellar reflex was 2+, Achilles reflex was 1+ (diminished) but present.
Vascular Assessment:
As mentioned, dorsalis pedis and posterior tibial pulses were palpable bilaterally, although the left limb's pulses were subjectively weaker. Doppler signals confirmed patency of both arteries. Capillary refill was brisk. This finding, while reassuring for macrovascular integrity, underscores the critical concept that palpable pulses do
not
rule out compartment syndrome.
Based on the clinical findings – significant pain out of proportion, pain with passive stretch, tense compartments, sensory deficits in specific nerve distributions, and motor weakness – a diagnosis of acute compartment syndrome of the left lower leg was highly suspected.
Imaging & Diagnostics
Plain Radiographs (AP and Lateral views of the left tibia/fibula):
Initial radiographs revealed a comminuted, mid-diaphyseal spiral fracture of the left tibia, with an associated non-displaced fracture of the proximal fibula. The fracture morphology suggested a rotational and bending force, consistent with the motorcycle accident mechanism. There was approximately 15 degrees of varus angulation and 10 mm of shortening. No significant bone loss or high-energy comminution suggesting a Gustilo-Anderson Type III open fracture was noted from the X-rays alone. The surrounding soft tissue swelling was prominent.
*
Interpretation:
The fracture pattern is amenable to intramedullary nailing. The significant soft tissue swelling on X-ray correlates with the clinical examination findings.
Compartment Pressure Measurements:
Given the strong clinical suspicion, emergent compartment pressure measurements were performed using a Stryker STIC device.
*
Anterior compartment:
65 mmHg
*
Lateral compartment:
58 mmHg
*
Deep posterior compartment:
48 mmHg
*
Superficial posterior compartment:
42 mmHg
* Diastolic blood pressure (DBP) at the time of measurement was 70 mmHg.
*
Delta Pressure:
Anterior compartment (65 - 70 = -5 mmHg), Lateral compartment (58 - 70 = -12 mmHg), Deep posterior compartment (48 - 70 = -22 mmHg), Superficial posterior compartment (42 - 70 = -28 mmHg).
- Interpretation: Absolute pressures >30-40 mmHg and a delta pressure (DBP - Intracompartmental Pressure) of <20-30 mmHg are highly indicative of compartment syndrome. In this case, the anterior and lateral compartments demonstrated critically elevated pressures, with delta pressures of -5 mmHg and -12 mmHg, respectively, unequivocally confirming the diagnosis of acute compartment syndrome. The deep and superficial posterior compartments also showed significantly elevated pressures, warranting a complete four-compartment fasciotomy.
Other Diagnostics:
*
Laboratory Bloods:
Initial blood work showed mild leukocytosis (WBC 12.5 x 10^9/L), hemoglobin 14.2 g/dL, and normal electrolytes. Creatinine kinase (CK) levels were elevated at 1200 U/L (normal <200 U/L), suggestive of muscle ischemia and rhabdomyolysis, which can be a consequence or co-factor in compartment syndrome. Myoglobinuria was present on urine dipstick.
CT/MRI indications:
CT or MRI is typically
not
indicated or appropriate for the acute diagnosis of compartment syndrome, as it delays definitive surgical intervention. These modalities may be used in elective settings for chronic exertional compartment syndrome or for detailed assessment of concomitant soft tissue injuries or complex fracture patterns once compartment syndrome has been ruled out or addressed. In an emergent setting, time is tissue. Pre-operative templating for tibial nailing can be performed using standard X-ray measurements if necessary, but immediate surgical intervention for compartment syndrome takes precedence.
Differential Diagnosis
The acute presentation of pain and swelling in the lower extremity after trauma necessitates a comprehensive differential diagnosis. Distinguishing acute compartment syndrome from other conditions is paramount due to its time-sensitive nature and devastating potential sequelae.
| Feature | Acute Compartment Syndrome | Deep Vein Thrombosis (DVT) | Cellulitis | Rhabdomyolysis (isolated, no CS) |
|---|---|---|---|---|
| Pathophysiology | Increased interstitial pressure compromising microvascular perfusion leading to tissue ischemia. | Thrombus formation in deep veins, causing venous outflow obstruction and inflammation. | Bacterial infection of dermis and subcutaneous tissue. | Extensive muscle breakdown releasing intracellular contents into circulation. |
| Pain Character | Severe, "bursting," tight, disproportionate to injury, worsens with passive stretch. | Aching, cramping, typically duller, may worsen with standing/walking. | Burning, throbbing, tender to touch, less often "bursting." | Diffuse muscle soreness, weakness, cramping, often bilateral. |
| Swelling | Tense, firm, "wood-like" compartments, circumferential. | Edematous, pitting, usually distal to affected vein, often unilateral. | Localized, erythematous, warm, non-pitting. | Diffuse, generalized muscle swelling and tenderness, not compartment specific. |
| Skin Changes | Taut, shiny, often erythematous. Blistering may occur late. | Erythema, warmth, tenderness along vein distribution. | Erythema with poorly defined borders, warmth, often fever. | Often none, may have some diffuse swelling or bruising if traumatic cause. |
| Pulses | May be palpable (present in 90-95% of cases), but subjective weakness possible. | Usually normal, unless severe edema compromises arterial flow. | Normal. | Normal. |
| Motor Weakness | Present, particularly in affected compartment muscles. | Typically absent, unless severe edema causes nerve compression. | Absent, unless severe pain limits movement. | Profound weakness, fatigue. |
| Sensory Deficits | Paresthesias, numbness in specific nerve distributions (e.g., first web space for deep peroneal). | Uncommon, unless severe edema causes generalized nerve compression. | Absent. | Absent, unless severe systemic effects. |
| Temperature | Normal or slightly elevated locally. | Increased local warmth. | Significantly increased local warmth, often systemic fever/chills. | Normal, may be febrile if severe systemic inflammation. |
| Specific Signs | Pain with passive stretch of muscles, tense compartments. | Homan's sign (controversial), palpable cord. | Lymphangitis, regional lymphadenopathy. | Dark urine (myoglobinuria), elevated CK. |
| Diagnostic Confirmation | Intracompartmental pressure measurement. | Duplex ultrasonography (gold standard). | Clinical diagnosis, culture from wound/bulla if present. | Serum CK levels, urine myoglobin. |
| Treatment | URGENT FASCIOTOMY. | Anticoagulation, thrombolysis in select cases. | Antibiotics. | IV fluids, electrolyte management, renal support. |
In Mr. J.D.'s case, the classic "6 Ps" (pain out of proportion, pain with passive stretch, paresthesia, pallor, pulselessness, paralysis) were being observed, specifically marked pain out of proportion, pain with passive stretch, paresthesia, and motor weakness. The key differentiating factor was the extreme tenseness of the compartments and the subsequent critical compartment pressure measurements. While DVT or cellulitis could cause pain and swelling, they would not typically present with the same degree of compartment rigidity or specific neurological deficits. Rhabdomyolysis was a concomitant finding, not an alternative diagnosis in this context, but rather a sequela of prolonged muscle ischemia.
Surgical Decision Making & Classification
The definitive diagnosis of acute compartment syndrome based on clinical examination and confirmed by compartment pressure measurements (delta pressure <20-30 mmHg in multiple compartments) mandated immediate surgical intervention . Delaying fasciotomy beyond 6-8 hours from symptom onset significantly increases the risk of irreversible muscle necrosis, nerve damage, and long-term disability, including Volkmann's contracture, chronic pain, and limb loss.
Operative vs. Non-operative:
Compartment syndrome is a surgical emergency. Non-operative management is contraindicated once the diagnosis is established. The only scenario for observation without immediate surgery would be if compartment pressures were borderline and clinical signs equivocal, in which case strict serial examinations and repeat pressure measurements would be necessary. This was not the case for Mr. J.D.
Classification:
1.
Gustilo-Anderson Classification for Open Fractures:
While no obvious large open wound was present, the significant soft tissue swelling and potential for bone spike penetration from a comminuted tibia fracture necessitate careful intraoperative assessment. At minimum, this would be considered a Gustilo-Anderson Type I open fracture if there's a small wound (<1cm) with minimal contamination and simple fracture pattern, or potentially Type II if the wound is larger (>1cm) or there's moderate soft tissue damage. The decision for intramedullary nailing of the tibia fracture would depend on this classification; open fractures generally require thorough debridement and often staged fixation. For Mr. J.D., considering the high-energy mechanism and comminuted nature, the soft tissue injury was considered severe (Tscherne C3 for closed injury, or Gustilo Type I/II if open wound found) even if the skin was intact pre-fasciotomy.
2.
Tscherne and Oestern Classification of Soft Tissue Injuries (for closed fractures):
This classification is primarily used for closed fractures to grade soft tissue injury.
*
C0:
No or minimal soft tissue injury.
*
C1:
Superficial abrasion or contusion.
*
C2:
Deep abrasion, muscle contusion, impending compartment syndrome.
*
C3:
Extensive skin contusion, severe muscle damage,
established compartment syndrome
, or vascular injury.
Mr. J.D.'s case clearly falls into
Tscherne C3
due to the established compartment syndrome and severe muscle damage. This classification underscores the severity of the soft tissue injury, which often dictates the urgency and complexity of surgical management beyond just the fracture itself.
Treatment Goals:
1. Decompression of all involved compartments to restore perfusion and prevent irreversible tissue damage.
2. Debridement of any necrotic tissue.
3. Stabilization of the underlying tibia fracture.
4. Minimizing complications such as infection, nerve injury, and chronic pain.
5. Facilitating limb salvage and functional recovery.
Surgical Technique / Intervention
Mr. J.D. was immediately transferred to the operating theatre for emergent four-compartment fasciotomy of the left lower leg and subsequent definitive fixation of his tibia fracture.
Patient Positioning:
The patient was placed supine on the operating table. The entire lower extremity from the ipsilateral iliac crest to the toes was prepped and draped in a sterile fashion. A pneumatic tourniquet was applied to the thigh but not inflated.
Surgical Approach – Dual Incision Fasciotomy:
The standard dual-incision approach was utilized for complete decompression of all four compartments of the lower leg.
-
Anterolateral Incision:
- A longitudinal incision was made, approximately 15-20 cm in length, midway between the tibial crest and the fibula, starting just distal to the fibular head and extending towards the ankle. This incision was made directly over the anterior intermuscular septum.
- Subcutaneous dissection: The incision was carried through skin and subcutaneous tissue. Careful hemostasis was achieved.
- Identification of Fascia: The fascia overlying the anterior compartment was identified.
- Anterior Compartment Fasciotomy: The fascia of the anterior compartment was incised longitudinally along its entire length, exposing the tibialis anterior, extensor digitorum longus, and extensor hallucis longus muscles. The deep peroneal nerve and anterior tibial artery/vein were carefully protected during this step. The muscles were observed to bulge upon release.
- Lateral Compartment Fasciotomy: Retraction of the skin flaps allowed visualization of the fascia over the lateral compartment (peroneus longus and brevis). This fascia was also incised longitudinally along its entire length, releasing the lateral compartment. Care was taken to identify and protect the superficial peroneal nerve, which typically courses superficially within this compartment, often piercing the fascia more distally.
-
Posteromedial Incision:
- A second longitudinal incision, also approximately 15-20 cm, was made approximately 2 cm posterior to the posteromedial border of the tibia. This avoided direct incision over the tibia and protected the saphenous vein and nerve anteriorly.
- Subcutaneous dissection: Incision through skin and subcutaneous tissue, again with careful hemostasis.
- Identification of Fascia: The fascia overlying the superficial posterior compartment (gastrocnemius and soleus muscles) was identified.
- Superficial Posterior Compartment Fasciotomy: The fascia was incised longitudinally along its entire length, releasing the superficial posterior compartment. The plantaris muscle was also identified and released if present.
- Deep Posterior Compartment Fasciotomy: The superficial posterior compartment muscles (gastrocnemius and soleus) were retracted posteriorly. The fascia overlying the deep posterior compartment (flexor digitorum longus, tibialis posterior, flexor hallucis longus) was identified. This fascia, often quite thick, was then incised longitudinally along its entire length. This step required careful identification and protection of the tibial nerve and posterior tibial artery/veins, which lie directly on the deep posterior compartment fascia. The muscles of the deep compartment were then observed to bulge.
Intraoperative Findings after Fasciotomy:
Upon release, significant muscle bulging was observed from all four compartments, particularly the anterior and lateral compartments. The muscle appeared dusky and edematous initially but quickly regained a healthier, redder color after decompression, indicating restoration of perfusion. No frank necrotic muscle was noted at this initial stage. The wounds were copiously irrigated.
Definitive Fixation of Tibia Fracture:
Following successful fasciotomy and confirmation of muscle viability, attention was turned to the comminuted mid-diaphyseal tibia fracture.
*
Debridement:
The fracture site was thoroughly debrided via a limited anterior approach, directly through one of the fasciotomy incisions if possible, or a separate small incision if necessary. All devitalized tissue and hematoma were removed. The wound was copiously irrigated with several liters of sterile saline.
*
Reduction Techniques:
Given the comminution, closed reduction was attempted using traction and fluoroscopic guidance.
*
Traction:
Distal traction was applied to the foot to achieve length.
*
Manual Manipulation:
Manual manipulation, often with external rotation to correct typical varus/apex anterior deformity, was used.
*
Blocking Screws (Optional):
If fluoroscopy revealed persistent malalignment during reaming, blocking screws (Poller screws) would be considered to guide the intramedullary nail into the central canal.
*
Fixation Construct – Reamed Intramedullary Nailing:
*
Entry Point:
A standard paratendinous approach was used to access the proximal tibia for nail insertion. A starting point just medial to the lateral tibial spine, in line with the intercondylar notch, was chosen to prevent apex anterior angulation.
*
Reaming:
Sequential reaming of the tibial canal was performed under fluoroscopic guidance to allow for insertion of an appropriately sized intramedullary nail. Reaming was done slowly and incrementally to minimize heat necrosis and fat embolization risk.
*
Nail Insertion:
A locked intramedullary tibial nail (e.g., Expert Tibia Nail, Synthes) was then inserted and advanced across the fracture site.
*
Distal Locking:
Distal locking screws were inserted under fluoroscopic guidance, typically in a static fashion to achieve rotational stability and maintain length.
*
Proximal Locking:
Proximal locking screws were inserted after ensuring optimal nail position and fracture reduction.
*
Final Assessment:
Final fluoroscopic images confirmed satisfactory fracture reduction, alignment, and stable fixation.
Wound Management:
The fasciotomy wounds were not primarily closed. They were packed loosely with saline-moistened sterile gauze and covered with sterile dressings. A vacuum-assisted closure (VAC) device was considered for later stages but not applied immediately to allow for further assessment of tissue viability. The decision for delayed primary closure, skin grafting, or secondary intention healing would be made in 48-72 hours.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (0-72 hours):
*
Wound Care:
The fasciotomy wounds were carefully monitored. Dressings were changed daily, and the wounds were assessed for signs of infection, further necrosis, or resolution of swelling. The limb was kept elevated to minimize edema.
*
Pain Management:
Aggressive multimodal analgesia, including opioid and non-opioid medications, was administered. Regional nerve blocks were considered.
*
Antibiotics:
Broad-spectrum intravenous antibiotics were continued for 24-48 hours post-operatively, particularly given the open nature of the fasciotomy wounds and the potential for a Gustilo-Anderson classification fracture.
*
Fluid and Electrolyte Management:
Monitoring for rhabdomyolysis sequelae, including acute kidney injury. Intravenous fluids were continued, and urine output monitored. Electrolytes, especially potassium, were closely watched.
*
Neurovascular Monitoring:
Regular checks of distal pulses, capillary refill, sensation, and motor function were performed.
*
Fracture Immobilization:
The limb was placed in a bulky soft dressing or a posterior splint for comfort and initial immobilization, although the IM nail provides inherent stability.
*
Second Look/Wound Closure:
Approximately 48-72 hours post-fasciotomy, Mr. J.D. was returned to the operating theatre for a "second look" procedure. At this stage, all wounds were thoroughly inspected. Any non-viable or necrotic muscle tissue was meticulously debrided. The viability of the remaining muscle and soft tissue dictated the next steps for wound closure.
*
Delayed Primary Closure:
If swelling had significantly resolved and skin edges could be approximated without tension, sutures, staples, or Steri-Strips were used for delayed primary closure.
*
Skin Grafting:
If skin loss or significant tension prevented primary closure, split-thickness skin grafting was planned.
*
VAC Therapy:
Vacuum-assisted closure (VAC) was considered to reduce wound size, promote granulation tissue, and prepare the wound bed for eventual grafting or delayed closure. For Mr. J.D., swelling had largely resolved, and the wounds were amenable to delayed primary closure with a few strategically placed sutures after the second look.
Early Rehabilitation (Days 3-14):
*
Weight Bearing:
Non-weight-bearing (NWB) on the operative limb, typically for 4-6 weeks, or as per the surgeon's discretion based on fracture stability and healing. Touch-down weight-bearing (TDWB) might be initiated earlier if fixation is robust and pain-controlled.
*
Range of Motion (ROM):
Active and passive range of motion exercises for the ankle and toes were initiated, usually with the guidance of a physiotherapist. Emphasis was placed on preventing ankle stiffness and Achilles tendon contracture.
*
Muscle Strengthening:
Gentle isometric exercises for the quadriceps and hip musculature were started.
*
Mobility:
Ambulation with crutches or a walker was taught, maintaining NWB on the operative limb.
Progressive Rehabilitation (Weeks 2-12):
*
Weight Bearing Progression:
Gradual progression to protected weight-bearing (PWB) and then full weight-bearing (FWB) was initiated based on clinical and radiographic signs of fracture healing (e.g., callus formation). This typically occurred between 6-12 weeks.
*
Intensified ROM and Strengthening:
More aggressive range of motion exercises, including ankle stretching and mobilization. Progressive resistance exercises for all muscle groups of the lower limb.
*
Proprioception and Balance Training:
Once partial weight-bearing was achieved, exercises to improve balance and proprioception were incorporated.
*
Scar Management:
Massage, silicone sheeting, or other modalities to manage fasciotomy scars and minimize contracture.
Long-term Rehabilitation (>12 weeks):
*
Return to Activity:
Gradual return to activities of daily living, work, and recreational activities as tolerated. Specific sports or high-impact activities might require several months of dedicated rehabilitation.
*
Monitoring for Complications:
Ongoing monitoring for chronic pain, persistent neurological deficits, muscle weakness, ankle stiffness, and the potential need for hardware removal (e.g., if symptomatic or for a second-stage procedure).
*
Psychological Support:
Acknowledging the significant physical and psychological impact of severe trauma and compartment syndrome, providing appropriate support and referrals where necessary.
Mr. J.D. progressed well, achieved delayed primary closure of his fasciotomy wounds, and began protected weight-bearing at 6 weeks. At 6 months post-injury, he had achieved full ankle ROM, satisfactory fracture healing, and was resuming light activities, albeit with some residual numbness in the first web space (deep peroneal nerve neuropathy) and mild weakness in ankle dorsiflexion, which is a common sequela.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
1.
High Index of Suspicion:
The single most crucial pearl. Compartment syndrome is a clinical diagnosis. Think of it in any high-energy trauma to the limb, especially tibia fractures, crush injuries, reperfusion injuries, or prolonged limb compression.
2.
Pain Out of Proportion:
This is often the earliest and most reliable sign. Don't be reassured by palpable pulses or a lack of pallor; arterial flow may be preserved while microcirculation in the muscle is compromised.
3.
Pain with Passive Stretch:
A highly sensitive and specific sign. Always perform this examination.
4.
Tense Compartments:
Palpate all four compartments firmly. A "wood-like" feel is pathognomonic.
5.
Neurological Deficits:
Paresthesias and motor weakness are relatively late signs, indicating significant nerve ischemia. Do not wait for these.
6.
"6 Ps" Revisited:
While classic, remember that Pulselessness and Pallor are
very late
signs, indicating irreversible damage or impending limb loss. The first three "Ps" (Pain out of proportion, Pain with passive stretch, Paresthesia) are the diagnostic cornerstones.
7.
Compartment Pressure Monitoring:
Indicated in equivocal cases, uncooperative patients (e.g., altered mental status, children), or when clinical examination is difficult. Use the delta pressure (Diastolic BP - Intracompartmental Pressure < 20-30 mmHg) as it accounts for patient's perfusion status.
8.
Time is Tissue:
Once diagnosed, fasciotomy is a surgical emergency. Every hour of delay increases morbidity. Do not wait for specific imaging (CT/MRI) or specialist consultation if you are able to perform the procedure.
9.
Complete Fasciotomy:
Ensure all involved compartments are released adequately. In the lower leg, this usually means a four-compartment fasciotomy via dual incisions. Incomplete release is a common cause of poor outcomes.
10.
Second Look:
Plan for a second look in 48-72 hours for debridement of any necrotic tissue and wound management (delayed closure, skin grafting, VAC).
11.
Associated Injuries:
Always look for and address associated injuries, especially fractures, after compartment decompression.
12.
Rhabdomyolysis Management:
Monitor CK levels, urine output, and electrolytes (especially K+) to prevent and manage acute kidney injury. Aggressive IV fluids are critical.
Pitfalls:
1.
Underestimation of Pain:
Dismissing patient's subjective pain ("drug-seeking," "over-reactive") is a dangerous pitfall.
2.
Reassurance by Palpable Pulses:
A palpable pulse does NOT rule out compartment syndrome. This is a common and critical misconception.
3.
Delay in Diagnosis/Treatment:
The most common cause of poor outcomes. Any hesitation once diagnosis is suspected can lead to irreversible damage.
4.
Inadequate Fasciotomy:
Not releasing all four compartments, or making incisions too short, too shallow, or misplacing them. Forgetting to release the deep posterior compartment is a common error.
5.
Failure to Debride Necrotic Muscle:
If left in situ, necrotic muscle can lead to infection and further systemic complications.
6.
Misinterpretation of Compartment Pressure Readings:
Relying solely on absolute pressure without considering the patient's diastolic blood pressure (delta pressure) can lead to missed diagnoses, especially in hypotensive patients.
7.
Premature Wound Closure:
Closing fasciotomy wounds under tension can lead to recurrent compartment syndrome or skin necrosis. Always plan for delayed closure.
8.
Nerve Injury during Fasciotomy:
The superficial peroneal nerve and saphenous nerve are at risk with lateral and medial incisions, respectively. The deep peroneal nerve, tibial nerve, and associated vessels are deep and must be protected.
9.
Focusing Only on the Fracture:
While important, the fracture is secondary to limb-threatening compartment syndrome. Prioritize life and limb over definitive fracture fixation.
10.
Lack of Awareness of Chronic Sequelae:
Persistent pain, weakness, numbness, contractures (e.g., Volkmann's), and psychological distress are common long-term issues that require ongoing management.
Understanding these pearls and pitfalls is essential for any orthopedic surgeon, resident, or medical student aspiring to provide optimal care for patients with acute compartment syndrome. Early diagnosis and timely, complete surgical intervention remain the cornerstones of successful management.
