-
Atlas Fractures
- These are rarely associated with neurologic injury.
- Instability invariably equates to the presence of transverse alar ligament insufficiency, which can be diagnosed either by direct means, such as by identifying bony avulsion on CT scan or ligament rupture on MRI, or indirectly by identifying widening of the lateral masses.
- Fifty percent of these injuries are associated with other cervical spine fractures, especially odontoid fractures and spondylolisthesis of the axis.
- Cranial nerve lesions of VI to XII and neurapraxia of the suboccipital and greater occipital nerves may be associated.
- Vertebral artery injuries may cause symptoms of basilar insufficiency such as vertigo, blurred vision, and nystagmus.
- Patients may present with neck pain and a subjective feeling of “instability.”
- The mechanism of injury is axial compression with elements of hyperextension and asymmetric loading of condyles causing variable fracture patterns.
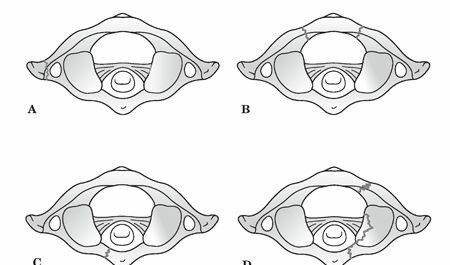
- Classification (Levine) ( Fig. 9.6)
- Isolated bony apophysis fracture
- Isolated posterior arch fracture
- Isolated anterior arch fracture
- Comminuted lateral mass fracture
-
Burst fracture, also known as the Jefferson fracture



- Treatment
- Initial treatment includes halo traction/immobilization.
- Stable fractures (posterior arch or nondisplaced fractures involving the anterior and posterior portions of the ring) may be treated with a rigid cervical orthosis.
-
Less stable configurations (asymmetric lateral mass fracture with “floating” lateral mass, burst
fractures) may require prolonged halo immobilization. - C1–C2 fusion may be necessary to alleviate chronic instability and/or pain.
Atlas Fractures: Spot Symptoms & Get Expert Treatment Insights
Updated: Feb 2026
56 Views
Key Medical Takeaway
Your ultimate guide to Atlas Fractures: Spot Symptoms & Get Expert Treatment Insights starts here. Atlas fractures, also known as atlas fractures atlas, are injuries to the C1 vertebra, typically caused by axial compression. These are rarely associated with neurologic injury but instability often indicates transverse alar ligament insufficiency. Treatment ranges from rigid cervical orthosis for stable types to prolonged halo immobilization or C1–C2 fusion for less stable configurations. They are often linked to other cervical spine fractures.

Keywords