INTRODUCTION TO CARPAL INSTABILITY AND LIGAMENT RECONSTRUCTION
Carpal instability represents a complex biomechanical failure of the wrist, most frequently manifesting as scapholunate dissociation (SLD) or lunotriquetral (LT) instability. The carpus functions as an intricate intercalated segment between the radius and the metacarpals, relying entirely on its capsuloligamentous constraints for stability. When the scapholunate interosseous ligament (SLIL) is disrupted, the scaphoid inherently flexes while the lunate extends with the triquetrum, resulting in a Dorsal Intercalated Segment Instability (DISI) deformity. Conversely, failure of the lunotriquetral ligament allows the lunate to flex with the scaphoid, producing a Volar Intercalated Segment Instability (VISI) pattern.
Ligament reconstruction is indicated in patients with symptomatic, reducible dynamic or static carpal instability who have not yet developed advanced degenerative changes (e.g., Scapholunate Advanced Collapse [SLAC]). The primary goal of these procedures is to restore the kinematic linkage of the proximal carpal row, correct rotatory subluxation of the scaphoid, and halt the progression of arthrosis.
This masterclass details the most prominent historical and contemporary techniques for carpal ligament reconstruction, including the Almquist four-bone reconstruction, the Brunelli tenodesis, Taleisnik’s modifications, and the Blatt capsulodesis.
PREOPERATIVE PLANNING AND POSITIONING
Meticulous preoperative planning is essential. Standard posteroanterior (PA), lateral, and specialized views (e.g., clenched fist, ulnar deviation) must be evaluated to assess the reducible nature of the deformity and rule out fixed arthritic changes.
💡 Clinical Pearl
Ligament reconstruction is strictly contraindicated in the presence of fixed carpal deformities or established radiocarpal/midcarpal arthritis. In such cases, salvage procedures such as proximal row carpectomy (PRC) or partial wrist arthrodesis are the treatments of choice.
Patient Positioning:
1. Place the patient supine on the operating table.
2. Extend the operative arm onto a radiolucent hand table.
3. Apply a well-padded pneumatic tourniquet to the proximal arm.
4. Utilize intraoperative fluoroscopy to confirm carpal reduction and hardware placement dynamically.
THE ALMQUIST ET AL. RECONSTRUCTION TECHNIQUE
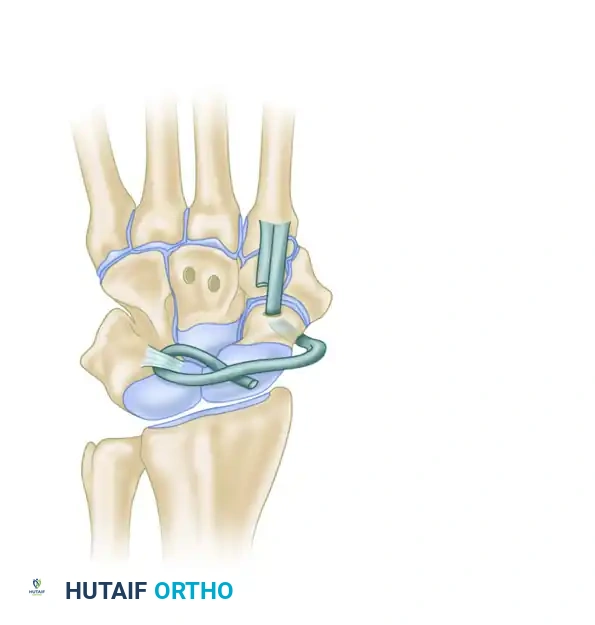
The Almquist technique is a robust, combined dorsal and palmar approach that utilizes a split tendon graft (typically the extensor carpi radialis brevis [ECRB]) routed through the capitate, lunate, scaphoid, and distal radius to recreate the complex multidirectional stability of the carpus.
Surgical Approach and Exposure
- Dorsal Incision: Make a straight dorsal longitudinal incision centered over the fourth dorsal compartment.
- Retinaculum Reflection: Carefully reflect the extensor retinaculum radially, elevating it from the fifth compartment toward the third compartment. Leave the retinaculum attached at its radial margin to serve as a robust closure layer later.
- Neurectomy: Identify and divide the terminal end of the posterior interosseous nerve (PIN) proximal to the wrist joint. This prophylactic denervation significantly reduces postoperative dorsal wrist pain.
- Capsulotomy: Open the dorsal wrist capsule longitudinally to expose the proximal carpal row (scaphoid, lunate) and the capitate.
- Palmar Incision: Make a separate palmar incision parallel to the thenar crease. Extend it proximally in a zigzag fashion several centimeters proximal to the wrist flexion crease to expose the palmar capsule.
Bone Tunnel Preparation
⚠️ Surgical Warning
When penetrating the palmar capsule, do so sharply and avoid excessive stripping. Stripping the palmar capsule compromises the critical radioscaphocapitate (RSC) and long radiolunate (LRL) ligaments, which are essential for secondary carpal stability.
- Drilling the Carpus: Drill small holes from dorsal to palmar in the proximal neck of the capitate, the nonarticular surface of the lunate, and the nonarticular proximal pole of the scaphoid. These tunnels should be positioned 5 to 7 mm from the proximal articular surfaces to prevent intra-articular fracture or cartilage damage.
- Reduction: Manually reduce the rotary subluxation of the scaphoid and correct the DISI deformity before passing the drill through the palmar capsule.
- Guidance and Enlargement: To avoid malpositioning, initially use a Kirschner wire (K-wire) as a guide. Once the trajectory is confirmed fluoroscopically, enlarge the drill holes to approximately 3.5 mm using a larger drill, burr, or curette. The tunnels must be smooth and large enough to accommodate the tendon graft without shredding it.
Graft Harvest and Routing
- Tendon Preparation: Extend the dorsal incision proximally along the course of the radial wrist extensors. Split the ECRB tendon in half by cutting into its musculotendinous junction and stripping it distally to its insertion at the base of the third metacarpal. If the ECRB musculotendinous junction is too far distal, the extensor carpi radialis longus (ECRL) tendon may be used instead.
- Suture Tagging: Pass a locking zigzag (Krakow-style) suture into the free proximal end of the harvested tendon slip.
- Carpal Fixation: Pass a 22-gauge stainless steel wire through the holes in the scaphoid and lunate. Use a wire tightener to secure the loop dorsally. This internal wire loop reduces scaphoid rotation and firmly secures the scaphoid and lunate together during the healing phase.
- Tendon Passing: Use another loop of 22-gauge wire as a tendon passer. Pass this loop from palmar to dorsal through the capitate tunnel to retrieve the tagged ECRB tendon.
- Routing Sequence:
- Pull the tendon from dorsal to palmar through the capitate, exiting through the palmar capsule into the carpal canal.
- Thread the tendon through the palmar surface of the lunate, exiting dorsally.
- Route it over to the scaphoid, passing dorsally through the scaphoid tunnel and exiting its palmar surface. Ensure this is done outside the capsule without stripping it.
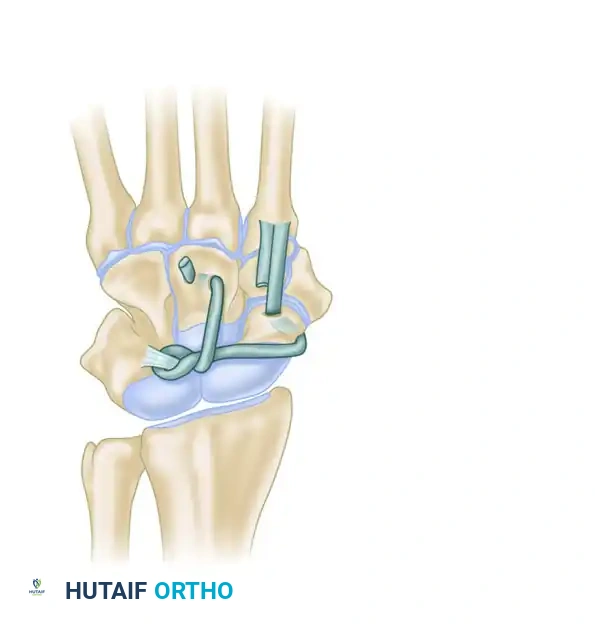
Radial Tethering and Closure
- Radial Preparation: Expose the palmar surface of the distal radius on the ulnar side of the scaphoid's exit hole. This positioning is critical to tether the proximal pole of the scaphoid in an ulnar direction, counteracting its natural tendency to subluxate radially and flex.
- Radial Tunnel: Drill a hole in the radius from the palmar surface, exiting dorsally into the fourth dorsal compartment. Enlarge it to allow free tendon passage.
- Final Tensioning: Pass the tendon from palmar to dorsal through the radius. Pull the graft as taut as possible while maintaining carpal reduction. Suture the tendon dorsally to the periosteum, the dorsal capsule, and the palmar capsule using robust nonabsorbable sutures.
- Closure: Repair the dorsal capsule, reposition and repair the extensor retinaculum, and close the skin in layers. Apply a nonadherent dressing and a rigid long-arm splint.
THE BRUNELLI AND BRUNELLI TECHNIQUE
The Brunelli technique is a cornerstone of scapholunate reconstruction. It utilizes a distally based slip of the flexor carpi radialis (FCR) tendon, routed through the distal pole of the scaphoid, to act as a dynamic tenodesis that prevents scaphoid flexion and rotary subluxation.
Surgical Approach
- Dorsal Exposure: With the patient supine and tourniquet inflated, make a straight 4-cm longitudinal dorsal incision. Section and reflect the extensor retinaculum.
- Arthrotomy: Enter the wrist joint via a longitudinal capsular incision between the ECRB and the extensor pollicis longus (EPL) tendons.
- Debridement: Incise the capsuloligamentous remnants between the scaphoid and lunate. Meticulously excise scar tissue in the SL interval, strictly sparing the articular cartilage.
- STT Joint Release: Identify the scaphotrapeziotrapezoid (STT) joint distal to the scaphoid. Excise any capsular scarring or thickening in this region to mobilize the scaphoid and allow for anatomic reduction.
FCR Harvest and Scaphoid Tunnel
- Palmar Exposure: Make a palmar skin incision over the FCR tendon.
- Surgical Warning: Exercise extreme caution to avoid injury to the radial artery, the median nerve, and the palmar cutaneous branch of the median nerve. Enter the wrist strictly through the FCR sheath.
- Interval Clearing: Remove scar tissue between the scaphoid and lunate from the palmar aspect so that the interval is clearly visualized from dorsal to palmar.
- Tendon Splitting: Incise the FCR sheath down to the trapezium and trapezoid, preserving its deep insertion at the base of the second metacarpal. Split the FCR tendon longitudinally, harvesting a 7-cm slip that remains attached distally.
- Scaphoid Drilling: Drill a small hole in the distal pole of the scaphoid, parallel to its distal articular surface. Enlarge this tunnel to approximately 2.5 mm in diameter.
Tendon Routing and Fixation
- Passing the Graft: Pass the FCR tendon slip from palmar to dorsal through the prepared scaphoid tunnel.
- Reduction: Pull the tendon slip dorsally and proximally. This vector effectively reduces the scaphoid, correcting the proximal pole subluxation and closing the scapholunate gap.
- K-Wire Fixation: Temporarily fix the anatomically reduced scaphoid using a K-wire driven from the distal scaphoid into the capitate or lunate.
- Anchoring: Suture the tendon slip securely to the fibrous remnant of the dorsal scapholunate ligament on the lunate, and then anchor it to the robust fibrous tissue at the dorsoulnar margin of the distal radius.
- Closure: Close the capsular incisions and skin. Apply a nonadherent dressing and a sugar-tong splint.
TALEISNIK AND LINSCHEID MODIFICATIONS
Taleisnik and Linscheid expanded upon these principles to address specific patterns of carpal instability, utilizing different tendon grafts based on the biomechanical deficit.
Triquetrolunate Instability (VISI)
For lunate stabilization in patients with triquetrolunate instability (which presents as a static VISI or dynamic DISI collapse pattern contributing to medial carpal instability), Taleisnik recommended utilizing the flexor carpi ulnaris (FCU).
* Technique: The lateral half of the FCU is harvested as a strip, left attached distally at the pisiform. It is threaded from the palm, passed through to the dorsal aspect of the lunate, and secured to the dorsal surface of the distal radius. This vector counteracts the abnormal flexion of the lunate seen in VISI deformities.
Dynamic DISI Deformities
For dynamic DISI deformities where the scaphoid requires stabilization against abnormal flexion:
* Technique: The medial half of the ECRB is left attached distally at the third metacarpal. It is threaded through the lunate from dorsal to palmar and anchored under the pronator quadratus on the anterior surface of the distal radius.
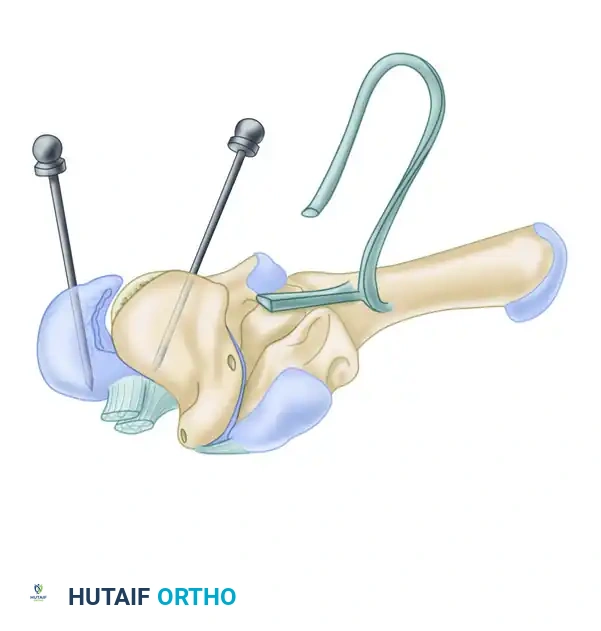
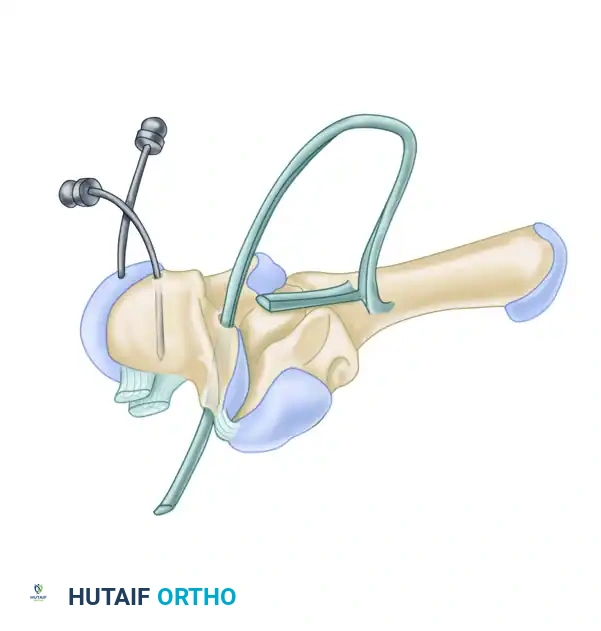
Ligamentous Augmentation (Figure 69-91)
In cases of scaphotrapezial laxity combined with SLD, a strip of ECRL can be utilized.
1. The ECRL strip is passed through a drill hole directed through the scaphoid tuberosity.
2. The tendon is pulled through the hole and passed into the joint capsule over the scaphoid waist.
3. It is then passed through the dorsal aspect of the lunotriquetral ligament using a tendon passer.
4. Finally, it is looped under itself and passed distally into a hole in the capitate.
5. This line of pull depresses the proximal pole of the scaphoid, elevates the distal pole (correcting rotatory subluxation), and rotates the lunotriquetral joint into flexion.
BLATT DORSAL CAPSULODESIS
Blatt described a highly effective, albeit non-anatomic, capsulodesis technique useful for two primary conditions causing wrist impairment: scapholunate dissociation and caput ulnae syndrome caused by distal radioulnar joint (DRUJ) incongruity.
💡 Clinical Pearl
Blatt’s capsulodesis is particularly valuable in patients with symptomatic dynamic instability or a reducible static deformity. It relies on creating a robust dorsal tether to prevent the scaphoid from flexing abnormally.
Key Steps:
1. A proximally based flap of the dorsal wrist capsule (incorporating the dorsal intercarpal ligament) is elevated.
2. The scaphoid is anatomically reduced and pinned with K-wires.
3. A trough is created in the dorsal cortex of the distal pole of the scaphoid.
4. The capsular flap is inserted into this trough and secured with suture anchors or transosseous sutures.
5. This creates a strong dorsal checkrein that prevents the scaphoid from rotating into flexion, thereby maintaining the reduction of the SL interval.
POSTOPERATIVE CARE AND REHABILITATION
The success of carpal ligament reconstruction relies heavily on strict adherence to postoperative immobilization protocols to allow for biologic incorporation of the tendon grafts and capsular healing.
Almquist Protocol:
* 0-10 Days: The patient is immobilized in a rigid long-arm splint. Sutures are removed at 7 to 10 days.
* 1-8 Weeks: A long-arm cast is applied and worn for an additional 7 weeks to neutralize forearm rotation, which places stress on the carpal ligaments.
* 8-12 Weeks: The cast is removed. A removable long-arm plaster or custom thermoplastic splint is applied. The splint is worn at all times except during controlled, active range-of-motion (ROM) exercises.
* 12-16 Weeks: The patient is transitioned to a short-arm splint.
* 16+ Weeks: Resistive exercises are initiated and progressively advanced to full strengthening.
Brunelli Protocol:
* 0-10 Days: Immobilization in a sugar-tong splint. Wound inspection and suture removal at 7 to 10 days.
* 1-4 Weeks: A solid sugar-tong cast is applied.
* 4 Weeks: The cast and the temporary K-wires are removed in the clinic. Active mobilization of the wrist is initiated under the guidance of a certified hand therapist, utilizing a short-arm plastic splint between sessions.
* 8-9 Weeks: Gentle resistive exercises are introduced.
* 10-12 Weeks: Progression to advanced strengthening and proprioceptive re-education. Return to heavy manual labor or contact sports is typically delayed until 5 to 6 months postoperatively.
Complications and Pitfalls
Surgeons must counsel patients regarding the expected loss of terminal wrist flexion and extension, which is an inherent trade-off for achieving carpal stability. Complications include hardware failure (K-wire breakage or migration), graft rupture, infection, and the eventual progression to radiocarpal arthrosis if the reduction is lost. Meticulous surgical technique, particularly avoiding thermal necrosis during drilling and ensuring isometric graft tensioning, is paramount to minimizing these risks.
