Introduction & Epidemiology
Hip fractures represent a significant global health burden, primarily affecting the elderly population and carrying substantial morbidity and mortality. The incidence is projected to rise with an aging demographic, making their effective management a paramount orthopedic challenge. While internal fixation remains the preferred treatment modality for many hip fracture patterns, particularly in younger patients and specific stable fractures in the elderly, fixation failure remains a critical complication leading to revision surgery, prolonged recovery, and increased healthcare costs.
Fixation failure, encompassing implant cutout, migration, nonunion, malunion, and avascular necrosis (AVN), undermines the primary goal of restoring anatomical continuity and functional independence. Understanding and identifying the critical predictors of fixation failure are essential for optimizing patient selection, refining surgical techniques, and guiding post-operative management strategies. This review aims to consolidate current knowledge regarding the multifactorial nature of these predictors, ranging from patient-specific biological factors to biomechanical aspects of the fracture and technical nuances of surgical fixation.
Surgical Anatomy & Biomechanics
Effective internal fixation of hip fractures hinges upon a thorough understanding of the proximal femoral anatomy and its inherent biomechanical properties, particularly in the context of compromised bone quality.
Proximal Femoral Anatomy
The proximal femur comprises the femoral head, neck, and trochanteric regions.
*
Femoral Head:
Articulates with the acetabulum, supplied predominantly by retinacular vessels.
*
Femoral Neck:
Connects the head to the shaft, characterized by a dense cortical shell and intricate trabecular network. Its anteversion and valgus angulation are critical biomechanical features. Fractures here disrupt the primary weight-bearing trabeculae (medial compressive, lateral tensile) and blood supply.
*
Trochanteric Region:
The greater and lesser trochanters serve as attachment points for numerous hip musculature. The intertrochanteric region is largely cancellous, making it susceptible to comminution, especially in osteoporotic bone.
Blood Supply to the Femoral Head
The vascularity of the femoral head is critical, especially in femoral neck fractures. The primary supply is from the medial and lateral circumflex femoral arteries, which give rise to retinacular vessels ascending along the femoral neck within the capsule. Displacement of femoral neck fractures can disrupt these vessels, predisposing to AVN and subsequent collapse or nonunion.
Biomechanics of Fixation
The proximal femur is subjected to substantial bending, shear, and compressive forces during weight-bearing. Internal fixation constructs are designed to counteract these forces, providing stability until biological healing occurs.
*
Load Sharing:
Ideal constructs promote load sharing between the implant and the bone, minimizing stress shielding and allowing physiological stress stimulation for callus formation.
*
Bone Quality:
Osteoporosis significantly reduces bone mineral density and architectural integrity, decreasing the pullout strength of screws and the purchase of intramedullary nails. This is a primary predictor of cutout and fixation failure.
*
Fracture Pattern Stability:
*
Femoral Neck Fractures:
Instability is often related to displacement and comminution of the posterior cortex. Pauwels classification (angle of the fracture line to the horizontal) and Garden classification (degree of displacement and rotation) are critical. High Pauwels angles (Type III) and displaced Garden III/IV fractures inherently have higher shear forces and greater risk of nonunion or AVN.
*
Intertrochanteric Fractures:
Stability is determined by the integrity of the posteromedial cortex and the lesser trochanter. Comminution in these areas, particularly reverse obliquity patterns, converts primarily compressive forces into highly destabilizing shear forces, making standard sliding hip screws (SHS) prone to failure and often mandating intramedullary nail (IMN) fixation.
Indications & Contraindications
The decision between operative and non-operative management, and subsequently, the choice of implant, is multifactorial and heavily influences the risk of fixation failure.
Indications for Internal Fixation
Internal fixation is generally indicated for:
*
Displaced or Unstable Fractures:
Where non-operative management would lead to unacceptable deformity, pain, or nonunion.
*
Fractures in Physiologically Demanding Patients:
Younger, active individuals where restoration of near-anatomical function is paramount.
*
Certain Pathological Fractures:
To provide stability and pain relief.
Contraindications for Internal Fixation
Contraindications, often relative, include:
*
Severely Comminuted/Unreconstructible Fractures:
Where internal fixation is unlikely to achieve stable reduction or hold.
*
Pre-existing Severe Degenerative Joint Disease:
Arthroplasty may be preferred.
*
Significant Pre-existing Morbidities:
Rendering a lengthy or complex fixation procedure unsafe, or limiting post-operative rehabilitation capacity, thus increasing risk of failure.
*
Non-ambulatory Patients with Minimal Pain:
Sometimes, non-operative management or simpler procedures might be considered, though less common for hip fractures.
| Indication for Operative Fixation | Contraindication/Consideration for Non-Operative or Arthroplasty |
|---|---|
| Femoral Neck Fractures: | |
| Displaced (Garden III/IV) in younger patients (<60-65 years) | Highly comminuted/unreconstructible neck fracture |
| Non-displaced/impacted (Garden I/II) in all ages | Severe pre-existing coxarthrosis (consider arthroplasty) |
| Pauwels Type I/II | Elderly, low demand, medically unstable with non-displaced fracture (rare) |
| Intertrochanteric Fractures: | |
| All displaced or unstable patterns (AO/OTA 31-A2, 31-A3) | Severely comminuted, unfixable (consider arthroplasty if possible) |
| Stable patterns (AO/OTA 31-A1) | Extreme medical fragility, non-ambulatory, minimal pain (rare) |
| Reverse obliquity (IMN indicated) | |
| Subtrochanteric Fractures: | |
| All displaced or unstable patterns | Severe bone loss, pathological fracture not amenable to fixation |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is a cornerstone of preventing fixation failure. It involves a systematic assessment of the patient, the fracture, and the surgical strategy.
Patient Assessment
- Medical Optimization: Evaluate comorbidities (cardiac, pulmonary, renal, endocrine, nutritional status). Malnutrition, anemia, uncontrolled diabetes, and renal insufficiency are known predictors of poor bone healing and increased complication rates.
- Bone Health Assessment: Review medical history for osteoporosis, prior fragility fractures, or medications affecting bone metabolism. While formal BMD testing is rarely done acutely, clinical suspicion of severe osteoporosis influences implant choice and surgical technique.
- Functional Status: Assess pre-injury ambulation, cognitive function, and social support. These factors influence rehabilitation potential and compliance, indirectly affecting implant survival.
Fracture Assessment
-
Radiographic Analysis:
-
Plain Radiographs:
Anteroposterior (AP) pelvis and AP/lateral views of the injured hip are standard.
- Assess fracture pattern, displacement, comminution, and angulation.
- For femoral neck fractures: Garden classification (I-IV) and Pauwels angle (I-III) are critical for prognosis and implant choice.
- For intertrochanteric fractures: AO/OTA classification (31-A1, A2, A3) is used. Assess integrity of the posteromedial cortex, lesser trochanter, and presence of reverse obliquity.
- Computed Tomography (CT): Increasingly utilized for complex fractures, particularly to assess comminution, articular involvement, and guide implant choice. It can quantify bone quality (e.g., Hounsfield units) which correlates with osteoporotic bone.
-
Plain Radiographs:
Anteroposterior (AP) pelvis and AP/lateral views of the injured hip are standard.
-
Implant Selection:
Based on fracture pattern, bone quality, and surgeon preference.
- Femoral Neck: Cannulated screws (stable, non-displaced), sliding hip screw (SHS) with anti-rotation screw (select displaced, younger patients), or arthroplasty (displaced in elderly).
- Intertrochanteric: SHS (stable, A1/A2.1), Intramedullary Nail (IMN) (unstable, A2.2, A2.3, A3, reverse obliquity).
Surgical Plan
- Reduction Strategy: Determine the anticipated reduction maneuver (traction, internal/external rotation, abduction/adduction).
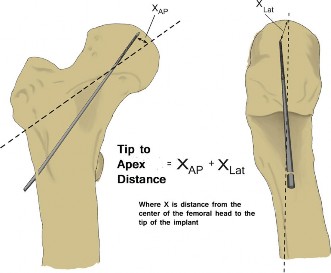
- Fixation Configuration: Plan screw trajectory, length, and position within the femoral head. For SHS/IMN, estimate tip-apex distance (TAD). Optimal TAD (<25mm, ideally <20mm) is a critical predictor of failure.
- Contingency Planning: Prepare for potential intraoperative challenges, such as difficult reduction or poor bone quality.
Patient Positioning
- Supine on Traction Table: Standard for most hip fracture fixations. Allows for controlled reduction with traction and manipulation, and simplifies fluoroscopic imaging.
- Lateral Decubitus: Less common for hip fractures, sometimes used for specific approaches or if a traction table is unavailable.
- Critical Considerations: Ensure adequate padding to prevent pressure injuries. C-arm access for both AP and lateral views must be unhindered. Maintaining sterility and access for draping.
Detailed Surgical Approach / Technique
Achieving stable and lasting fixation requires meticulous surgical technique, focusing on anatomical reduction and optimal implant placement. While specific techniques vary by fracture type and implant, certain principles universally apply to minimize fixation failure.
General Principles
-
Anatomical or Acceptable Reduction: This is arguably the most critical predictor of successful fixation. Poor reduction results in malalignment, increased stress on the implant, and impaired healing.
- Femoral Neck: Aim for anatomical reduction. For impacted or valgus-impacted fractures, maintain the impaction. For displaced fractures, gentle traction, internal rotation, and abduction/adduction maneuvers are used to restore alignment. Valgus reduction is often preferred over varus.
- Intertrochanteric: Achieve a stable reduction, ideally with restoration of the posteromedial buttress. A stable reduction often involves a slight valgus angulation and adequate restoration of femoral length and rotation. Avoid varus collapse.

An image demonstrating a comminuted intertrochanteric fracture with significant displacement. A suboptimal reduction, such as residual varus or inadequate restoration of the posteromedial buttress, significantly increases the risk of implant failure. -
Appropriate Implant Selection: Matching the implant to the fracture pattern and bone quality is paramount.
- Cannulated Screws (Femoral Neck): Typically 3 parallel screws. Indicated for stable, non-displaced, or valgus-impacted femoral neck fractures. Configuration (inverted triangle, diamond) should maximize purchase.
- Sliding Hip Screw (SHS) (Intertrochanteric): Consists of a lag screw inserted into the femoral head, a side plate, and cortical screws into the femoral shaft. Indicated for stable or reducible unstable intertrochanteric fractures (e.g., AO/OTA 31-A1, A2.1). The lag screw allows for controlled impaction at the fracture site.
- Intramedullary Nail (IMN) (Intertrochanteric, Subtrochanteric, Reverse Obliquity): Provides a more biomechanically favorable load-sharing construct, especially for unstable, comminuted, reverse obliquity, or subtrochanteric fractures. The nail acts as an internal splint, resisting bending and rotation.
-
Optimal Implant Placement: Correct positioning of the implant within the femoral head and neck is crucial to prevent cutout.
- Tip-Apex Distance (TAD): For SHS and IMN lag screws, the TAD is the sum of the distance from the tip of the lag screw to the apex of the femoral head on both AP and lateral radiographs, after accounting for magnification. A TAD > 25mm (ideally < 20mm) is strongly correlated with increased risk of cutout, particularly in osteoporotic bone. The lag screw should ideally be central or slightly inferior in the femoral head on the AP view and central in the lateral view.
- Screw Length and Trajectory (Cannulated Screws): Screws should engage the subchondral bone of the femoral head without penetrating the joint. The trajectory should maximize bone purchase and triangulate forces.
- Nail Entry Point (IMN): Correct entry point (piriformis fossa or greater trochanter tip) is critical to avoid iatrogenic fracture, malreduction, or subsequent biomechanical malalignment.
- Distal Locking: Ensures rotational stability and prevents shortening, especially in comminuted fractures.

An image depicting a post-operative radiograph of an intertrochanteric fracture fixed with an intramedullary nail. The lag screw demonstrates excellent placement within the femoral head, with an estimated Tip-Apex Distance (TAD) well within the acceptable range, and the nail is centrally placed within the femoral shaft. This optimal fixation minimizes the risk of implant cutout and nonunion.
Specific Surgical Techniques
1. Internal Fixation of Femoral Neck Fractures (Cannulated Screws)
- Approach: Lateral incision, typically 2-3 small incisions for percutaneous screw placement.
- Reduction: Performed under fluoroscopic guidance. Gentle traction, internal rotation to correct external rotation deformity, and abduction/adduction for varus/valgus alignment.
- Guide Wire Placement: Insert 3 guide wires, commonly in an inverted triangular pattern, ensuring good purchase in the femoral head and avoiding joint penetration. Ensure parallel or slightly converging trajectories.
- Screw Insertion: Measure lengths, drill, tap (if needed), and insert cannulated screws over the guide wires, leaving about 5mm from the subchondral bone.
- Assessment: Check AP and lateral views for screw position, length, and fracture reduction.
2. Fixation of Intertrochanteric Fractures (Sliding Hip Screw - SHS)
- Approach: Lateral incision over the proximal femur.
- Reduction: Traction, rotation, and potentially direct manipulation. Restore length, alignment, and rotation.
- Guide Wire Placement: Insert a guide wire from the lateral cortex, aiming for the center-inferior aspect of the femoral head on AP and central on lateral. Verify TAD.
- Barrel Reaming and Lag Screw Insertion: Ream over the guide wire, insert the lag screw. The screw should be fully seated with adequate bone purchase.
- Side Plate Application: Position the plate on the lateral femoral cortex, ensuring a snug fit and proper rotational alignment. Secure with cortical screws distally.
- Impaction: Allow for controlled impaction of the lag screw within the barrel to promote fracture site compression.
- Assessment: Fluoroscopic images (AP, lateral) for reduction, lag screw position, TAD, and plate alignment.
3. Fixation of Unstable Intertrochanteric/Subtrochanteric Fractures (Intramedullary Nail - IMN)
- Approach: Small incision over the greater trochanter.
- Entry Point: Critically important. Typically, the piriformis fossa or the tip of the greater trochanter, in line with the femoral canal. Incorrect entry (too medial or lateral) can lead to varus malalignment, iatrogenic fracture, or difficulty in distal locking.
- Reaming and Nail Insertion: Ream the femoral canal to the appropriate size. Insert the IMN, ensuring it passes the fracture site without displacing it.
- Lag Screw/Cephalic Screw Placement: Using targeting guides, insert the cephalic screw(s) into the femoral head. Optimal placement (TAD < 25mm, central on lateral, center-inferior on AP) is paramount.
- Distal Locking: Once the nail is seated and cephalic screws are in place, apply distal locking screws to prevent rotation and shortening. Ensure correct length and position.
- Assessment: Comprehensive fluoroscopic evaluation of reduction, nail position, cephalic screw placement, TAD, and distal locking.
Predictors of Fixation Failure Linked to Technique
- Poor Reduction: Varies collapse (varus malunion), rotational malunion, or persistent gap at the fracture site dramatically increases stress on the implant and reduces healing potential.
- High Tip-Apex Distance: Directly predicts cutout in SHS and IMN constructs.
- Eccentric Lag Screw Placement: Screws placed superiorly or inferiorly, or anteriorly/posteriorly within the femoral head.
- Lack of Bone Purchase: Screws too short or poorly engaged in osteoporotic bone.
- Inappropriate Implant Choice: Using an SHS for an unstable reverse obliquity fracture, or cannulated screws for a highly displaced femoral neck fracture in an elderly patient.
- Iatrogenic Comminution: During reaming or screw insertion, further weakening already compromised bone.
- Early Weight-Bearing on Unstable Fixation: Can lead to immediate implant failure.
Complications & Management
Fixation failure is a broad term encompassing several specific complications. Recognizing these, understanding their incidence, and having salvage strategies are crucial.
| Complication | Incidence (%) | Predictors (beyond general factors) | Salvage Strategy |
|---|---|---|---|
| Implant Cutout | 2-16% (SHS/IMN) | High TAD (>25mm), eccentric screw placement, osteoporotic bone, poor reduction (varus collapse), unstable fracture pattern. | Revision to IMN (if SHS failed), total hip arthroplasty (THA) or hemiarthroplasty (HHA) for femoral head collapse, Girdlestone resection arthroplasty (salvage for non-ambulatory). Often requires bone grafting or cement augmentation. |
| Nonunion/Pseudarthrosis | 5-30% (Femoral Neck); 2-5% (Intertrochanteric) | Femoral neck: Displaced fracture, inadequate reduction, AVN, poor blood supply, high Pauwels angle, insufficient fixation, younger age (high demand). Intertrochanteric: Severe comminution, excessive gap, inadequate stability, infection. | Femoral Neck: Revision internal fixation with bone grafting (younger patients, viable head), HHA/THA (elderly, failed fixation, AVN, or symptomatic nonunion). Intertrochanteric: Revision IMN or plate fixation with bone grafting, conversion to arthroplasty for select cases with severe pain and functional limitations. |
| Avascular Necrosis (AVN) of Femoral Head | 10-30% (Displaced Femoral Neck) | Displaced femoral neck fracture (Garden III/IV), delayed reduction/fixation, re-injury, intra-capsular hematoma. | Not directly a fixation failure but often leads to implant failure due to collapse. Management is typically THA or HHA once symptomatic collapse occurs. Core decompression for early-stage AVN, rarely done in the fracture setting. |
| Malunion | 5-15% | Inadequate reduction, unstable fracture, early weight-bearing on unstable fixation, technical errors. | Non-operative for asymptomatic malunion. Corrective osteotomy (complex, challenging) for symptomatic malunion (pain, gait disturbance, limb length discrepancy). Revision to arthroplasty if significant joint degeneration or pain. |
| Hardware Failure | <5% | Under-sizing of implant, poor implant quality (rare with modern implants), excessive loading on a non-healing fracture, stress riser from previous hardware. | Generally indicative of underlying nonunion or biomechanical failure. Requires revision surgery to address the underlying issue (e.g., nonunion) and replace/revise hardware. Often involves a different fixation strategy or conversion to arthroplasty. |
| Infection | 1-5% | Open fracture, prolonged surgery, poor surgical technique/sterility, patient comorbidities (diabetes, malnutrition). | Debridement, irrigation, cultures, antibiotic therapy, retention vs. removal of hardware (if stable fixation and early infection vs. unstable fixation or late infection). May require staged procedures or Girdlestone if severe. |
| Periprosthetic Fracture | 0.5-2% | Stress risers from existing hardware, revision surgery, bone fragility, subsequent trauma. | Depends on fracture pattern, stability of original implant. May require revision fixation (plate, cables, longer nail) or revision arthroplasty. |
General Management Principles for Fixation Failure
- Diagnosis: Thorough clinical evaluation, repeat radiographs (AP/lateral, potentially CT), and sometimes advanced imaging (MRI for AVN, bone scan for nonunion if early).
- Assessment of Cause: Determine whether failure is due to poor reduction, inadequate implant placement, biological nonunion, or progressive bone collapse. This guides salvage.
- Patient Factors: Re-evaluate patient's medical status, functional demands, and potential for further surgery and rehabilitation.
- Salvage Options: Range from revision internal fixation (with or without bone grafting) to conversion to arthroplasty (hemiarthroplasty or total hip arthroplasty) or, in extreme cases for non-ambulatory patients, Girdlestone resection arthroplasty.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation plays a crucial role in preventing fixation failure by allowing controlled loading, promoting bone healing, and restoring function. Protocols must be individualized based on fracture stability, quality of fixation, patient comorbidities, and cognitive status.
Initial Post-Operative Period (0-6 weeks)
- Pain Management: Crucial for early mobilization.
-
Mobilization:
- Stable Fixation (e.g., non-displaced femoral neck with cannulated screws, stable intertrochanteric with good IMN/SHS): Often allows for early weight-bearing as tolerated (WBAT) with assistive devices (walker, crutches). This promotes callus formation through physiological loading.
- Unstable Fixation (e.g., comminuted intertrochanteric, tenuous femoral neck fixation, poor bone quality): May require protected weight-bearing (toe-touch or partial weight-bearing) for a longer period (6-12 weeks) to prevent excessive stress on the healing fracture and implant. This decision is based on intraoperative stability assessment and post-operative radiographs.
- Range of Motion (ROM): Gentle active and passive ROM exercises for hip and knee to prevent stiffness and deep vein thrombosis (DVT).
- Muscle Strengthening: Isometric exercises for gluteal and quadriceps muscles.
- Fall Prevention: Education on fall prevention strategies is essential from day one.
Intermediate Phase (6-12 weeks)
- Progressive Weight-Bearing: Gradually increase weight-bearing as dictated by radiographic healing and clinical comfort. Full weight-bearing is typically achieved by 8-12 weeks for most stable fixations.
- Strengthening: Advance hip and core strengthening exercises (e.g., resisted abduction/adduction, hip extension).
- Gait Training: Focus on normal gait pattern, balance, and coordination.
- Occupational Therapy: Address activities of daily living (ADLs) and instrumental activities of daily living (IADLs).
Advanced Phase (Beyond 12 weeks)
- Return to Activity: Gradual return to pre-injury activities, avoiding high-impact sports until complete radiographic healing and strength recovery.
- Continued Strengthening and Conditioning: Address any residual deficits in strength, balance, and endurance.
- Bone Health Management: All patients, especially the elderly, should be evaluated for osteoporosis and initiated on appropriate medical therapy (e.g., bisphosphonates, calcium, vitamin D) to prevent future fragility fractures. This is a critical long-term strategy to reduce the risk of subsequent fixation failure or new fractures.
Predictors of Poor Rehabilitation Outcome/Secondary Fixation Failure
- Inadequate Pain Control: Limits participation.
- Poor Patient Compliance: Due to cognitive impairment, lack of social support, or non-adherence to protocols.
- Delayed Weight-Bearing: While sometimes necessary for unstable fractures, prolonged non-weight-bearing can lead to muscle atrophy, joint stiffness, and disuse osteopenia, hindering recovery.
- Early, Uncontrolled Weight-Bearing: On an unstable construct is a direct cause of implant cutout or fracture collapse.
- Unaddressed Osteoporosis: Persisting low bone density increases the risk of refracture or failure of the initial fixation.
Summary of Key Literature / Guidelines
The literature consistently highlights a confluence of patient, fracture, and surgical factors as critical predictors of fixation failure in hip fractures.
Patient-Related Predictors
- Osteoporosis/Low Bone Mineral Density: Universally acknowledged as the most significant patient-related risk factor for implant cutout and nonunion. Studies often show higher rates of failure in patients with T-scores indicative of osteoporosis or low Hounsfield units on CT scans.
- Advanced Age: Correlates with poorer bone quality and increased comorbidities, leading to higher failure rates.
- Comorbidities: Conditions such as diabetes mellitus, chronic renal failure, malnutrition (low albumin), smoking, and chronic corticosteroid use impair bone healing and increase infection risk, contributing to fixation failure.
- Cognitive Impairment: Affects patient compliance with weight-bearing restrictions and rehabilitation protocols, indirectly increasing failure risk.
Fracture-Related Predictors
-
Fracture Pattern Instability:
- Femoral Neck: Displaced Garden III/IV fractures, high Pauwels angle (>50-70 degrees), posterior comminution, and vertical shear patterns significantly increase the risk of nonunion and AVN, leading to fixation failure.
- Intertrochanteric: Comminution of the posteromedial cortex, involvement of the lesser trochanter, and reverse obliquity patterns (AO/OTA 31-A3) create inherent instability, predisposing to varus collapse and implant cutout, especially with SHS. IMNs are generally superior for these unstable patterns.
- Degree of Displacement: Directly impacts the disruption of blood supply (femoral neck) and the difficulty of achieving a stable reduction.
Surgical/Technical Predictors
- Quality of Reduction: Poor reduction, particularly residual varus angulation, is a paramount predictor of failure across all hip fracture types. Anatomic or acceptable reduction (e.g., valgus impaction) is associated with significantly lower failure rates.
-
Implant Position:
- Tip-Apex Distance (TAD): The most consistently reported surgical predictor for SHS and IMN. A TAD > 25mm (some literature suggests >20mm) is strongly associated with implant cutout. Optimal placement is central or inferior-central in the femoral head.
- Eccentric Lag Screw/Cephalic Screw Placement: Placement too superior, anterior, or posterior in the femoral head results in poor purchase and increased stress concentration, leading to cutout.
- Implant Choice: Using an inappropriate implant for the fracture pattern (e.g., SHS for reverse obliquity intertrochanteric fractures, or cannulated screws for highly displaced femoral neck fractures in the elderly with poor bone quality) is a recognized predictor of failure.
- Surgical Experience: While less formally quantified, surgeon experience and adherence to established principles are implied factors in achieving optimal reduction and fixation.
Key Guidelines and Recommendations
- Geriatric Fracture Centers: Multidisciplinary approach to optimize patient health, reduce surgical delay, and improve outcomes.
- Early Surgical Intervention: For displaced femoral neck fractures, reduction and fixation within 24-48 hours may reduce the risk of AVN.
- Intramedullary Nailing for Unstable IT Fractures: Strong recommendation for unstable (AO/OTA 31-A2.2, A2.3, A3) and subtrochanteric fractures.
- Arthroplasty for Displaced Femoral Neck Fractures in the Elderly: Hemiarthroplasty or THA often preferred over internal fixation due to high rates of re-operation from nonunion or AVN.
- Bone Health Optimization: Routine screening and management of osteoporosis in all fragility fracture patients.
In conclusion, preventing fixation failure in hip fractures requires a holistic approach that integrates careful pre-operative planning, meticulous surgical technique prioritizing stable reduction and optimal implant placement (especially considering TAD), appropriate implant selection for the fracture pattern and bone quality, and vigilant post-operative management including bone health optimization. Understanding and proactively addressing these critical predictors significantly improve patient outcomes and reduce the burden of revision surgery.
Clinical & Radiographic Imaging