INTRODUCTION TO MEDIAL MALLEOLAR NONUNION
Nonunion of the medial malleolus is a complex orthopedic challenge that compromises the stability and congruity of the talocrural joint. The medial malleolus serves as the primary buttress against medial talar shift and is the critical attachment site for the deltoid ligament complex. When a fracture in this region fails to unite, the persistent shear forces, combined with the intrusion of synovial fluid into the fracture gap, severely inhibit osteogenesis.
Surgical intervention is definitively indicated for symptomatic nonunions, progressive valgus deformity, or impending post-traumatic osteoarthritis. The primary goals of operative management are to eradicate fibrous pseudarthrosis, restore vital osteoinductive and osteoconductive properties through autologous bone grafting, and achieve absolute stability via rigid internal fixation.
This masterclass details the highly effective Banks technique for bone grafting medial malleolar nonunions, advanced biological augmentation strategies, and the critical role of partial fibulectomy in managing concurrent tibial shaft nonunions.
PREOPERATIVE EVALUATION AND BIOMECHANICS
Clinical Presentation
Patients typically present with chronic medial-sided ankle pain, localized swelling, and a persistent limp. Weight-bearing exacerbates the symptoms due to dynamic instability. Clinical examination often reveals point tenderness over the medial malleolus and pain with passive eversion of the hindfoot, which places tension on the deltoid ligament and the ununited fragment.
Radiographic Assessment
Standard weight-bearing anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory. A nonunion is radiographically defined by the persistence of a radiolucent fracture line, sclerotic fracture margins, and the absence of bridging trabeculae at least six months post-injury.
Clinical Pearl: Preoperative computed tomography (CT) is highly recommended. A CT scan provides a three-dimensional understanding of the nonunion morphology, the exact size of the distal fragment, and the presence of any intra-articular step-off or cystic changes, which are critical for preoperative templating.
SURGICAL TECHNIQUE: BONE GRAFTING OF MEDIAL MALLEOLAR NONUNION (BANKS TECHNIQUE)
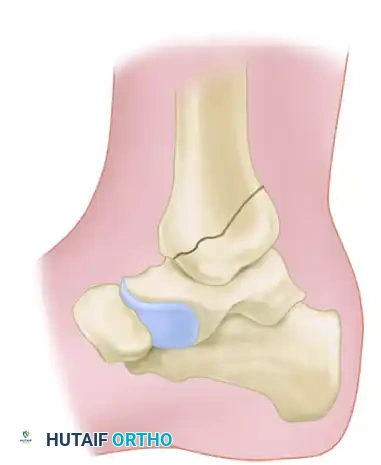
The Banks technique is a meticulously designed procedure that involves creating a wedge-shaped defect at the nonunion site, preserving the articular cartilage, and packing the defect with autologous cancellous bone harvested from the proximal tibial metaphysis.
1. Positioning and Anesthesia
The patient is placed in the supine position on a radiolucent operating table. General or regional anesthesia is administered. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field. The ipsilateral iliac crest should be prepped and draped in the event that a larger volume of structural bone graft is required, though the primary harvest site is the ipsilateral tibia.
2. Surgical Approach and Exposure
A medial longitudinal incision, approximately 10 cm in length, is made centered over the medial malleolus.
Careful subcutaneous dissection is performed to identify and protect the great saphenous vein and the saphenous nerve, which typically run anterior to the medial malleolus. The incision is carried down through the periosteum, and full-thickness flaps are elevated to expose the nonunion site.
3. Preparation of the Nonunion Site
The fibrous tissue interposed between the fracture fragments is meticulously excised using a combination of curettes and a surgical scalpel.

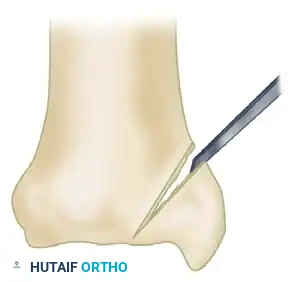
Once the nonunion is debrided, the sclerotic bone ends must be freshened to expose healthy, bleeding bone. Using a sharp osteotome or a high-speed burr, bone is removed to create a wedge-shaped defect.
Surgical Warning: The apex of this wedge must be directed precisely toward the articular surface of the ankle joint. It is imperative that damage to the articular cartilage is minimized or completely avoided. Preserving the articular hinge maintains joint congruity while allowing access for the graft.
4. Harvesting the Cancellous Bone Graft
To obtain the necessary autologous graft, a window is created in the tibial metaphysis at the proximal extent of the surgical wound.
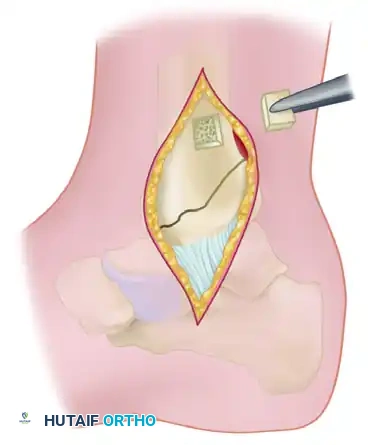
Using a thin osteotome or an oscillating saw, a square piece of cortical bone is removed.
* Technique Tip: The edges of this cortical window should be undercut. This allows the cortical piece to be securely replaced later, acting like a "manhole cover" that will not fall into the medullary canal.
* Through this window, a curette is used to harvest a generous amount of cancellous bone from the distal tibial metaphysis.
5. Reduction, Fixation, and Grafting
The medial malleolar fragment is restored to its anatomical position. It is held gently but securely with a pointed reduction forceps (towel clip).

The defect at the nonunion site is densely packed with the harvested cancellous bone. The osteoinductive and osteoconductive properties of this autograft are essential for bridging the pseudarthrosis.
Once the graft is packed, the fragment is rigidly fixed. A 4.5 mm partially threaded cancellous lag screw (typically 4.5 cm in length) is inserted from the tip of the medial malleolus, directed proximally and slightly laterally into the dense metaphyseal bone of the tibia. This provides interfragmentary compression across the grafted nonunion site.
Finally, the cortical piece is replaced over the metaphyseal window, and the wound is closed in layers.
ADVANCED BIOLOGICAL AUGMENTATION: MASQUELET TECHNIQUE AND RIA
In cases of recalcitrant nonunion, particularly those complicated by previous infection or massive bone loss, advanced biological reconstruction is required.
The Induced Membrane (Masquelet) Technique
If active infection is suspected or confirmed, a two-stage approach is mandatory:
1. Stage One: The bone and surrounding soft tissues are aggressively debrided and irrigated. An antibiotic-impregnated polymethylmethacrylate (PMMA) spacer is inserted into the bone defect. This spacer sterilizes the field and induces the formation of a highly vascularized, growth-factor-rich pseudosynovial membrane.
2. Stage Two: Once the soft tissue envelope has healed (typically 6 to 8 weeks later), a second operation is performed. The PMMA spacer is carefully removed, preserving the induced membrane.
Reamer-Irrigator-Aspirator (RIA) and rh-BMP2
To fill large defects within the induced membrane, copious amounts of bone graft are required, often exceeding what can be harvested from the iliac crest.
* RIA Harvest: Reaming of the ipsilateral femur using a Reamer-Irrigator-Aspirator (RIA) device provides a massive volume of highly osteogenic graft material. This can be performed in a retrograde fashion through the same incision used for an intramedullary tibial nail.
* Biologic Adjuvants: The addition of commercially available recombinant human Bone Morphogenetic Protein-2 (rh-BMP2) can be utilized for potent osteoinductive augmentation, significantly enhancing the rate of bone repair.
PARTIAL FIBULECTOMY AND WEIGHT BEARING IN TIBIAL NONUNION
When managing tibial fractures and nonunions, the biomechanical status of the fibula must always be considered. The fibula and tibia act as a coupled biomechanical system.
Biomechanics of the Fibular Strut
When both the tibia and fibula are fractured, the fibula—due to its smaller diameter and robust muscular envelope—almost always heals first. Once healed, the intact fibula becomes a load-sharing structure. It acts as a rigid strut that decreases axial loading across the healing tibia.
If the tibia has not yet united, this intact fibula prevents the close apposition of the tibial fracture fragments. Without axial compression (Wolff's Law), the tibial fracture site experiences strain environments conducive to fibrous tissue formation rather than primary or secondary bone healing, leading to nonunion.
Indications and Advantages of Partial Fibulectomy
Partial fibulectomy is indicated to destabilize the fibular strut, allowing the tibia to dynamically compress under weight-bearing loads. Sørensen outlined four distinct advantages to this technique:
1. Technical Simplicity: It is a straightforward, low-morbidity procedure.
2. Correction of Malposition: It allows for the closed correction of minor angular deformities.
3. Preservation of Biology: It avoids opening the primary tibial fracture site, thereby decreasing the risks of deep infection and preserving the fragile vascular supply to the nonunion fragments.
4. Future Options: It does not burn bridges; it allows for later bone grafting with or without internal fixation if union still fails to occur.
Clinical studies report successful healing in approximately 77% of patients with tibial nonunions treated with partial fibulectomy alone.
Pitfalls and Causes of Failure: Failure of the tibia to unite after partial fibulectomy is strongly associated with:
* Failure of the patient to comply with postoperative weight-bearing protocols.
* The presence of a true, synovial-lined pseudarthrosis (which requires open debridement).
* Previous prolonged treatment of the initial fracture with rigid external fixation, which may have severely compromised local biology.
Surgical Technique for Partial Fibulectomy
The surgical technique is highly effective and complications are rare when executed correctly.
* An incision is made over the middle to distal third of the fibula, avoiding the superficial peroneal nerve.
* A full-thickness segment of the fibula must be resected.
* Critical Dimension: The resected segment should be approximately 2.5 cm long. Removal of a smaller segment is a common technical error; it may allow the fibula to heal prematurely before the tibia has achieved solid union, recreating the strut effect.

Preoperative radiograph demonstrating a recalcitrant nonunion after osteotomy. The intact fibula is preventing axial compression of the tibia.

Radiograph showing failure to produce union by a sliding inlay graft. Note that the fibula remains intact, acting as a load-bearing strut and preventing tibial apposition.
Post-Resection Alignment
Immediately following the fibular resection, the tibia must be carefully aligned by closed manipulation. Because the lateral buttress has been removed, there is a risk of the tibia collapsing into a varus deformity.

Four years after the application of dual onlay grafts and osteotomy of the fibula. Note that the fibula now overlaps, allowing the tibia to compress and heal.

Final radiographic follow-up demonstrating solid union of the tibial shaft following successful fibular release and grafting.
POSTOPERATIVE CARE AND REHABILITATION
Medial Malleolar Grafting Post-Op
Postoperative care for the Banks technique mirrors that of a sliding graft.
* The ankle is immobilized in a well-padded short-leg cast or rigid splint in neutral dorsiflexion.
* The patient is kept strictly non-weight-bearing for the first 4 to 6 weeks to allow the cancellous graft to incorporate and prevent shear failure of the lag screw.
* At 6 weeks, radiographs are obtained. If early consolidation is visible, the patient is transitioned to a controlled ankle motion (CAM) boot and begins progressive partial weight-bearing, alongside active range-of-motion (ROM) exercises.
Partial Fibulectomy Post-Op
The postoperative protocol for partial fibulectomy relies heavily on mechanical loading.
* A straight long-leg walking cast is applied postoperatively to control angular alignment (preventing varus).
* The cast is worn for 6 weeks.
* Full weight-bearing is strongly encouraged immediately as tolerated. The axial load is the primary catalyst for osteogenesis at the tibial nonunion site.
CONCLUSION
The management of medial malleolar and tibial nonunions requires a profound understanding of lower extremity biomechanics and bone healing biology. The Banks technique provides an elegant, joint-sparing method to deliver vital cancellous autograft to the medial malleolus while achieving rigid compression. Concurrently, recognizing the inhibitory strut effect of an intact fibula is paramount; a strategically executed 2.5 cm partial fibulectomy can restore axial loading and reliably stimulate tibial union. Mastery of these techniques, combined with strict adherence to postoperative weight-bearing protocols, ensures optimal functional recovery for patients suffering from these debilitating nonunions.
