Arthroscopy of the Wrist: Preparation and Techniques
BACKGROUND
Since its inception, wrist arthroscopy has continued to evolve. The initial emphasis on viewing the wrist from the dorsal aspect arose from the relative lack of neurovascular structures as well as the familiarity of most surgeons with dorsal approaches to the radiocarpal joint.Anatomic studies provided a better understanding of both the interosseous ligaments as well as carpal kinematics, which led to the development of midcarpal arthroscopy.Innovative surgeons continue to push the envelope through the development of techniques for treating intracarpal pathology, which in turn has culminated in a plethora of new accessory portals.
ANATOMY




NONOPERATIVE MANAGEMENT
In general, wrist arthroscopy is indicated as a diagnostic technique in any patient with persistent wrist pain that has not responded to an appropriate trial of conservative measures:Nonsteroidal anti-inflammatories and activity modification Cortisone injectionWrist arthroscopy is used as an adjuvant procedure for the treatment of acute fractures of the distal radius or scaphoid or for staging degenerative disorders involving the carpus.
INDICATIONS

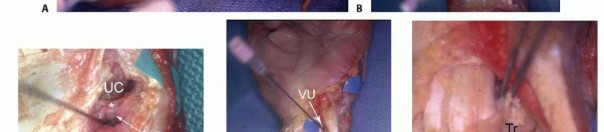

TABLE 1 ARTHROSCOPIC WRIST PROCEDURES
Ganglion resection: volar and dorsal Release of wrist contracture Arthroscopic synovectomyStaging of degenerative arthritis (scapholunate advanced collapse or scaphoid nonunion advanced collapse, Kienbock disease)Radial styloidectomyProximal pole of hamate resection Dorsal radiocarpal ligament repairEvaluation and treatment of carpal instability: scapholunate, lunotriquetral, midcarpal Triangular fibrocartilage tears: repair versus débridementArthroscopic wafer resectionArthroscopic reduction and internal fixation of distal radius fractures Arthroscopic-guided fixation of scaphoid fractures
CONTRAINDICATIONS
Contraindications to the use of dorsal or volar portals would include marked swelling, which distorts the topographic anatomy; large capsular tears, which might lead to extravasation of irrigation fluid; neurovascular compromise; bleeding disorders; or infection.Unfamiliarity with the regional anatomy is a relative contraindication.
SURGICAL MANAGEMENT
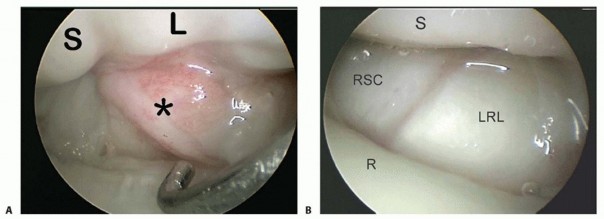
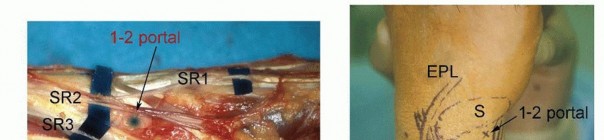
It is useful to have a systematic approach to viewing the wrist.The structures that should be visualized as a part of a standard examination include the radius articular surface; the proximal scaphoid, lunate, and triquetrum; the SLIL and lunotriquetral interosseous ligament (LTIL), both palmar and dorsal; the radioscaphocapitate ligament; the long radiolunate ligament; the radioscapholunate ligament; the ulnolunate ligament; the ulnotriquetral ligament; the articular disc; and the radial and peripheral TFCC attachments.Many procedures can be done without fluid, which minimizes the amount of swelling and fluid extravasation. Intermittentirrigation with a 10-mL syringe attached to the inflow portal of the arthroscope followed by suction with the full radius resector can help clear the field.The volar radial portal is used in patients with radial-sided and dorsal wrist pain to visualize the palmar SLIL and the DRCL.In patients with ulnar-sided wrist pain, the volar ulnar portal is used to assess the palmar LTIL and dorsal radioulnar ligament, the region of the ECU subsheath, and the radial TFCC attachment.The scope is then inserted in the 3-4 portal followed by various combinations of the 4-5 portal and 6R portal. The 6U portal is mostly used for outflow, but it may be used for instrumentation when débriding palmar LTIL tears.Midcarpal arthroscopy is then performed to probe the SLIL and LTIL joint spaces for instability, the capitohamate interosseous ligament, and to look for chondral lesions on the proximal capitate and hamate and loose bodies.The special-use portals such as the dorsal and volar DRUJ portals and the 1-2 portal are used as needed.
PREOPERATIVE PLANNING
A 2.7-mm, 30-degree angled scope along with a camera attachment is used.Table 2 describes the typical field of view as seen through a 2.7-mm arthroscope under ideal conditions.1,3 A 1.9-mm scope is sometimes beneficial, especially for evaluation of the DRUJ.A 3-mm hook probe is needed for palpation of intracarpal structures.A motorized shaver or diathermy unit such as the Oratec probe (Smith & Nephew, New York, NY) is useful for débridement. Ancillary equipment is largely procedure dependent.A motorized 2.9-mm and 3.5-mm burr is needed for bony resection.There are a variety of commercially available suture repair kits, including the TFCC repair kit by Linvatec (ConMed Linvatec, Corp., Largo, FL). Ligament repairs can also be facilitated by use of a Tuohy needle, which is generally found in any anesthesia cart.
POSITIONING
The patient is positioned supine on the operating table with the involved arm abducted on an arm table. A tourniquet is placed as far proximal on the arm as feasible.Traction is useful:A shoulder holder along with 5- to 10-pound sandbags attached to an arm slingA commercially available traction tower such as the Linvatec tower (ConMed Linvatec Corp., Utica, NY) or the ARC traction tower (Arc Surgical LLC, Hillsboro, OR)For the dorsal portals, the surgeon faces the dorsum of the wrist and is seated by the patient's head. For the volar portals, the surgeon faces the palm and is seated in the patient's axillary region.
APPROACH
Portals are established by palpating and identifying anatomic landmarks and then inserting a 22-gauge needle into the joint space. The joint can be injected with 5 mL of saline. The ability to draw the saline back into the syringe serves as evidence that the needle is in the joint. This is not necessary for dry arthroscopy.Shallow incisions avoid injury to sensory nerve branches and tendons. Soft tissues are dissected using a blunt mosquito clamp or a pair of small tenotomy scissors. The dorsal capsule is pierced with these same instruments, providing access to the joint.A blunt trocar is used to introduce the scope cannula, which will house the scope and the inflow.An 18-gauge needle is placed in the 6U portal for outflow, but this is not needed with dry arthroscopy.Synovitis, fractures, ligament tears, and a tight wrist joint may limit the field of view and necessitate the use of more portalsto adequately assess the entire wrist.P.27
TABLE 2 FIELD OF VIEW
Portal|Radial|Central|Volar|Dorsal/Distal|Ulnar---------|---1-2 Scaphoid and lunate fossa, dorsal rim of radiusProximal and radial scaphoid, proximal lunateOblique views of RSC, LRL, SRLOblique views of DRCLTFCC poorly visualized3-4 Scaphoid and lunate fossa, volar rim of radiusProximal scaphoid and lunate, dorsal and membranous SLILRSC, RSL, LRL, ULL Obliqueviews of the DRCLinsertion onto the dorsal SLILTFCC radial insertion, central disc, ulnar attachment, PRUL, DRUL, PTO, PSR4-5 Lunate fossa, volar rim of radiusProximal lunate, triquetrum, dorsal and membranous LTILRSL, LRL, ULL Poorly seen TFCC radialinsertion, central disc, ulnar attachment, PRUL, DRUL, PTO, PSR6R Poorly seen Proximal lunate, triquetrum, dorsal and membranous LTILULL, ULT Poorly seen TFCC radial insertion, central disc, ulnar attachment, PRUL, DRUL, PTO, PSR6U Sigmoid notch Proximal triquetrum, membranous LTILOblique views of ULL, ULTOblique views of DRCLTFCCoblique views of the radial insertion, central disc, ulnar attachment, PRUL, DRULVolar radialScaphoid and lunate fossa, dorsal rim of radiusScaphoid and lunate fossa, dorsal rim of radiusPalmar scaphoid and lunate, palmar SLILOblique views of RSL, LRL, ULLOblique views of the radial insertion,central disc, ulnar attachment, PRUL, DRULMidcarpal radialScaphotrapeziotrapezoidal joint, distal scaphoid poleSLIL joint, distal scaphoid, distal lunateRadial limb of arcuate ligament (ie, continuation of the RSC ligament)Proximal capitate, CHIL, oblique views of proximal hamateLTIL joint, partial triquetrumMidcarpal ulnarDistal articular surface of the lunate and triquetrum and partial scaphoidSLIL joint Volar limb of arcuate ligament (ie, continuation of the triquetrocapitolunate)Oblique views of proximal capitate, CHIL,proximal hamateLTIL joint, triquetrumDorsal distal radioulnar jointSigmoid notch, radial attachment of TFCCUlnar head Palmar radioulnarligamentProximal surface of articular discLimited view of deep DRULVolar distal radioulnar jointSigmoid notch, radial attachment of TFCCUlnar head Dorsal radioulnarligamentProximal surface of articular discFoveal attachment of deep fibers of TFCC (ie, DRUL,PRUL)RSC, radioscaphocapitate ligament; LRL, long radiolunate ligament; SRL, short radiolunate ligament; DRCL, dorsal radiocarpal ligament; TFCC, triangular fibrocartilage complex; SLIL, scapholunate interosseous ligament; RSL, radioscapholunate ligament; ULL, ulnolunate ligament; PRUL, palmar radioulnar ligament; DRUL, dorsal radioulnar ligament; PTO, pisotriquetral orifice; PSR, prestyloid recess; LTIL, lunotriquetral interosseous ligament; ULT, ulnotriquetral ligament; CHIL, capitohamate ligament.Adapted from Slutsky DJ. Wrist arthroscopy portals. In: Slutsky DJ, Nagle DJ, eds. Techniques in Hand and Wrist Arthroscopy. Philadelphia: Elsevier, 2007.
TECHNIQUES
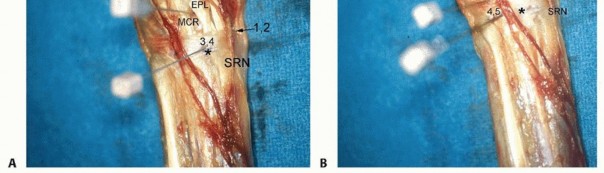
3-4 PORTAL

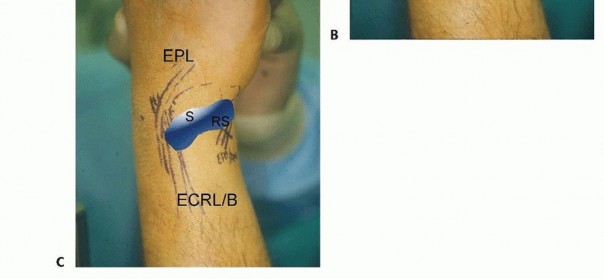
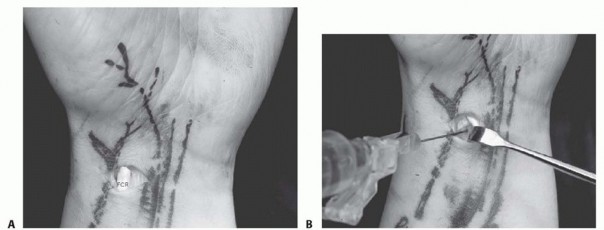
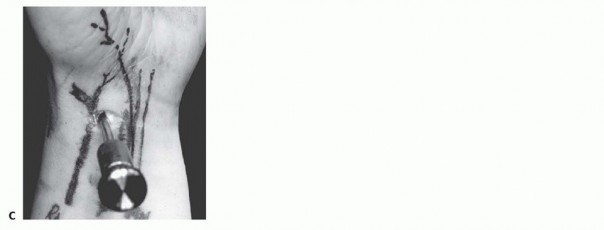
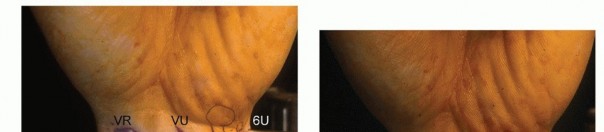
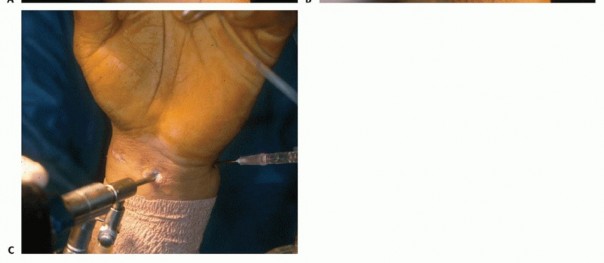
B. Saline injection of radiocarpal joint. C. Insertion of cannula through floor of the FCR sheath. (From Slutsky DJ. Volar portals in wrist arthroscopy. J Am Soc Surg Hand 2002;2:225-232.)

VOLAR DISTAL RADIOULNAR JOINT PORTAL
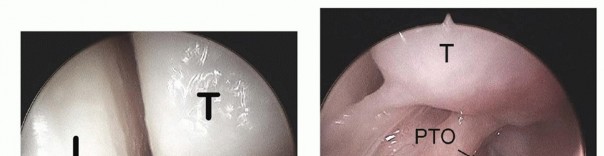
The volar DRUJ portal is accessed through the volar ulnar skin incision ( TECH FIG 7A-E).The joint is entered by angling the 22-gauge needle 45 degrees proximally.It is useful to leave a needle or cannula in the ulnocarpal joint for reference.Alternatively, a probe can be placed in the distal DRUJ portal and advanced through the palmar incision to act as a switching stick over which the cannula can be threaded. 5Initially, the space appears quite limited, but over the course of 3 to 5 minutes, the fluid irrigation expands the joint space, which improves visibility.A 3-mm hook probe is inserted through the dorsal distal DRUJ portal for palpation.A burr or thermal probe can be substituted as necessary.Direct visualization of the foveal attachment prevents accidental injury to this structure. The articular disc is seen superiorly.Proximal surface tears of the TFCC, which are usually caused by severe axial load, may be detected through this portal.The dome of the ulnar head lies inferiorly.The TFCC attachment to the sigmoid notch can be palpated with a hook probe in the distal dorsal DRUJ portal as it penetrates the dorsal DRUJ capsule.The deep attachments of the dorsal radioulnar ligament can be seen as it inserts into the fovea.In ideal cases, the conjoined tendon of the dorsal radioulnar ligament, ulnar collateral ligament, and palmar radioulnar ligament can be visualized.
DORSAL DISTAL RADIOULNAR JOINT PORTAL
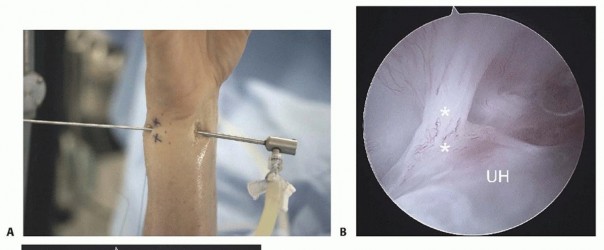
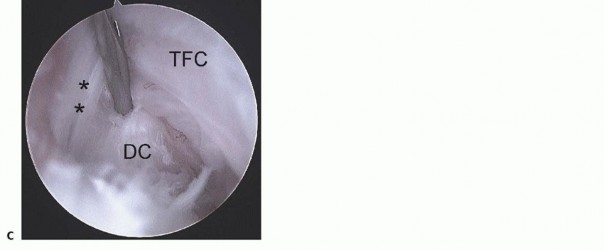
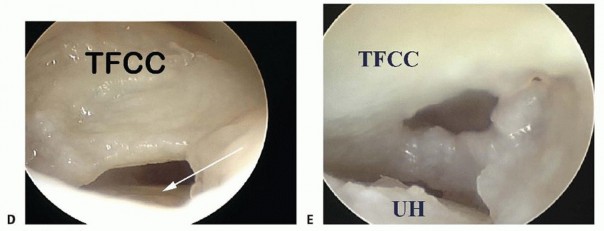
TECH FIG 7 •(continued)D. View of a radial TFC tear from the 4-5 portal under dry arthroscopy. Note the exposure of the ulnar head (arrow).TFCC, triangular fibrocartilage complex. E. View of the same TFC tear from the VDRU.UH, ulnar head.The joint space is entered by inserting a 22-gauge needle horizontally at the neck of the distal ulna.Fluoroscopy facilitates needle placement.The distal dorsal DRUJ portal is identified 6 to 8 mm distally with the 22-gauge needle and just proximal to the 6R portal.This portal can be used for outflow drainage or for instrumentation.It lies on top of the ulnar head but underneath the TFCC and so is difficult to use in the presence of positive ulnar variance.The TFCC has the least tension in neutral rotation of the forearm, which is the optimal position for visualizing the articular dome of the ulnar head, the undersurface of the TFCC, and the proximal radioulnar ligament from its attachment to the sigmoid notch to its insertion into the fovea of the ulna.Because of the dorsal entry of the arthroscope, the course of the dorsal radioulnar ligament is not visible until its attachment into the fovea is encountered.Entry into this portal provides views of the proximal sigmoid notch cartilage and the articular surface of the neck of the ulna.
PEARLS AND PITFALLS
- Use shallow skin incisions.
- Use the wound spread technique to protect surrounding sensory nerves.
- If the trocar does not insert easily, reposition to avoid chondral injury.
- Wrist traction often diminishes during the procedure and should be readjusted as needed to avoid scraping the articular surface.
- Use of a standard methodologic approach ensures a complete and thorough examination.
POSTOPERATIVE CARE
The postoperative rehabilitation depends on the specific procedure that is performed.After diagnostic arthroscopy, with or without débridement, the patient is splinted for comfort for a brief period of 4 to 7 days.Active wrist motion is encouraged after this period and patients are allowed activities of daily living, followed by gradual strengthening.If a ligament repair or TFCC repair has been performed or if there is interosseous pinning, the protocol is adjusted as necessary and typically involves an initial period of immobilization before instituting wrist motion.
COMPLICATIONS
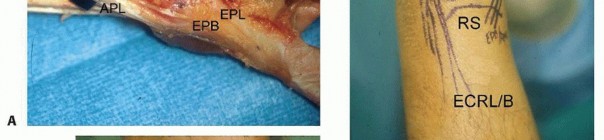
Most of the complications related to use of the dorsal portals are related to injury to the sensory branches of the superficial radial nerve and the dorsal cutaneous branch of the ulnar nerve.The palmar cutaneous branch of the ulnar nerve is at risk with the volar radial portal, although the interposed FCR tendon mitigates this risk.There is no true internervous plane when using the volar ulnar portal; hence, sensory branches of the palmar cutaneous branches of the ulnar nerve or nerve of Henle are always at risk. Thus, proper wound spread technique is paramount.The ulnar neurovascular bundle is also potentially at risk with overzealous retraction or poor portal placement.P.34Venous bleeding, loss of wrist motion (especially forearm supination), complications related to fluid extravasation, and infection are general risks attendant to any arthroscopic procedure.These can be minimized by fastidious surgical technique, aggressive rehabilitation as necessary, and diligent followup in the early postoperative period.
REFERENCES
- Berger RA. Arthroscopic anatomy of the wrist and distal radioulnar joint. Hand Clin 1999;15(3):393-413.
- Geissler WB, Freeland AE, Savoie FH, et al. Intracarpal soft-tissue lesions associated with an intra-articular fracture of the distal end of the radius. J Bone Joint Surg Am 1996;78(3):357-365.
- Slutsky DJ. Arthroscopy portals: volar and dorsal. In: Budoff J, Slade JF, Trumble TE, eds. Master's Techniques in Wrist and Elbow Arthroscopy. Chicago: American Society for Surgery of the Hand, 2006.
- Slutsky DJ. Clinical applications of volar portals in wrist arthroscopy. Tech Hand Up Extrem Surg 2004;8(4):229-238.
- Slutsky DJ. Distal radioulnar joint arthroscopy and the volar ulnar portal. Tech Hand Up Extrem Surg 2007;11:38-44.
- Slutsky DJ. Management of dorsoradiocarpal ligament repairs. J Am Soc Surg Hand 2005;5:167-174.
- Slutsky DJ. Volar portals in wrist arthroscopy. J Am Soc Surg Hand 2002;2:225-232.
- Slutsky DJ. Wrist arthroscopy portals. In: Slutsky DJ, Nagel DJ, eds. Techniques in Hand and Wrist Arthroscopy. Philadelphia: Elsevier, 2007.
- Slutsky DJ. Wrist arthroscopy through a volar radial portal. Arthroscopy 2002;18:624-630.
- Steinberg BD, Plancher KD, Idler RS. Percutaneous Kirschner wire fixation through the snuff box: an anatomic study. J Hand Surg Am 1995;20:57-62.
- Viegas SF. Midcarpal arthroscopy: anatomy and portals. Hand Clin 1994;10(4):577-587.
